

INTRODUCTION
Hepatic hemangiomas frequently accompany arterioportal shunt with an incidence of up to 26%.1 CT and MR findings of these tumors with arterioportal shunt have been well addressed; they tend to show rapid contrast enhancement than those without shunt on dynamic studies.1 However, it is still worthwhile to detail sonographic features of such tumors, because they are frequently found at screening sonography incidentally and further or follow-up study can be simplified if they can be differentiated from malignant tumors. In this article, we present suggestive sonographic findings of hepatic hemangioma attributed to an accompanied arterioportal shunt.
CASE
A 58-year-old man visited our hospital with right upper quadrant pain. His clinical history did not include any specific disease, family history was unremarkable, and physical examination was unremarkable. The results of routine laboratory investigations were unremarkable as well. Serologic tests for hepatitis A, B, and C were negative.
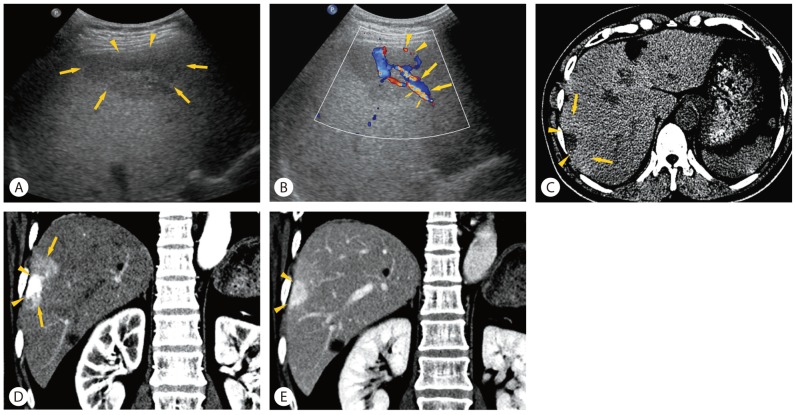
Hepatic sonography showed increased liver echogenicity, suggestive of hepatic steatosis. Gallbladder was unremarkable, and there was no remarkable abnormal finding in the biliary tree and pancreas as well. In the subcapsular area of the right hepatic lobe, there was a 2-cm, well-defined nodule with echo-poor appearance, surrounded by large geographic perinodular hypoechoic area, suggestive of peritumoral sparing of hepatic steatosis (Fig. 1). There was no thrombus at the portal branch, in the spared area of hepatic steatosis around the tumor. Doppler study revealed hypervascularity of the tumor and the reverse hepatofugal flow of the peritumoral portal vein parallel to the feeding artery, indicating the presence of arterioportal shunt accompanying the tumor. Based on grayscale and Doppler sonographic findings, hepatic hemangioma with arterioportal shunt was highly suspected.
Unenhanced and postcontrast dynamic CT scans were performed for further evaluation of hepatic tumor. Unenhanced CT scan showed decrease of hepatic parenchymal attenuation, suggestive of hepatic steatosis. The tumor was seen as low attenuation nodule in the subcapsular area of the right hepatic lobe, surrounded by subtle hyperdense area, suggesting peritumoral sparing of steatosis. Dynamic contrast-enhanced CT showed strong homogenous enhancement of the tumor, surrounded by large wedge-shaped parenchymal hyperenhancement during the arterial phase. The tumor showed persistent enhancement similar to hepatic vessels and the surrounding parenchymal hyperenhancement was also appreciated during the venous phase. Several small nodules (< 1 cm) with similar enhancement pattern as the one described above were also noted in both hepatic lobes. The diagnosis of hepatic hemangiomas with arterioportal shunt was made by typical CT features.
DISCUSSION
Most commercial ultrasound scanners are equipped with Doppler function, and Doppler study is widely used as a part of routine examination for liver tumors. The value of Doppler sonography for the evaluation of hepatic hemangioma has been generally underestimated, presumably because most typical hemangiomas have slow intratumoral flow below the sensitivity limits of Doppler technique. However, in contrast to the dissatisfying results of Doppler sonography in typical slow-flow hemangiomas, it has been reported that Doppler sonography can commonly depict large penetrating arteries, intratumoral flow, and peritumoral hepatofugal portal flow in patients with atypical high-flow hemangiomas with arterioportal shunt.2,3 Because the performance of Doppler sonography is generally attenuated with lesion depth, such findings are more commonly appreciated when the lesion is located shallow from the ultrasound transducer.2 In addition to the high-flow hemangiomas with arterioportal shunt, many hypervascular hepatic tumors other than, such as hepatocellular carcinomas, focal nodular hyperplasias, and hepatic adenomas may show intratumoral blood flow on Doppler sonography. However, the peritumoral hepatofugal portal flow is an uncommon finding among various hypervascular tumors other than high-flow hemangiomas with arterioportal shunt and hepatocellular carcinomas. Hepatofugal portal flow associated with hepatocellular carcinoma is usually seen in cases with tumor thrombus in the portal vein.4 Therefore, the presence of peritumoral hepatofugal portal flow on Doppler sonography in the absence of portal vein thrombus may be an important sign that enhance the suspicion of high-flow hemangiomas with arterioportal shunt.
It has been shown that the speed of enhancement on dynamic post-contrast study is correlated with the sonographic pattern. The tumors with rapid enhancement on dynamic studies tend to be hypoechoic sonographically, and those with slow enhancement tend to be hyperechoic.5 In addition, it is interesting that, in the presence of hepatic steatosis, an arterioportal shunt associated with high-flow hemangiomas may result in peritumoral sparing of steatosis. Some investigators speculated that the intrahepatic, regional alteration of portal flow (dilution of portal blood by nonlipid-rich arterial blood by arterioportal shunt) may be an important factor as the cause of the focal sparing of steatosis.6 Therefore, in the presence of hepatic steatosis, high-flow hemangiomas with arterioportal shunt tend to appear as hypoechoic masses surrounded by geographic peritumoral less hypoechoic area.7
SUMMARY
Arterioportal shunt accompanying hepatic hemangioma can be diagnosed on Doppler sonography, by demonstrating the hepatofugal flow at the peritumoural portal branch parallel to the feeder. In the presence of hepatic steatosis, an arterioportal shunt associated with high-flow hemangiomas may result in peritumoral sparing of steatosis so that the tumor appear as hypoechoic masses surrounded by geographic peritumoral less hypoechoic area. A precise sonographic appreciation of such findings may ensure an accurate sonographic diagnosis of these tumors.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




