Safety of reduced dose of mycophenolate mofetil combined with tacrolimus in living-donor liver transplantation
Article information
Abstract
Background/Aims
The dose of mycophenolate mofetil (MMF) has been reduced in Asia due to side effects associated with the conventional fixed dose of 2-3 g/day. We aimed to determine the pharmacokinetics of a reduced dose of MMF and to validate its feasibility in combination with tacrolimus in living-donor liver transplantation (LDLT).
Methods
Two sequential studies were performed in adult LDLT between October 2009 and 2011. First, we performed a prospective pharmacokinetic study in 15 recipients. We measured the area under the curve from 0 to 12 hours (AUC0-12) for mycophenolic acid at postoperative days 7 and 14, and we performed a protocol biopsy before discharge. Second, among 215 recipients, we reviewed 74 patients who were initially administered a reduced dose of MMF (1.0 g/day) with tacrolimus (trough, 8-12 ng/mL during the first month, and 5-8 ng/mL thereafter), with a 1-year follow-up. We performed protocol biopsies at 2 weeks and 1 year post-LDLT.
Results
In the first part of study, AUC0-12 was less than 30 mgh/L in 93.3% of cases. In the second, validating study, 41.9% of the recipients needed dose reduction or cessation due to side effects within the first year after LDLT. At 12 months post-LDLT, 17.6% of the recipients were administered a lower dose of MMF (0.5 g/day), and 16.2% needed permanent cessation due to side effects. The 1- and 12-month rejection-free survival rates were 98.6% and 97.3%, respectively.
Conclusions
A reduced dose of MMF was associated with low blood levels compared to the existing recommended therapeutic range. However, reducing the dose of MMF combined with a low level of tacrolimus was feasible clinically, with an excellent short-term outcome in LDLT.
INTRODUCTION
Mycophenolate mofetil (MMF) has been combined with calcineurin inhibitors for the prevention of acute cellular rejection (ACR) and to decrease the side effects of calcineurin inhibitors following kidney, heart, and liver transplantation (LT).1 Despite the widespread use of MMF in combination with tacrolimus, the optimal dose for this combination has yet to be defined, especially for LT.2 It has conventionally been administered as a fixed dose (2.0-3.0 g/day) without routine plasma concentration monitoring of mycophenolic acid (MPA), the active metabolite.2,3,4,5,6
In a 2008 consensus meeting about MPA in Rome,7 the recommended initial daily dose of MMF was 3.0 g rather than 2.0 g with cyclosporine in adult transplantations. It is more likely to achieve the minimum target MPA exposure in early post transplantation. However, clinically, the most popular dose of MMF is based on the side effects (leukopenia, gastrointestinal problems such as abdominal discomfort or diarrhea, infection, etc.). Indeed, many studies conducted in Asian renal transplant recipients, including a randomized controlled trial, suggested the need for MMF dose reduction so as to minimize the side effects of MMF.8,9,10 In Korea, mostly 1.0 to 1.5 g daily of MMF was used in actual clinical situations, based on the side effect. That is a generally reduced dose in comparison to that given in Western countries and in comparison to the recommendation from the 2008 consensus meeting.
There are a few studies on the pharmacokinetics or feasibility of a reduced dose of MMF, especially in living donor LT (LDLT). Therefore, we designed two sequential studies with the following aims: 1) a preceding prospective preliminary study for pharmacokinetics of a reduced dose of MMF in early post-LDLT, and 2) a validating study for the feasibility of a reduced dose of MMF with tacrolimus combination within the first year follow-up after LDLT.
PATIENTS AND METHODS
Patient selection
For the pharmacokinetics of a reduced dose of MMF in early post-LDLT, we performed a preceding prospective preliminary study, and then a retrospective following study for validation. In the preliminary study, eligible patients were adult LDLT recipients with end-stage liver disease at our institution, and we administered MMF (mainly 1.0 g/day) with tacrolimus (through level, 8-12 ng/mL) with 14 days follow-up after LT (or hospital stay if the length of stay was < 14 days). We performed the protocol biopsy before discharge. We excluded patients with any of the followings: age <19 or >65 years, previous organ transplantation, multiple organ transplantation, pregnancy, breast-feeding, advanced hepatocellular carcinoma with invasion of major vessels or distant metastasis, human immunodeficiency virus positive, active peptic ulcer within two weeks, administration of other study drug, hemodialysis within 30 days of LT, serum creatinine level over 1.4 mg/dL before LT, contraindication of tacrolimus or corticosteroids or MMF or basiliximab, and poor compliance to regular follow-up. This study was approved by the institutional review board at Seoul National University Hospital (approval number: 0811-068-263).
Between October 2009 and December 2011, 365 cases of LT had been performed at the Seoul National University Hospital (Seoul, Korea), and all of recipients received blood group compatible grafts and orthotopic LT. Among these, 215 recipients were adults, and underwent LDLT. In the following validating study, we selected the patients who were initially administered a reduced dose of MMF (1.0 g/day) with tacrolimus, with a follow-up period of 1 year after LT. We excluded patients with same criteria in the preceding pharmacokinetic study and the patients enrolled in the preceding study. This study was approved by the institutional review board at Seoul National University Hospital (approval number: 1311-086-536).
Immunosuppressive protocol
All recipients had received induction with 20 mg of intravenous basiliximab (an interleukin-2 receptor antagonist; Simulect, Novartis) within two hours before LT and on postoperative days (POD) 4. Initially, a basal immunosuppressive regimen based on tacrolimus (Prograf, Astellas or Tacrobell, Chong Kun Dang), steroids, and MMF (CellCept, Roche) was administrated as a part of the initial triple immunosuppressive regimen or was introduced during follow-up as a maintenance immunosuppressive agent.
Tacrolimus started within 5 days after LT. The tacrolimus dose was adjusted according to individual clinical need with respective target whole-blood trough levels around 8 to 12 ng/mL for the first month after LT, followed by 5 to 8 ng/mL thereafter. Intravenous methylprednisolone 500 mg was given intra-operatively before portal perfusion, and was tapered from 200 mg to 20 mg within 6 days. Thereafter, oral prednisolone was continued at 20 mg daily until the first month after LT, and tapered to 0 to 5 mg/day after about 6 months post-LT. MMF was started with 1.0 g daily within 5 days (93.3% in the preliminary study and 100.0% in the validating study) after LT and adjusted according to the occurrence of related side effects.
Measurements of MPA plasma concentration and the AUC0-12
In the pharmacokinetic study, for therapeutic drug monitoring (TDM) of MMF, we measured the concentration of MPA and the area under the curve from 0 to 12 hours (AUC0-12). To measure pharmacokinetic parameters, blood samples before the dose (C0) and at 1, 2, 4, 6, and 12 hours after the dose were obtained on POD 7 and 14. About 5 mL of venous blood were collected into EDTA tubes. The plasma concentration of MPA was measured by a validated high-performance liquid chromatography tandem mass spectrometry. The full AUC0-12 was determined according to the Classic linear trapezoidal method.
Follow-up and investigation of safety and efficacy
In the validating study, the patients were usually discharged in POD 14 to 30, and complete laboratory investigation was conducted almost daily during hospital stay, including liver function tests (LFT) and blood tacrolimus trough level. Outpatient follow-up was usually conducted once a week for the first month after discharge and was gradually lengthened to every 3 or 4 months, with additional visits as Clinically necessary. A complete laboratory investigation, including LFT and blood tacrolimus trough level measurement, was conducted at each follow-up.
MMF was initially administered daily with dose of 1.0 g if the white blood cell (WBC) count exceeded 3,500/mm3, reduced to 0.5 g daily for 2,500 to 3,500/mm3, and ceased for less than 2,500/mm3. During follow-up, we decreased or ceased the MMF based on apparent toxicities with clinical suspicion related to MMF: neutropenia (defined as WBC count <3,500/mm3 in this study), gastrointestinal problem, or infection including cytomegalovirus.
Nephrotoxicity was defined as an elevated serum creatinine (>1.4 mg/dL) after excluding renal insufficiency due to other causes.
Patients underwent an ultrasonography-guided protocol liver biopsy. Protocol biopsies were performed at POD 7 to 14, additional biopsies at 1 year after LT, and at the time as clinically indicated. We defined the acute cellular rejection (ACR) when the rejection activity index (RAI, Banff score; 0-2, no rejection; 3, borderline; 4-5, mild rejection; 6-7, moderated rejection; 8-9, severe rejection) was of 4 or more points.11 When RAI was 4 points, we maintained the level of tacrolimus in cases without abnormal LFT, but we increased the level of tacrolimus with significant abnormal LFT results. When RAI was 5 or more points, we treated the patients with steroid pulse therapy regardless of abnormal LFT. In all cases, informed consent was obtained from each patient before biopsy.
Statistical analysis
In the validating study, statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Illinois, USA).Continuous data were presented as the mean ± standard deviation or medians, and categorical parameters were presented as the number of cases with percentage in parenthesis. Survival rates were estimated using the Kaplan-Meier method and compared using the Log rank test.
RESULTS
Patient enrollment and characteristics
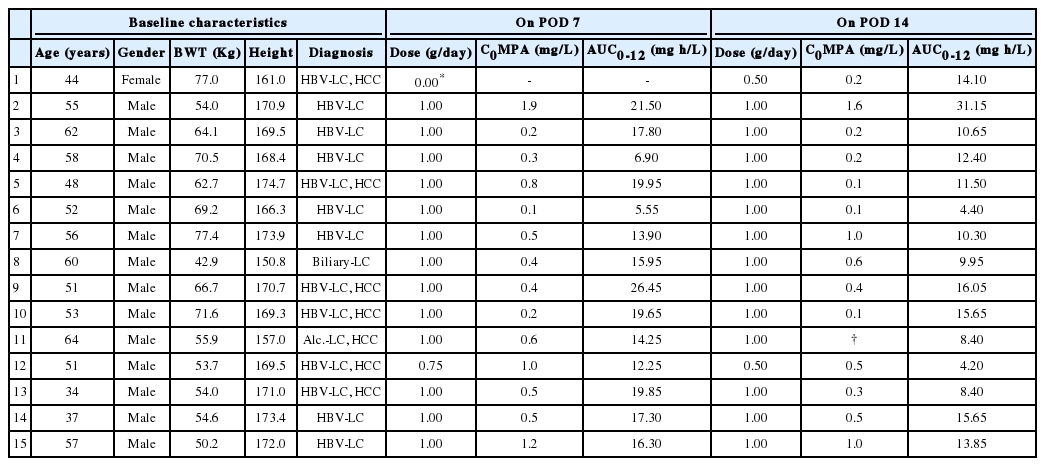
Among 215 adult patients who underwent LDLT between October 2009 and December 2011, 17 patients were enrolled in the pharmacokinetic study. Two patients dropped out due to withdrawal (refusal of samplings). Finally, 15 patients (14 males and 1 female; mean age 52.1 years, range 34 to 64 years) were enrolled. LT had been performed mainly due to hepatitis B virus-related liver cirrhosis in 86.7% (n=13), and 7 patients (46.7%) had a coexisting hepatocellular carcinoma. The baseline characteristics of the 15 patients are shown in Table 1.
Characteristics of the patients and pharmacokinetic parameters of a reduced dose of MMF in preliminary study
In the validating study, among 215 adult patients, 74 patients (61 males and 13 females; mean age 52.3 years, range, 25-65 years) were included. LT had been performed due to mainly hepatitis B virus-related liver cirrhosis (75.7%), and 60.8% had a coexisting hepatocellular carcinoma (n=45). Table 2 summarized the baseline characteristics of the 74 patients.

Baseline characteristics of the patients in a reduced dose of MMF with tacrolimus combination in adult LDLT
Plasma MPA levels and AUC0-12 of reduced dose of MMF (mainly 1.0 g daily)
In the pharmacokinetic study, the initial dose of MMF started with 1.0 g daily with tacrolimus within 5 days after LT and was maintained with 1.0 g daily during follow-up, except for 2 cases: one for pre-dosing leukopenia and the other for side effect. After all, most of the patients received MMF with 1.0 g daily (86.7%) in early post-LDLT. In the first case, the patient had to skip the MMF for a week due to pre-dosing leukopenia and then started with a lower dose (0.5 g/day). In case number 12, the patient's initial dose of MMF was 1.0 g daily, but he had to reduce the dose as time passed because of gastrointestinal symptoms. Comparing to the generally recommended therapeutic range (30-60 mg h/L),7 the AUC0-12<30 mg h/L was present in 100% on POD 7 (range, POD 6-8) and present in 93.3% on POD 14 (range, POD 10-19). The median AUC0-12 was 16.30 mg h/L (range, 5.55-26.45 mg h/L) on POD7 and 11.50 mg h/L (range, 4.20-31.15 mg h/L) on POD14 as shown in Table 1.
Efficacy and safety
In the preliminary study, the mean hospital stay was 15.6 days (range, 9-43 days). There was no mortality and no major complications (Clavien-Dindo classification grade ≥IIIa).12 There was no biopsy-proven ACR or graft loss. Also, there were no episodes of elevation of blood urea nitrogen or serum creatinine (>1.4 mg/dL). There was only one case of a drug related side effect, case number 12, as previously described. The patient's initial dose of MMF was 1.0 g daily, but he had to reduce the dose as time passed because of gastrointestinal problem. He received the dose of 0.75 g/day on POD 7, and 0.5 g/day on POD 14 (Table 1).
In the validating study, side effects of the patients in immunosuppression of reduced dose of MMF combined with a low level of tacrolimus in adult LDLT are summarized in Table 3. A total of 64.9% (n=48) maintained the initial dose of MMF (1.0 g/day). Among 74 recipients, 41.9% (n=31) experienced dose reduction or cessation of MMF due to related side effects at least once within the first year after LT. Finally, 12 months after LT, 17.6% (n=13) were administered a lower dose of MMF (0.5 g/day), and 16.2% (n=12) needed permanent cessation of MMF due to side effects. Even with a reduced dose of MMF with tacrolimus combination immunosuppression, leukopenia was present in 51.4%, nephrotoxicity in 10.8%, gastrointestinal problems in 6.8%, and infection in 5.4% during the study period. Leukopenia was the most common side effect requiring dose reduction or cessation of MMF. At 1 year after LT, nephrotoxicity related with tacrolimus was present in 4.1% of the cases (n=3), but there was no severe renal impairment requiring medication or renal replacement therapy. One patient needed an increased dose of MMF (1.5 g/day) to reduce tacrolimus due to calcinuerine inhibitor related nephrotoxicity.

Side effects of a reduced dose of MMF
In the validating study, the short-term outcome of the patients in immunosuppression of a reduced dose of MMF combined with a low level of tacrolimus with a follow-up of 1 year in adult LDLT is summarized in Table 4. Overall biopsy-proven ACR was present in 2.7% of the cases (n=2), and both cases were of mild ACR. One patient who underwent biopsy at 2 weeks post-LT showed 4 points of RAI without an abnormal LFT and maintained the usual immunosuppressants. The other patient who underwent biopsy at 1 year post-LT showed 5 points of RAI with a significant abnormal LFT and was treated with steroid pulse therapy with good response. In other pathologic abnormalities, portal inflammation (≥ mild degree) was present in 39.2%, and fibrosis (≥ mild degree) in 18.9% of the cases within the first year after LT. Major morbidity (Clavien-Dindo classification grade ≥IIIa) was present in 18.9% (n=14), and biliary complication was most common. There was no mortality. Patient and graft survival were 100% at 12 months after LT, both. The 1-, 6- and 12-month rejection-free survival rates were 98.6%, 98.6% and 97.3%, respectively (Fig. 1).

Short-term outcome of a reduced dose of MMF with low level of tacrolimus in adult LDLT
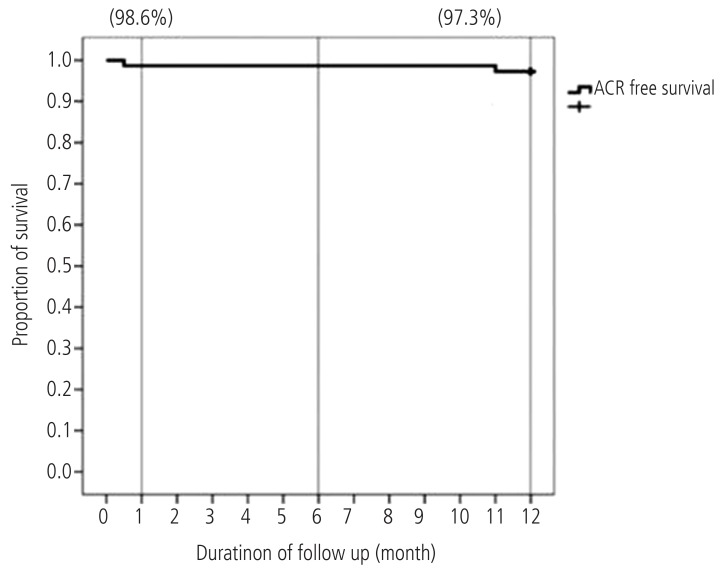
Kaplan-Meier curve showing acute cellular rejection (ACR)-free survival for patients in reduced dose of mycophenolate mofetil with tacrolimus combination in adult living donor liver transplantation.
DISCUSSION
The initial dose of MMF was recommended at 2.0 to 3.0 g daily in previous studies, but those were based on adult renal transplantation and concomitant cyclosporine therapy.2,3,4,5,7,8 The recommended initial dose of MMF is based on data from clinical trials carried out in Western countries,7,8,13 and, actually, lower doses of MMF have been needed due to side effects in clinical settings in Asian countries. Therefore, we designed the present study composed of pharmacokinetics and validation on the appropriate dose of MMF combined with tacrolimus in LDLT in Asian. To the best of our knowledge, this was the first biopsy-proven study on that.
The MPA AUC0-12 is generally regarded as the most reliable pharmacokinetic parameter of risk for ACR 14,15 and the choice for drug exposure evaluation.16,17,18 Although the results are conflicting, MPA levels determined via high performance liquid chromatography between 1.0 and 3.5 mg/L for the C0, and 30 to 60 mg h/L for AUC0-12 have been recommended following renal or heart transplantation.3,4,6,7,14,19,20
Van Gelder et al.17 concluded that under-exposure to MPA in the first week after renal transplantation is highly predictive of the development of subsequent acute rejections, and an increased MMF starting dose may be the way to go. However, Brunet et al. reported21 that during the first month after LT, exposure to MPA was low in a considerable proportion of 15 LT recipients receiving MMF at 2 g/day and tacrolimus, and they showed that there was no relationship between MPA pharmacokinetics and the efficacy of MMF. In the present study, compared to the generally recommended therapeutic range, the AUC0-12 was low in almost all patients except one. However, there was no biopsy-proven ACR, graft loss, or death in early post-LDLT.
From other studies, the incidence of dose reduction of MMF at least once due to side effects ranged from 42.0% to 70.3% with a standard dose of MMF of 2.0 or 3.0 g/day in renal transplantation.22,23,24 In the present study, although MMF was initially administered in a low dose (1.0 g/day) compared to recommendations from others, 41.9% experienced a dose reduction or cessation of MMF due to related side effects at least once within the first year after LT. Finally, about one-third of patients (33.8%) needed to reduce the dose of MMF (<1.0 g/day) due to related side effects at 1 year post-LT. This is similar to the other studies (25-35%), even though it was in a different baseline dosing of MMF (1.0 g/day vs. 2.0-3.0 g/day).25,26,27,28
Among all the side effects in this study that caused additional MMF dose adjustment, leukopenia was most common (87.1%). Even though WBC count at the time of the start of MMF exceeded 3,500/mm3 in all patients, leukopenia occurred in 36.5%. The reason why the recipients in our study were very sensitive to leukopenia, even in a reduced dose of MMF and of tolerable condition before administration, maybe due to pre-LT existing leukopenia, partial graft of LDLT, and relatively lower total body weight in this population.8 Pre-LT WBC count had mean 4,540/mm3 (range, 1,180-21,200/mm3), and leukopenia (<3,500/mm3) was present in 44.6% at pre-LT. This considerable portion of preoperative leukopenia may be due to portal hypertension from underlying liver cirrhosis.
With respect to safety and efficacy, under tacrolimus based immunosuppression in adult LDLT, Yilmaz et al. reported the biopsy proven ACR as 11% for 107 recipients within the first year after LT,29 and Sugawara et al. reported that as 45% for 100 recipients within the first three months after LT.30 In our study, the overall biopsy-proven ACR was present in 2.7% of the cases, and this is excellent result compared to that of others. The reason for this excellent outcome may be due to the following characteristics in our cohort: 1) hepatitis B-virus related liver cirrhosis dominant baseline (75.7% in validating study)31,32; 2) selected patients with pre-LT normal renal function (100.0%); 3) low Model for End-stage Liver Disease score (mean, 15.32±8.23); 4) almost all were of elective LDLT (97.3%). In a similar cohort in our institute, we had reported that the 1-year survival rate was present in 96.0% and the graft survival in 99.0%, even with different immunosuppressant base.33 Additionally, a relatively small sample size was one of the limitations of this study. For evaluation of the long-term outcome and renal preserving effects of immunosuppression of reduced dose of MMF combined with low trough level of tacrolimus in LT, long-term follow-up and more studies should be continued, henceforward.
In conclusion, a reduced dose of MMF was pharmacokinetically low compared to the existing recommended therapeutic range in early post-LDLT. Even with the low level of MPA AUC0-12, there was no biopsy-proven ACR, graft loss, or death of patients under immunosuppression combined with low trough level of tacrolimus within the first year after LDLT. Even with the initially reduced dose of MMF, dose adjustment was frequently needed due to the side effects. After all, reduced dose of MMF combined with low levels of tacrolimus was feasible and safe with an excellent short-term outcome in hepatitis B virus dominant adult LDLT. More long-term follow-up and larger-scale prospective studies for this in LT are needed in the future.
Acknowledgements
This work was presented in part at the 12th Congress of the Asian Society of Transplantation (CAST 2011).
Notes
The prospective preliminary pharmacokinetic study in this work was supported by a grant from Roche (06-2009-1310). There was no grant or financial support in the following validating study.
The authors have no conflicts to disclose.
Abbreviations
ACR
acute cellular rejection
Alc.
alcoholic
AUC0-12
area under the curve from 0 to 12 hours
BUN
blood urea nitrogen
BWT
body weight
C0MPA
plasma concentration of mycophenolic acid at pre-dosing
GFR
glomerular filtration rate
GI
gastrointestinal
HBV
hepatitis B virus
HCC
hepatocellular carcinoma
LC
liver cirrhosis
LDLT
living donor liver transplantation
LFT
liver function tests
LT
liver transplantation
MELD
model for end-stage liver disease
MMF
Mycophenolate mofetil
MPA
mycophenolic acid
POD
postoperative days
RAI
rejection activity index
TDM
therapeutic drug monitoring
WBC
white blood cell