

INTRODUCTION
The red cell distribution width (RDW), which a measure of anisocytosis, has traditionally been used in the differential diagnosis of anemia.1 Recent studies, however, have reported that RDW is associated with increased mortality in many clinical conditions2 and found that high RDW is associated with an increase in allcause mortality. The most plausible explanations for those associations are chronic inflammation and oxidative stress, which leads to an elevation in RDW.3-5
Nonalcoholic fatty liver disease (NAFLD) includes a wide spectrum of liver damage ranging from simple steatosis to non-alcoholic steatohepatitis (NASH), advanced fibrosis, and hepatocellular carcinoma.6,7 Likewise, the association with chronic inflammation and oxidative stress though to be proximate mediating mechanisms of more advanced fibrosis in NAFLD.6 We hypothesized that a common interaction of the aforementioned pathophysiological processes might be link RDW with degree of fibrosis in NAFLD.
We used two simple noninvasive fibrosis scores for evaluating advanced fibrosis of NAFLD. One is the BARD score, which is used to rule out hepatic fibrosis in patients with NAFLD, is composed of three variables (BMI ≥25 is 1 point, AST/ALT ratio (AAR) ≥0.8 is 2 points, and type 2 diabetes mellitus is 1 point) is usually readily available and very easy to estimate.8 And another one is FIB-4 score was calculated according to the following formula: age (years)×AST [IU/L]/platelet count [expressed as platelets×109/L]×(ALT [IU/L]).1,2,9
The goal of the present study is to investigate whether RDW values differ between the lower BARD and FIB-4 score group and the higher BARD and FIB-4 score group, and to consider the role of RDW as a predictive marker for the advanced fibrosis in NAFLD.
METHODS
Study population
A total of 110,978 subjects (63,729 men and 47,249 women) who presented for a routine health maintenance exam at Kangbuk Samsung Hospital (Sungkyunkwan University School of Medicine) between January 1 and December 30, 2010 were included in this study. In addition to obtaining a complete medical history and physical examination, which included waist circumference, all 110,978 subjects underwent an abdominal ultrasound and had blood drawn to determine serum levels of viral markers. The exclusion criteria were based on potential other causes for hepatic injury, steatosis, and/or fibrosis that might confound the data. Thus, subjects were excluded from this study based on: (a) no evidence of hepatic steatosis on ultrasonography (n=77,684); (b) consumption of alcohol ≥20 g per day (n=6,435); (c) antibody to hepatitis C (anti-HCV) positivity (n=67) or hepatitis B surface antigen (HBsAg) positivity (n=1,808); and (d) a history of past or current malignancy (n=93). Additionally, 343 individuals with abnormal abdominal ultrasonography results (evidence of malignancy or cirrhosis) were excluded. Cirrhosis really whether caused by NAFLD is difficult to prove consequently, were excluded. Thus, the final number of subjects available for study was 24,547, which was comprised of 20,008 men and 4,539 women.
Laboratory measurements
All subjects had fasted overnight before they were seen by physicians in clinic. Their height and weight were determined, and their body mass index (BMI) was expressed as weight (kg) divided by the square of the height (m2). Blood samples were collected and a complete blood count was measured by an automated laser-based hematology analyzer (Advia 2120; Siemens Healthcare Diagnostics, Deerfield, Ill). White blood cell count, platelet count, hemoglobin, mean corpuscular volume (MCV), and RDW were all recorded. The fasting glucose level was measured using the hexokinase method. HBsAg and antibody to hepatitis B surface antigen (anti-HBs) were measured by a chemiluminescent microparticle immunoassay (CMIA) (Architect i2000 SR, Abbott, IL, USA). HCV Ab was measured by polymerase chain reaction (PCR) (COBAS AMPLICOR, Roche, Basel, Switzerland). An enzymatic calorimetric test was used to measure the total cholesterol (TC) and triglyceride (TG) concentrations. The selective inhibition method was used to measure the level of high-density lipoprotein cholesterol (HDL-C) and a homogeneous enzymatic calorimetric test was used to measure the level of low-density lipoprotein cholesterol (LDL-C) (Advia 1650 Autoanalyzer, Byer Diagnostics Leverkusen Germany). High sensitivity C-reactive protein (hs-CRP) was analyzed by performing particle-enhanced immunonephelometry with using the BNTM System (Dade Behring, Marburg, Germany). This result was presented in mg/L, and the minimum detectable hsCRP level was 0.175 mg/L after performing a 1:20 sample dilution.
Abdominal ultrasonography
Abdominal ultrasonography (ASPEN; Acuson, PA, USA) was performed by experienced radiologists who were blinded to clinical presentation and laboratory findings. The diagnosis of fatty liver was made using the following criteria: a diffuse hyper-echoic echotexture, hepatorenal echo contrast in reference to the cortex of the right kidney, vascular blurring, and deep-echo attenuation.10,11
Degree of liver fibrosis assessment by the BARD score and FIB-4 score
The BARD score is composed of 3 variables: an AST/ALT ratio ≥0.8 is 2 points, a BMI ≥25 is 1 point, and the presence of diabetes mellitus is 1 point. Thus, the possible score ranges from 0 to 4 points.12 According to the results by Harrison et al, a score values of 0 or 1 has a high negative predictive value (NPV) for severe hepatic fibrosis and a score of 2-4 was associated with an OR for advanced fibrosis of 17 (confidence interval 9.2 to 31.9).12
The FIB-4 score was calculated according to the following formula: age×AST (IU/l)/platelet count (×109/L)×√ALT (IU/L). And the FIB-4 score can reliably exclude advanced fibrosis and lead to the avoidance of liver biopsy in more than 60% of patients with NAFLD and normal or elevated ALT levels, it might be an appropriate score to triage patients with NAFLD into those who have a low probability of advanced fibrosis and those who need further investigation.13
Statistical analysis
Statistical analysis of the data was performed by Statistical Package for Social Sciences (SPSS) version 18 software (SPSS Inc., Chicago, IL, USA). The Shapiro-Wilk test was used to determine whether the continuous variables were normally distributed. Descriptive statistics are displayed as means±standard deviation for normally distributed variables and as medians with interquartile ranges for non-normally distributed variables. RDW quartiles were generated for the overall population based on its distribution. Baseline characteristics were then compared across these quartiles using One-way analysis of variance (ANOVA) or Kruskal-Wallis tests were used for continuous variables, whereas a Fisher's exact test was used to test differences among the RDW quartiles. RDW values in the BARD score and FIB-4 score groups were compared using a one-way analysis of covariance (ANCOVA) test. Differences in subgroups were tested using a Tu key HSD test. Pearson correlation coefficients were used to test univariate correlations for BARD and FIB-4 score with some inflammatory markers. A P-value of less than 0.05 was considered to be statistically significant in this study.
To estimate overall odds for higher BARD score (2-4) and higher FIB-4 score (>1.3), multivariate adjusted logistic regression analysis was performed adjusting for age, sex, hemoglobin level, MCV, hsCRP, history of smoking, history of diabetes and history of hypertension.
Ethics statement
The analysis of data was approved by the Institutional Review Board of Kangbuk Samsung Hospital, which confirmed that the study was in accordance with the ethical guidelines of the Helsinki Declaration. All participants provide their written informed consent to participate in this study. and our ethics committees approve this consent procedure.
RESULTS
Table 1 shows patient baseline characteristics distribution across the quartiles of RDW. Most of the demographic, anthropometric, and biochemical characteristics were comparable between the groups. FIB-4 score and high BARD score (2,3 and 4 respectively) increased in relation to increasing RDW (p for trend <0.001) whereas, low BARD score (0-1) decreased with increasing RDW. Age, BMI, HbA1c, Diabetes and hypertension increased with increasing RDW. Mean FIB-4 score was 0.80±0.34 in Q1, 0.83±0.35 in Q2, 0.85±0.36 in Q3 and 0.86±0.46 in Q4 (P<0.001).
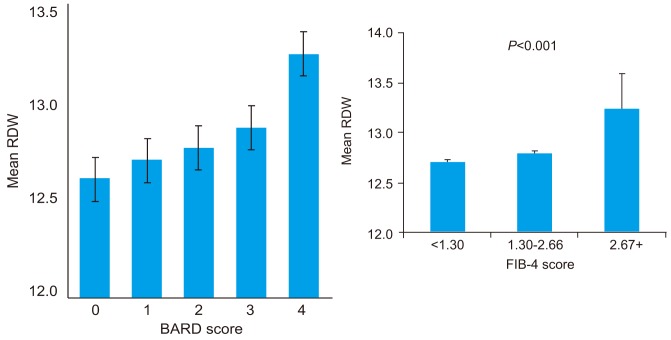
Higher RDW values indicate greater variation in size. In the case of folate and vitamin B12 deficiency anemia, iron deficiency anemia, old age and various cardiovascular disease, causing the RDW to be elevated.14,15 After adjusting for age, sex, hemoglobin level, MCV, hsCRP, history of smoking, history of diabetes and history of hypertension, mean RDW values were 12.61±0.41, 12.70±0.70, 12.77±0.62, 12.87±0.82 and 13.25±0.90 in BARD score 0, 1, 2, 3, and 4 groups, respectively and 12.71±0.72, 12.79±0.66 and 13.23±1.52 in FIB-4 score <1.30, 1.31-2.66 and ≥2.67 groups, respectively (P<0.05 ANCOVA) and (Fig. 1).
Table 2 shows the correlation coefficients between several inflammatory markers and BARD and FIB-4 score. RDW and ferritin were found to be significantly correlated with BARD and FIB-4 score.
Table 3 and Table 4 shows some metabolic components and inflammatory markers distributed according to low and high BARD score and FIB-4 score. High BARD score group was older, had lower body mass index and diabetes, hypertension increased. High FIB-4 score was older but diabetes and hypertension was decreased.
As shown in Table 5, a graded increase in proportion of having advanced fibrosis (BARD score 2-4 and FIB-4≥1.3) with increasing quartiles of RDW(51.1% in Q1 vs. 63.6% in Q4 on BARD score and 6.9% in Q1 vs. 10.5% in Q4 on FIB-4 score, P<0.001) was observed. RDW as a categorical variable (adjusted OR: 1.76, 95% CI: 1.55-2.00 in BARD score and 1.69, 95% CI: 1.52-1.98 in FIB-4 score, P<0.001) remained a statistically significant predictor of advanced fibrosis (BARD score 2-4 and FIB-4≥1.3) in model 3 and 4.
DISCUSSION
In this retrospective study we demonstrated that an increased RDW, which is a simple morphologic marker of red blood cell size heterogeneity, was associated with advanced fibrosis in NAFLD patients. This association remained significant even after adjusting for patient demographics and laboratory parameters.
The mechanism by which elevated RDW values are associated with increased NAFLD fibrosis is unknown. An elevation in the RDW may occur during conditions of ineffective red blood cell production (iron deficiency, B12 or folate deficiency, and hemoglobinopathies), increased red blood cell destruction (hemolysis), or after blood transfusions.16,17 Additionally, proinflammatory cytokines have been shown to inhibit erythropoietin-induced erythrocyte maturation. Thus, inflammation could lead to anisocytosis via release of immature red blood cells into the peripheral circulation.18-20
Several non-invasive methods have been used to identify advanced fibrosis in patients with NAFLD.21 All of them show a greater utility in suggesting the absence of advanced fibrosis rather than predicting the presence of it. Considering the similarity of results between the scoring systems, we used the BARD score and FIB-4 score, which is easier to apply in clinical practice, to identify patients without severe liver fibrosis in this study.8 In the study by Harrison et al a low BARD score (0 or 1 point) had a very compelling negative predictive value (96%) in identifying patients without advanced fibrosis,12 while the positive predictive value of a high score was not as high (43%)
Fibroscan is also a noninvasive test, it can be performed at the point of care, there is no pain, and sedation is not required. Also, the test takes only 5-7 minutes to perform, it is significantly less expensive than liver biopsy, and it has not been associated with any side effects. But technical limitations of the test preclude its use in patients who have ascites, individuals who are morbidly obese, and/or patients who have large amounts of chest wall fat. In these groups, either the test cannot be performed or the results are not reliable.22 Several other noninvasive methods can be used to measure liver stiffness. One radiologic method for measuring liver fibrosis is magnetic resonance (MR) elastography. The advantage of MR elastography is that it is very accurate for measuring liver stiffness; however, this test requires patients to undergo an MR imaging scan, and therefore it cannot be performed at the point of care. Acoustic resonance force impulse testing is another radiologic method for measuring liver fibrosis, but this method is still undergoing evaluation and has not yet been broadly adopted for clinical use.22
Oxidative stress increases the fragility of red blood cells. Oxidative stress also decreases the rate of erythroid maturation and decreases erythrocyte lifespan.23 Previous studies have reported that higher RDW is correlated with hypertension,24 inflammatory bowel disease,15 microalbuminuria,14 and cardiovascular diseases. These conditions which are associated with low antioxidant nutrients. The primary source of plasma glutathione peroxidase is the kidney and plasma selenium, plasma glutathione peroxidase, and glutathione peroxidase activity in erythrocytes have been strongly correlated with stages of chronic renal failure.25 Inflammatory bowel disease is associated with lower circulating carotenoids and increased oxidative stress.26
To the best of our knowledge this is first study that has attempted to analyze the association between RDW and NAFLD fibrosis. In this study we showed that higher levels of RDW and ferritin were associated with a higher BARD score and FIB-4 score. Ferritin has previously been shown to predict advanced fibrosis in NAFLD in several studies.27 An elevated hsCRP level, however, was not associated with advanced fibrosis in NAFLD in this study. It is tempting to speculate that higher RDW may will be an earlier marker of chronic subclinical inflammation might be responsible for the association between RDW and advanced fibrosis in NAFLD at normal hsCRP levels.5,28
Among biomarkers of inflammation, hsCRP has proved to be the most robust, as it is an excellent analyte with a standardized assay. a strong, graded association of RDW with hsCRP and ESR independent of numerous confounding factors.5
RDW is also found to be elevated in conditions associated with higher oxidative stress28,29 and has been shown to be associated with markers of oxidative stress,4 which in turn might explain the association with elevated RDW values.30
Our study findings indicate a graded association between high RDW and advanced fibrosis. Although the precise pathophysiologic link between this interaction was not examined in the present study, common interactions between inflammation, oxidative stress may explain the observed association and the emerging utility of these biomarkers in the prediction of advanced fibrosis in NAFLD.
Our study is a cross-sectional analysis with inherent limitations and thus it is unable to definitively comment on causality or temporal association. Our study was confined to a relatively racially homogenous group of individuals of Korean descent who were recruited at a single medical institution. This study did not incorporate liver biopsies, which is the gold standard in diagnosing the level of fibrosis in NAFLD. However, our group and others have previously published studies using BARD score and FIB-4 score to establish the degree of fibrosis. Finally, a different number of subjects in each study group is another potential limitation.
In conclusion, in a very large cohort, our observations revealed a graded positive relationship between RDW and the level of fibrosis in NAFLD independent of multiple confounders, including hsCRP. Further studies with larger sample sizes and prospective approaches are needed to elucidate the mechanism underlying this association.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




