

INTRODUCTION
Chronic hepatitis C virus (HCV) infection is one of the major causes of chronic hepatitis, cirrhosis, and hepatocellular carcinoma.1,2 The prevalence of HCV infection varies geographically, with the majority of infected people (about 90 million) originating from Asian countries.3 Despite the high burden of HCV disease among Asians, very little is known about the treatment outcomes in these patients because most of the pivotal studies only included small numbers of Asian patients.4-6
The standard-of-care treatment for patients with chronic hepatitis C (CHC) has been combination of peginterferon (PEG-IFN) and ribavirin (RBV), which induces sustained virological response (SVR) rates of 40-50% in cases with HCV genotype 1, and of 80% or more in cases with genotype 2 or 3 infections.4-6 The recent development of protease inhibitors has substantially improved the SVR rates of patients with genotype 1.7,8 However, given the high cost and the more frequent occurrence of adverse events associated with triple combination therapy with PEG-IFN, RBV, and protease inhibitor, it is important to identify who would benefit the most from this therapy.
Although the HCV genotype is known to be the strongest predictor of SVR, several host genetic factors have also been found to affect the response to treatment. Recent studies have revealed that the likelihood of achieving an SVR with PEG-IFN and RBV depends on the nucleotide sequence near the interleukin (IL) 28B gene.9-11 Interestingly, the frequency of the favorable IL 28B allele is substantially higher in East Asians.9,10 Notably, several earlier studies have demonstrated that Asian patients are more likely to achieve SVR than Caucasians.12-16 However, contradicting the earlier reports described above, several recent studies have found that Asians have similar or even inferior SVR rates compared to Caucasian patients with the same HCV genotype.17-20
When comparing data from different studies, the study design and methods of analysis should be considered. Real-world effectiveness data derived from ordinary clinical practice settings often differ markedly from the efficacy data obtained in the settings of randomized controlled registration trials.21-23
We assessed the effectiveness of PEG-IFN α-2a and RBV therapy in treatment-naïve Korean patients with CHC and who had accurately diagnosed HCV genotype 1, 2, or 3.
PATIENTS AND METHODS
Patients
The study population was recruited from two groups of treatment-naïve patients with CHC who were treated with the PEG-IFN α-2a plus RBV combination. One group consisted of 100 patients in a prospective, industry-sponsored, open-label, uncontrolled, community-based clinical trial (Pegasys Expanded Access Program) conducted at six tertiary referral centers in Korea between 2003 and 2004 (Clinical Trial group). The second group consisted of 522 patients who were treated in a single tertiary referral hospital (Asan Medical Center, Seoul, Korea) between 2004 and 2008 (Cohort group).
Eligible patients were previously untreated adults aged 18-70 years who had polymerase chain reaction (PCR)-detectable HCV ribonucleic acid (RNA) and compensated liver disease. Patients were excluded if they had any of the following: a HCV genotype other than 1, 2, or 3; acute hepatitis C; decompensated cirrhosis; hepatocellular carcinoma; other forms of liver disease. Patients with human immunodeficiency virus, pre-existing severe depression or other psychiatric disease, previous organ transplantation, absolute neutrophil count (ANC) <1,000 cells/mm3, platelet count <75,000 cells/mm3, or hemoglobin (Hb) <13 g/dL for men or <12 g/dL for women were also excluded. Cirrhosis was based on the histological diagnosis in Clinical Trial group, and on histological or radiological diagnosis in Cohort group. All study patients were of Korean ethnicity. This study was approved by the Institutional Review Board at each participating center
Treatment protocol
The HCV genotype was determined by using the restriction fragment mass polymorphism (RFMP) assay. Patients with genotype 1 were treated with PEG-IFN α-2a (Roche, Basel, Switzerland) 180 µg/week and a daily RBV (Roche for the Clinical Trial group; Shinpoong, Korea for the Cohort group) dose of 1,000 mg (for patients with body weight <75 kg) or 1,200 mg (for patients with body weight ≥75 kg) for 48 weeks. Patients with genotype 2 or 3 were treated with PEG-IFN α-2a 180 µg/week and a daily RBV dose of 800 mg for 24 weeks. All study medications for the patients in the Clinical Trial group were provided by Roche, whereas the Cohort group patients purchased their medications. HCV RNA was quantified (Roche AMPLICOR HCV Test v2.0) at pretreatment, weeks 12, 24 and 48 for both genotypes and at week 72 for genotype 1.
Dose modification and definition of adherence
In the Clinical Trial group, if ANC dropped below 750 cells/mm3, PEG-IFN α-2a was reduced to 135 µg. If ANC fell below 500 cells/mm3, PEG-IFN α-2a was stopped until ANC recovered to 1,000 cells/mm3, and the restarting of medication was initiated from 90 µg. If platelet counts dropped below 50,000 cells/mm3, PEG-IFN α-2a was reduced to 90 µg. If platelet counts fell below 25,000 cells/mm3, the discontinuation of administration was recommended. The RBV dose was reduced if Hb decreased to <10 g/dL and stopped if Hb decreased to <8.5 g/dL.
In the Cohort group, the dose modification depended on the decision of the physician, which was based on laboratory data and clinical information and referred to the guidelines used in the clinical trial. The information about the amount of each drug administered to a patient was obtained from the drug dispensing/return or prescription records.
None of the patients in either group were treated with growth factors for hematological side effects.
Adherence ≥80/80/80 was defined when a patient was treated for ≥80% of the assigned treatment duration and received ≥80% of both PEG-IFN α-2a and RBV doses.
Main outcome measures
The primary outcome of interest in this study was the proportion of patients who achieved SVR, which was defined as documented PCR-undetectable serum HCV RNA levels at 24 weeks after cessation of treatment. Secondary outcomes included early virological response (EVR, reduction of HCV RNA levels by 2 log or more at 12 weeks of treatment), complete EVR (cEVR, PCR-undetectable HCV RNA at 12 weeks of treatment), and end-of-treatment response (ETR, HCV RNA undetectable at the end of treatment).
Statistical analysis
All response evaluations and adherence to treatment were assessed by modified intention-to-treat analysis unless specified (i.e., all patients who received at least one dose of medication were included in the analysis).
Between-group comparisons of continuous variables were determined by using independent t-tests, and categorized variables were compared by using the chi-square test or Fisher's exact test, as appropriate. The predictive factors for SVR were analyzed by logistic regression. A P-value less than 0.05 was considered to be statistically significant in all analyses. Statistical analyses were performed by using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
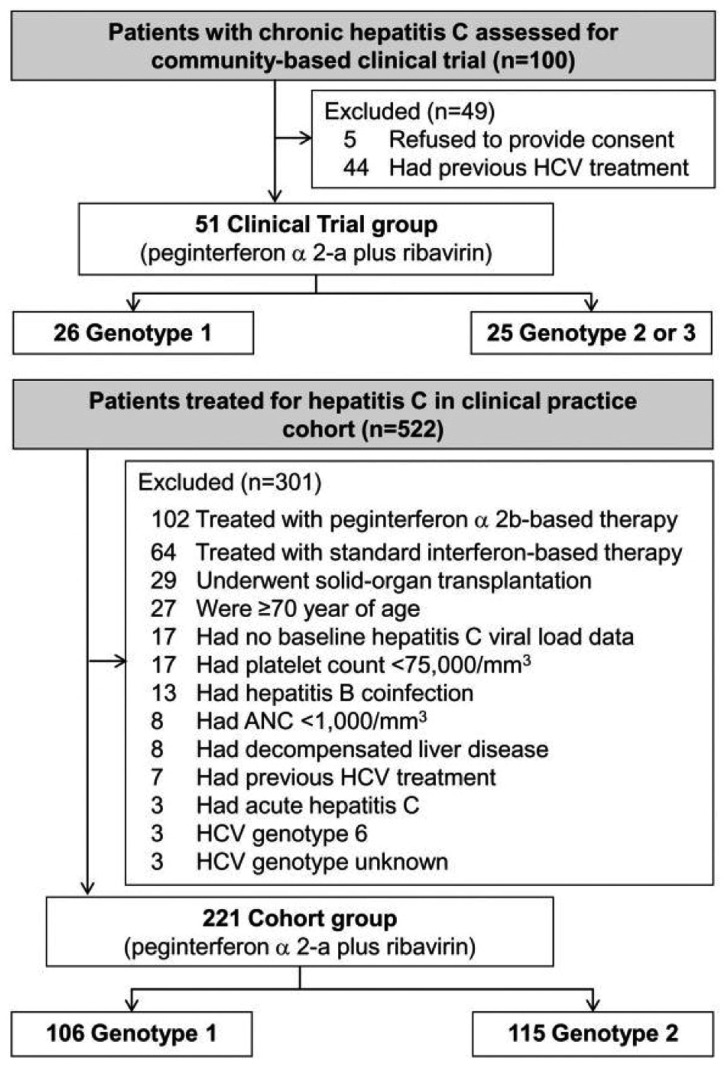
For the Clinical Trial group, 100 patients with CHC were assessed: 5 refused to provide consent and 44 had previous treatment; thus, 51 treatment-naive patients were included in intention-to-treat analysis. Of these, 26 and 25 had genotype 1 and genotype 2 or 3, respectively (Fig. 1).
In the Cohort group, 522 consecutive patients with HCV were assessed: 301, including three patients with HCV genotype 6, did not meet the enrollment criteria and were excluded. The remaining 221 eligible patients were included in intention-to-treat analysis. Of these, 106 and 115 had genotype 1 and genotype 2, respectively (Fig. 1).
The Clinical Trial and the Cohort group were similar in most baseline characteristics (Table 1). However, the Clinical Trial group had a higher serum ALT levels than the Cohort group (P=0.03 and P<0.01 for genotypes 1 and 2, respectively). Of those with genotype 2, the Cohort patients were more likely to have cirrhosis than the Clinical Trial patients (0% vs. 21.7%, P<0.01).
Virological responses and adherence to treatment
In patients with genotype 1, the Clinical Trial and Cohort group did not differ in the proportion of patients who achieved EVR, cEVR, and ETR (EVR: 84.6% vs. 80.2%, P=0.78; cEVR: 84.6% vs. 73.6%, P=0.24; ETR: 92.3% vs. 80.2%, P=0.25; Table 2). However, the Clinical Trial grouP had a significantly higher SVR rates than the Cohort group (80.8% vs. 54.7%, P=0.02). The Clinical Trial group also had a significantly higher proportion of patients with treatment duration ≥80% than the Cohort group (96.2% vs. 69.8%, P=0.01). However, the difference in the proportion of patients with adherence ≥80/80/80 was not significant between the two groups (53.8% vs. 38.7%, P=0.16).
In patients with genotype 2, the Clinical Trial group had significantly higher EVR and cEVR rates than the Cohort group (EVR: 92.0% vs. 72.2%, P=0.04; cEVR: 92.0% vs. 71.3%, P=0.03; Table 2). However, the two groups did not differ in terms of ETR and SVR rates (ETR: 96.0% vs. 96.5%, P=1.00; SVR: 96.0% vs. 87.8%, P=0.31, respectively). The Clinical Trial group had a significantly higher proportion of patients with a treatment duration ≥80% than the Cohort group (100% vs. 80.0%, P=0.01). However, the two groups were similar in the proportion of patients with adherence ≥80/80/80 (72.0% vs. 67.8%, P=0.68).
Predictive factors for SVR
In patients with genotype 1, univariate analysis showed that age, cirrhosis, treatment in the Clinical Trial, achievement of EVR, treatment duration ≥80%, and adherence ≥80/80/80 were significantly associated with the achievement of SVR (Table 3). Of these significant factors, age (odds ratio [OR]=0.95, 95% confidence interval [CI]=0.92-0.99, P=0.02), treatment in the Clinical Trial (OR=4.94, CI=1.38-17.7, P=0.01), achievement of EVR (OR=5.33, CI=1.62-17.52, P<0.01), and adherence ≥80/80/80 (OR=4.67, CI=1.82-12.0, P<0.01) were independently associated with SVR by multivariate analysis.
In patients with genotype 2, univariate analysis showed that age, cirrhosis, achievement of EVR, treatment duration ≥80%, and adherence ≥80/80/80 were significantly associated with SVR. Multivariate analysis revealed that only cirrhosis (OR=0.17, CI=0.05-0.63, P<0.01) and treatment duration ≥80% (OR=8.16, CI=2.29-29.13, P<0.01) were independently associated with SVR.
SVR rate as a function of EVR and adherence
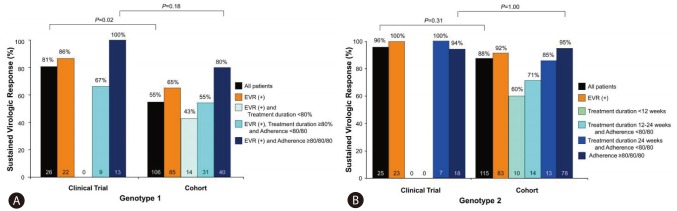
SVR rate as a function of the amount of treatment received was assessed at different adherence levels to determine any relationship between adherence and sustained response. As shown in Fig. 2, we found a stepwise, increasing relationship between adherence and SVR in either Clinical Trial or Cohort group regardless of HCV genotype. Thus, in genotype 1 patients with treatment duration ≥80%, at least 80% adherence to therapy increased SVR rates from 66.7% to 100% for those in Clinical Trial group and from 54.8% to 80.0% for those in Cohort group (Fig. 2A). In genotype 1 patients who achieved EVR and adherence ≥80/80/80, the SVR rate was not significantly different between the Clinical Trial and Cohort groups (100% vs. 80.0%, P=0.18).
In patients with genotype 2, the stepwise, increasing relationship between adherence and SVR was observed only in Cohort group (Fig. 2B).
Causes of non-adherence
When the genotype 1 and 2 patients were combined, 19 of the 51 Clinical Trial patients (37.3%) and 102 of the 221 Cohort group patients (50.7%) did not show adherence ≥80/80/80 (Table 4). Overall, the most common cause of non-adherence in both groups was laboratory abnormalities, including anemia and neutropenia. However, the two groups differed significantly in terms of the distribution of the causes of non-adherence (P<0.01): compared to the Clinical Trial group, laboratory abnormalities were a significantly less frequent cause of non-adherence in the Cohort group (89.5% vs. 50.0%, P<0.01), while adverse symptoms were a more frequent cause (10.5% vs. 34.3%, P=0.04).
DISCUSSION
In the present study, we tried to adequately address all issues in assessing the treatment response in CHC patients including heterogeneity in ethnicity of patients, prior treatment-experience, errors in HCV genotyping, study design, and dataset for endpoint analysis. Thus, we clearly demonstrate that treatment-naïve Korean patients with CHC achieve high SVR rates with PEG-IFN α-2a plus RBV therapy in both the community-based clinical trial and the clinical practice settings. For patients with HCV genotype 1, the overall SVR rates of the Clinical Trial and the clinical practice Cohort group were 80.8% and 54.7%, respectively, by an intention-to-treat analysis. The SVR rates of the Clinical Trial and the Cohort group increased to as high as 100% and 80.0%, respectively, when a per-protocol analysis was applied (i.e., in patients with EVR and adherence ≥80/80/80). For patients with genotype 2, the overall SVR rates of the both groups were 96.0% and 87.8%, respectively.
The SVR rates of this real-world effectiveness study in East Asian patients with CHC are higher than the SVR rates of published randomized controlled registration trials that employed a similar regimen and duration of treatment and mainly included Caucasian patients.4,5 In the latter trials, the overall SVR rates ranged between 46% and 52% for genotype 1 patients and between 76% and 80% for genotype 2 or 3 patients. The SVR rate of 81% in our Clinical Trial group and 80% of treatment-adherent patients in our clinical practice Cohort group with HCV genotype 1 were even higher or comparable to the results from recent registration trials on triple combination therapy with boceprevir or telaprevir, PEG-IFN, and RBV.7,8
The high effectiveness of PEG-IFN and RBV therapy in our patients with CHC are interesting because patients treated in community practices generally have lower, or similar at best, response rates compared to those in registration trials; this is due to the inclusion of a broader spectrum of patients, less frequent monitoring, lack of financial support, low insurance coverage, and lower adherence to treatment.21,23-26 Thus, the data of this study strongly suggest that East Asian patients with CHC are more responsive to PEG-IFN plus RBV therapy than Caucasian patients.
The results of this study are consistent with those of several previous clinical trials and cohort studies, which showed that Asian patients with CHC have higher SVR rates when directly compared to Caucasian patients.12-16 As we and others have found, the vast majority (82-100%) of Asians who had EVR also achieved cEVR, whereas only about half of Caucasians with EVR achieved cEVR.17 These results suggest that a higher proportion of the Asian subjects in the present study were rapid virological responders, and as a result, they had lower rates of breakthrough or relapse and a higher SVR rate.
Recent understanding for the effect of IL-28B gene-related single nucleotide polymorphisms on response to PEG-IFN and RBV treatment may provide the biological basis for the racial differences in viral kinetics during treatment.9,11 Patients with the C/C genotype showed a greater decline in HCV RNA during first 4 weeks of treatment when compared to patients with non-C/C genotypes, irrespective of race,27 and that the C/C genotype is also associated with a three times higher probability of SVR than the C/T and T/T genotypes combined.9,27 Geographical variation in the IL28B gene supports the notion that East Asian patients should have higher response rates as they have a higher frequency of the C/C genotype than their white European counterparts.9,10,28,29
In contrast to our results, others have recently demonstrated that Asians have similar or even inferior SVR rates compared to Caucasian patients with the same HCV genotype.17-20 They suggested that the SVR rates in Asians in the earlier studies were erroneously inflated by the possible inclusion of easier-to-treat genotype 6 patients in the genotype 1 group. Supporting this is that the earlier studies used the INNO-LiPA probe assay for HCV genotyping which may mistype genotype 6 as genotype 1. This is a plausible possibility because up to one-third of HCV-infected patients from Southern China and Southeast Asia are estimated to have HCV genotype 6.30 However, the mistyping error was eliminated from our study because we used the RFMP genotyping assay, which accurately differentiates HCV genotype 6 from genotype 1.31 A bias might also have arisen by including diverse ethnic groups as a single Asian race in previous studies. Each of Asian ethnic groups encompasses diverse genetic backgrounds, and racial classifications do not convey genetic homogeneity.13,15 For example, grouping subjects from Indian sub-continent and East Asia as Asians may introduce bias, as genetic heterogeneity may exist between these groups.19 By including only a single East Asian ethnic group, this kind of selection bias could be avoided in this study.
Adherence to treatment was an independent determinant of the achievement of SVR in this study. The importance of adherence on SVR rates has been well described previously.25,32-35 We also found that adherence to treatment was more important for patients with genotype 1 than those with genotype 2, and adherence tended to be lower in the Cohort group than in the Clinical Trial group. Accordingly, the overall SVR rate for genotype 1 patients in the Cohort group was lower than patients in the Clinical Trial group. However, this difference disappeared when the outcome of only the patients with a high level of adherence was evaluated. These results suggest that measures to raise adherence to standard treatment in East Asian patients with CHC would be more costeffective way to improve the overall SVR rate than adding protease inhibitors, especially in clinical practice settings.
The most common cause of non-adherence was dose reduction due to laboratory abnormalities. Asians seem to be much more likely to undergo RBV dose reductions and discontinuations of treatment because of anemia.16,17 Hence, it is possible that the use of growth factors may be particularly beneficial for Asian patients in terms of improving adherence to treatment and SVR in clinical practice.24
Treatment-related adverse symptoms were more frequent cause of non-adherence in the Cohort group compared with Clinical Trial group. Although it is unclear whether the dose reduction or treatment discontinuation was patient-initiated or physician-instructed, the importance of the role of health care providers should not be overlooked. Previous studies have reported that decreased drug exposure due to physician-directed dosage reductions of interferon and RBV can reduce virologic response rates.33-36 In addition to the physician experience, the role of a dedicated physician assistant who provides education and support to patients undergoing hepatitis C therapy has been suggested to be important.24,37 Unfortunately, we did not have such a physician assistant during the period of this study, which might have contributed to the low adherence in our clinical practice cohort patients.
The main limitation of our study is its retrospective design. However, we used the standard definition of SVR as our primary endpoint which is an objective and well-defined outcome variable. Moreover, all results were analyzed according to the intention-to-treat method. Second, there is a possibility of type 2 error, that is, the small number of Clinical Trial group may fail to show the significant difference in the SVR rate between the Clinical Trial group and the Cohort group in per-protocol analysis (100% vs. 80%) in genotype 1 and in intention-to-treat analysis and per protocol analysis in genotype 2 (96% vs. 88%, and 94% vs. 95%, respectively). However, the SVR rate was already near the maximum level of 100% in the Clinical Trial group, thus, there is low possibility to discriminate the significant difference by increasing the sample size of the Clinical Trial group. Third, since our study only included patients of a single Asian ethnicity, we were not able to compare our results directly to those of Caucasian patients. Lastly, since few patients had HCV RNA quantitation data at treatment week 4, we could not analyze the impact of a rapid virological response on the achievement of SVR.
In conclusion, our study highlights the importance of ethnicity as an integral component of the tailored treatment approach to CHC. Our results also emphasize the need to enhance adherence to HCV therapies. With adequate adherence to PEG-IFN α-2a plus RBV treatment, Korean patients with HCV genotype 1 could achieve similar or even higher SVR rate than that can be achieved by Caucasian patients with triple combination therapy including protease inhibitors. Thus, measures to raise adherence to the standard therapy in clinical practice may improve the SVR rates in East Asian CHC patients as effectively as adding protease inhibitors.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




