

INTRODUCTION
Chronic hepatitis C affects an estimated 1-2% of the Korean population and is one of the leading causes of liver cirrhosis and hepatocellular carcinoma in Korea and is closely linked to insulin resistance (IR) and lipid metabolism.1,2 Moreover, in hepatitis C virus (HCV) antibody-positive patients, glucose intolerance in the absence of diabetes was reported to be 3.5-fold higher than in HCV antibody-negative patients.3
Interferon (IFN), in combination with ribavirin (RBV), is the standard treatment used to eradicate viruses and prevent the progress of liver disease in CHC patients. Sustained virologic response (SVR) is predicted by negative HCV RNA at week 4 or 12 of treatment. However, rapid normalization of alanine aminotransferase (ALT) also predicts viral response during treatment in CHC patients.4 Moreover, HCV is related to the onset and progress of lipid metabolism; therefore, total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels are useful factors in terms of predicting the effects of IFN therapy.5
Minuk et al6 reported that patients with high serum cholesterol concentrations had a greater likelihood of successful treatment with IFN, suggesting that serum lipid concentration may be an important predictive factor for response to CHC treatment. This study tracked differences in lipid profile and IR prior to treatment and after treatment in CHC patients who received combination therapy with IFN and RBV.
PATIENTS AND METHODS
Patients
During the study period, 203 patients received combination therapy with IFN and RBV for CHC at Bucheon Hospital in Soonchunhyang University from January 2005 to December 2011. Among these patients, 60 underwent continuous measurement of lipid levels and homeostasis model for assessment (HOMA) values and were compared to 23 chronic hepatitis B (CHB) patients who received IFN therapy and underwent continuous measurement of lipid levels and HOMA values. We excluded patients who were administered a lipid-lowering agent or a glucose-lowering agent, such as metformin, glitazones or subcutaneous insulin, which could affect lipid metabolism or IR. Alcohol intake was limited to 40 g for males and 30 g for females once per week. In addition, routine exercise and diet control were recommended for each patient to limit these variables during the study period.
Patients received a subcutaneous injection of 180 ┬Ąg peg-IFN-╬▒-2a or 1.5 ┬Ąg/kg peg-IFN-╬▒-2b once per week, together with 1200-mg RBV to those patients with HCV genotype 1, and 800-mg RBV to those without non-HCV genotype 1. HCV RNA levels were measured using a quantitative polymerase chain reaction (PCR) assay (Artus HCV RG reverse transcription [RT]-PCR kit; Qiagen, Hamburg, Germany).
Insulin and fasting blood glucose were calculated for HOMA-IR and HOMA-╬▓ to measure IR, and changes between pre- and post-treatment were examined in the high-IR group, defined as a pre-treatment HOMA-IR >2.5. SVR was defined as HCV RNA clearance 24 weeks after the end of treatment. To determine whether these changes were due to IFN, changes in lipid levels and HOMA values in the CHB patients were compared to virologic responses pre-treatment, and at 24 and 48 weeks after treatment.
The period before treatment was defined as BTx, the end of the treatment as DTx, and 24 weeks after end of the treatment as ATx. HOMA-╬▓ and HOMA-IR were calculated as follows:
Statistical analysis
Statistical analysis was performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA). The results represent means┬▒standard deviation (SD). Analysis of variance (ANOVA) was used to evaluate continuous variables, and Pearson's chi-square2 test used to analyze categorical variables. A P<0.05 was considered to indicate statistical significance.
RESULTS
Baseline clinical characteristics
In the CHC patients, we observed a SVR in 49 of 60 patients (81%), which included 36 of 60 patients (60%) with HCV genotype 1. The pre-treatment patient age was significantly higher in the non-SVR group than the SVR group (56.6 vs. 48 years, respectively; P = 0.007). There was no significant difference in pre-treatment body mass index (BMI), alanine aminotransferase (ALT), HCV RNA titer, TC, TG, LDL-C, HDL-C, HOMA-IR or HOMA-╬▓ (Table 1).
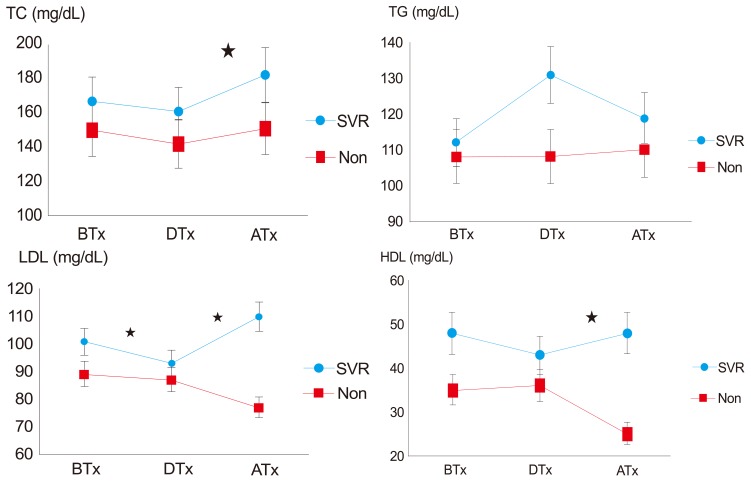
Changes in treatment response-dependent lipid profile
In the CHC patients, TC, LDL-C, HDL-C tended to decrease DTx and increase again ATx in the SVR group. LDL-C significantly changed DTx (BTx, 101.1; DTx, 93.2; P =0.008) and changed ATx in the SVR group (DTx, 93.2; ATx, 110.8; P=0.001; Table 2-1 and Fig. 1). We analyzed the 23 CHB patients using a similar method, and found no significant difference BTx, DTx, and ATx (Table 2-2). However, this data set was limited by the small sample size (SVR=15, non-SVR=8).
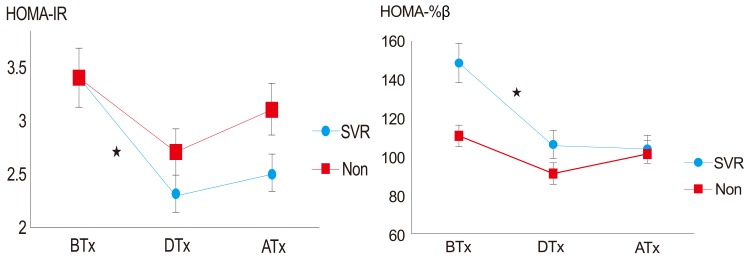
Changes in treatment-response-dependent insulin resistance
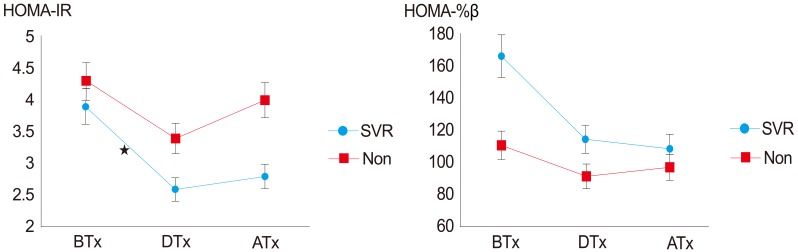
To evaluate the IR from HOMA-╬▓ and HOMA-IR values, fasting insulin and blood glucose values were examined with changes in HOMA-╬▓ and HOMA-IR. There was a significant change in HOMA-╬▓ and HOMA-IR DTx (Table 3 and Fig. 2). Pre-treatment HOMA-IR >2.5 was defined as high IR with a higher SVR rate with low baseline insulin resistance (71.5% in patients in HOMA-IR >2.5 vs. 86.7% in HOMA-IR <2.5 group). In HOMA-IR >2.5 patients, HOMA-IR significantly decreased DTx in the SVR group (BTx, 3.9; DTx, 2.6; P=0.035; Table 4 and Fig. 3).
DISCUSSION
Patients with LC due to HCV have a three- to five fold higher frequency of diabetes compared to patients with hepatitis B.7 With the worldwide spread of CHC, the correlation of metabolic syndrome with IR is a major public health problem gaining importance. It has been reported that HCV infection is itself a risk factor for metabolic syndrome and affects glucose metabolism through various direct or indirect mechanisms to induce IR, which aggravates liver disease and reduces the response to anti-viral treatment.
In a meta-analysis of 34 studies, CHC patients had twice as many risk factors for diabetes and when age and BMI were considered, an 11-fold risk was calculated.8 However, the association between CHC and IR remains unknown. Patients with diabetes have a significantly higher CHC infection rate than non-infected patients, and accordingly, HCV increases the prevalence of diabetes and is more prevalent in diabetic patients.9
Treatment of CHC patients with IFN may influence lipid metabolism by several mechanisms. The first is resolution of hepatic inflammation after successful HCV eradication, which may normalize hepatocellular function and hepatic production of serum lipoproteins.10
The second is that IFN itself may alter lipid metabolism via receptors on hepatocytes, adipocytes and enterocytes, which have several important roles in the regulation of serum lipid concentrations.11 The third is that eradication of HCV from hepatocytes may normalize hepatocyte function if HCV has a direct effect on hepatocyte lipid metabolism.12
Several studies have reported that LDL-C is a useful predictive prognostic factor for treatment with IFN and RBV in CHC. Minuk et al6 speculated that LDL may inhibit HCV binding to receptors on hepatocytes13,14 and SVR was greater in CHC patients with a higher pre-treatment LDL-C concentration, indicating that it could be predictive of treatment success. Even though significant differences were not noted in the current study, the LDL-C level was relatively high in the SVR group at 101 mg/dL compared to the non-SVR group at 89.2 mg/dL. Furthermore, we observed that TC and LDL-C decreased in the SVR group during treatment and returned to baseline levels after the end of treatment. In the non-SVR group, LDL-C decreased consistently, even after the end of treatment, while TC returned baseline in a manner similar to the SVR group after the end of the treatment. This is consistent with the report by Tada et al15 of 185 Japanese patients, in whom TG tended to increase in the SVR group during early treatment and decrease to the baseline level after the end of the treatment.
Cholesterol is associated with HCV since the exterior membrane of HCV has an affinity for lipids. LDL combined with HCV results in the abnormal lipid metabolism associated with the eradication of HCV.16 Since successful treatment of CHC reduces the quantity of lipid combined with HCV, the serum concentration of circulating lipid increases. The serum TG concentration displayed a different course during IFN treatment compared to serum total cholesterol. TG concentration remained significantly higher during IFN treatment and returned to its pretreatment level after the end of treatment. Therefore, this dramatic change in serum TG levels is likely caused by the IFN treatment itself. The activity of hepatic TG lipase, an enzyme that degrades serum TG, is inhibited during IFN administration, and hepatocellular TG synthesis is stimulated by IFN treatment.17,18 Therefore, the elevated TG levels during IFN treatment might be caused by an IFN-induced decrease in TG degradation, as well an IFN-induced increase in hepatic TG synthesis.
IR is associated with genotype and a high viral load predicts anti-viral therapeutic responses in CHC patients.19 IR is defined as a situation in which the normal concentration of insulin cannot induce a normal metabolic process, or a requirement for supraphysiological amounts to induce the normal metabolic process.20 The mechanisms underlying HCV-induced IR in hepatocytes remain unknown but it is thought that progress to LC in existing HCV can be aggravated by induction of liver fibrosis through differential stimulation of phosphatidylinositol-3-kinase and extracellular-regulated kinase photophosphorylation.21 While IR is reported at a frequency of 10-25% in the normal population, it can be as high as 30-70% in CHC patients.22 Obesity is a common cause of IR, but according to Bartenschlager et al,23 there is no specific association between IR and obesity in CHC patients. In this study, there was no significant difference in BMI between the SVR and non-SVR groups.
Several prior studies using surrogate measures of IR, including HOMA-IR, report that IR is a predictor of non-response to anti-HCV therapy.24,25,26,27 In a study of 159 Spanish patients, individuals with SVR had lower baseline HOMA-IR score compared with non-SVR patients (HOMA-IR=2.4 vs. 3.8).28 In addition, after adjusting for genotype and liver fibrosis scores, the odds of non-sustained response to anti-HCV therapy were ~1.8-fold higher with increasing HOMA-IR scores.28
The association between SVR and IR, however, has not been reported consistently. In a recent study of 412 Italian patients, SVR was associated with HCV genotypes 2 and 3 and younger age, but baseline HOMA-IR scores between individuals who did and did not achieve SVR did not reach statistical significance.29 In another study, there were no improvements in SVR despite pharmacologically induced improvement of IR with metformin.30 Some studies have shown a statistically significant decrease in HOMA-IR scores with viral eradication and achievement of SVR.28,31
When using precise measurements, IR did not appear to be substantially associated with achievement of SVR. Moreover, successful viral eradication did not substantially influence IR when compared with HCV therapy that does not result in SVR. However, HCV therapy, regardless of SVR achievement, appeared to improve IR. This suggests that individuals with higher degrees of IR may benefit from receiving HCV therapy in an attempt to decrease their risk of clinical sequelae of IR. Currently, in HOMA-IR and HOMA-╬▓ showing IR, glucose intolerance improves when the HOMA-IR level is high and HOMA-╬▓ is low, and HOMA-IR reflects IR itself, while HOMA-╬▓ reflects the insulin secretion of the pancreas.
A hepatitis C antiviral long-term treatment against cirrhosis (HALT-C) study reported that the decrease of HOMA-IR correlated with the removal of virus at 24 weeks of treatment32 and according to a study on 277 Taiwanese patients by Huang et al2 after IFN treatment, HOMA-╬▓ showed a significant decrease; in the group with high pre-treatment HOMA-IR, HOMA-IR and HOMA-╬▓ decreased significantly after the treatment regardless of SVR.
In South Korea, there was a report describing HOMA-IR and BMI measurements in CHC 28 patients who received IFN and RBV treatment with 22 patients in the SVR group (78.6%) and HOMA-IR significantly decreased in the SVR group. However, there was no significant change in BMI; 6 of 28 patients were in the non-SVR group, and showed no significant changes in BMI and HOMA-IR level.33
Preceding studies report that IR is an independent predictive factor for SVR in CHC patients. SVR occurs in 32.8% of patients with genotype 1 and HOMA-IR >2, compared to 60.5% of those with HOMA-IR <2. However, other prospective studies report that the lower the pre-treatment HOMA-IR, the higher the SVR with IFN treatment; thus, pre-treatment HOMA-IR will help to predict the results of treatment. In our study, the HOMA-IR and HOMA-╬▓ values decreased significantly during treatment, while among the patients with high pre-treatment HOMA-IR, the SVR group showed a significant decrease in HOMA-IR at the end of treatment. However, because a number of factors (such as age, obesity and the degree of hepatocyte damage) was not controlled, there is a limitation in the interpretation of the results. In the pretreatment high-insulin-resistance group (HOMA-IR >2.5), the HOMA-IR was decreased significantly in SVR group during DTx. Therefore, treatment response and insulin resistance changes are likely related, and successful HCV treatment would lead to improvements in IR and insulin hypersecretion.
Only Kim et al33 reported IR and lipid metabolism changes in CHC patients in Korea, which included only 28 patients. Our study did not compare variables that might affect the results (i.e., BMI), as it was of a retrospective design with a limited number of patients compared to other reports. However, the results are significant because they support the eradication of HCV with peg-IFN and RBV that alters lipid metabolism and might be improve IR in Korean patients.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




