

EPIDEMIOLOGY
Alcoholic liver disease continues to be a significant source of healthcare expenditure with increasing rates of hospitalization and increasing costs per hospitalization in large part from complications such as sepsis, acute renal failure, and gastrointestinal (GI) bleeding in patients with advanced forms of alcoholic liver disease.1 There is an increasing trend of transplantation for alcoholic liver disease with an approximately 45% increase in transplant registrations in the United States.2 This is likely to continue to increase in the setting of diminishing cases of hepatitis C-related cirrhosis over the future decades.
Alcohol-related liver disease can be defined both clinically and histopathologically.3 Steatosis is the earliest histopathologic lesion and frequently will have no clinical sequelae associated with it but would be detected on biopsies in most individuals who drink in excess for periods of time, even as short as one or few days. A smaller percentage of individuals will develop more advanced lesions characterized by inflammation and fibrosis. Alcoholic hepatitis is a specific histopathologic and clinical diagnosis characterized by inflammation usually in the setting of some degree of co-existing fibrosis and, in many cases, cirrhosis as well. Histopathology is also characterized by the presence of mega-mitochondrial and Mallory hyaline and balloon degeneration of hepatocytes.
A number of risk factors can exacerbate alcohol-related liver disease. Women are at greater risk for any given amount of alcohol consumption to develop alcohol-related liver problems.4 Obesity also exacerbates alcohol-related liver disease as does malnutrition.4 Patatin-like phospholipase domain-containing protein 3 (PNPLA3) is the most characterized polymorphism that predisposes towards more advanced alcohol-related liver lesions.5
More recently, binge drinking is becoming an increasing problem in the alcohol arena.6 Binge drinking is defined as 4 to 5 drinks over a 2-hour period that may achieve a blood alcohol level of 0.08 mg/dL as defined by the National Institute on Alcohol Abuse and Alcoholism (NIAAA). It's associated with social harm, crime, and increasing unplanned pregnancy. However, the effects of binge drinking on alcohol-related liver complications compared to drinking the equivalent amount of alcohol on a daily basis is uncertain, and one recent study suggests that daily heavy alcohol consumption may be worse than binge drinking, given any equal amount of units of alcohol consumed per week.6 There is also a pending crises relating to powdered alcohols which can be easily carried and dissolved in liquid or even snorted and regulations are ongoing at state and national levels to stem this potential epidemic. There may be benefits to small amounts of alcohol consumption of <14 units/day for men and <7 units/day for women.6 However, the therapeutic to toxic threshold of alcohol consumption is very narrow and alcohol consumption beyond these estimated and relative thresholds quickly increases alcohol-related liver problems and all cause morbidity and mortality.
DIAGNOSIS AND PROGNOSIS OF ALCOHOLIC LIVER DISEASE
One of the major controversies in the field of alcoholic hepatitis relates to the role of the liver biopsy.7 The major previously-discussed potential benefits of the role of liver biopsy in diagnosing alcoholic hepatitis is that alternative diagnoses have different therapies and therefore especially given the potential toxicity of therapies such as corticosteroids that a definitive diagnosis is required. Studies have shown that perhaps approximately 15% of cases where the diagnosis is presumed that clinical grounds may be incorrect.7 The cons or the downsides of a liver biopsy relate to the cost of the biopsy which often requires a transjugular approach and interventional radiology. The inconvenience of the biopsy is it may delay initiation of treatment and potential complications especially given the frequent coagulopathy and co-morbid illnesses in these individuals.
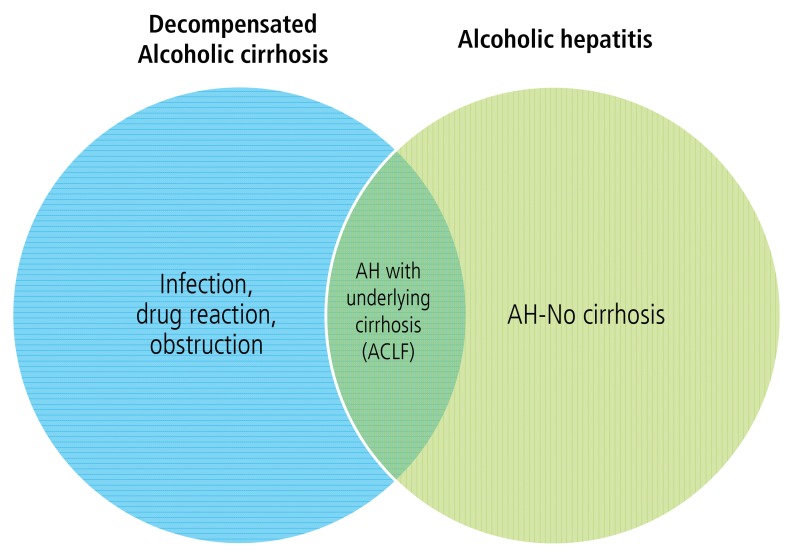
Is the history of alcohol consumption adequate to make the diagnosis of alcoholic hepatitis? The history is very difficult to obtain accurately. Some various approaches are used, particularly obtaining history from multiple sources including patient's family members, CAGE questionnaire where some more details are inquired relating to whether the patient has felt the need to cut back on their alcohol consumption, whether they get annoyed when other individuals ask them to cut back, whether they have guilt associated with alcohol consumption, and whether they require an eye opener, which is a drink in the morning. Two positive responses or one positive eye-opener response are generally suggestive of history of excess alcohol use. Laboratory markers can be helpful in predicting excess alcohol consumption, and some of them have been compiled together with demographic factors in the alcohol/nonalcoholic steatohepatitis index (ANI) which is originally designed to distinguish alcohol from nonalcoholic steatohepatitis (NASH) in individuals who have steatosis on a liver biopsy.8 This model uses the mean corpuscular volume (MCV), the asparate aminotransferase (AST)/alanine aminotransferase (ALT) ratio, the body mass index (BMI) and gender with a nomogram that's available at a web calculator (http://www.mayoclinic.org/medical-professionals/model-end-stage-liver-disease/alcoholic-liver-disease-nonalcoholic-fatty-liver-disease-index) to allow prediction of whether liver abnormalities may be relating to alcohol or non-alcohol related etiologies.8 We are now realizing that many patients may have a combination of both of these conditions as well as factored in the development of steatosis and liver problems, and even if the diagnosis of excess alcohol consumption is made, this may not always equate with alcoholic hepatitis. For example, alcoholic hepatitis may occur in the presence or absence of cirrhosis and in the absence of cirrhosis, the differential diagnosis may include biliary obstruction, Budd-Chiari Syndrome, or other causes of rapid increase in bilirubin. Furthermore, there is an overlap with decompensation of alcoholic cirrhosis or this turn of acute on chronic liver failure, and some of these individuals may have other causes for the rapid increase in bilirubin. This can be relating to infections and cholestatic reactions from infection, drug reactions or again biliary obstruction (Fig. 1). So the biopsy may help distinguish these alternative etiologies of hepatic decompensation in clinical scenarios where the diagnosis has been uncertain. However, in most clinical experts' viewpoint, the majority of cases certainly would not require a liver biopsy. The role of liver biopsy may be useful in clinical trials to assure the diagnosis; however, even in this setting, recruitment is markedly impaired when a liver biopsy is required for enrollment.
There are a number of advances in biomarkers recently in medicine, and one biomarker has been proposed for the diagnosis of alcoholic hepatitis. This biomarker relates to the detection of two breath products, one is trimethylamine (TMA), which is generated from the diet and metabolized through the liver to trimethylamine-N-oxide (TMAO) and thus the TMA measurement can help to predict alcoholic hepatitis based on increased gut permeability that increases TMA levels and impaired liver function that reduces the conversion of TMA to TMAO.9 Furthermore, pentane is a marker of oxidative stress that is also increased in alcoholic hepatitis, and a combination of these breath biomarkers has been proposed as a diagnostic test. This requires further validation.
Another potential role of liver biopsy has been proposed for prognosis of alcoholic hepatitis. In a recent study, the histologic score based on presence of fibrosis, neutrophil infiltration, bilirubin stasis, and mega mitochondria could independently predict 90-day mortality.10 Interestingly, neutrophil infiltration was actually protective in this study. How much a biopsy adds for prognosis compared to non-invasive models could be debated. For example, the discriminant function is a time-tested extensively-validated prediction model that is quite effective with a discriminant function of over 32, predicting about a 50% mortality. This is especially useful for steroid treatment since that's where it's been most expansively validated. However, some patients with a discriminant function of <32 still have a significant risk of death and so other models are also useful to provide more granular details as relating to death risk at various scores. The Model For End-Stage Liver Disease (MELD) score has been extensively validated for a variety of liver conditions including alcoholic hepatitis.11 There are some advantages to the MELD score over the discriminant function including that the INR is more accurate and available than the prothrombin time that's used in the discriminant function. The MELD score also has easily available calculators now (http://www.mayoclinic.org/medical-professionals/model-end-stage-liver-disease/meld-score-90-day-mortality-rate-alcoholic-hepatitis) and cut-points can be based on the toxicity of the proposed treatment.
If a patient is started on corticosteroids, it is important to assess their response after one week of treatment and to discontinue corticosteroids if the response is not appropriate. The response initially was proposed to be analyzed by changes in bilirubin at one week with individuals who have no improvement in their bilirubin to be discontinued from the steroids.12 Subsequently, a more refined score was also developed called the Lille score, which includes the bilirubin measurement plus some additional demographic and laboratory features.13 A Lille score over 0.45 after one week indicates patient is unlikely to response to steroids and who should have the steroids discontinued. Both of the scores are effective and simple analysis of a bilirubin at one week is sometimes adequate and quite easy to measure. Recently, some of these scores have been combined to see if they can provide even further prognostic value.14
A number of blood tests now are being proposed as potential markers of mortality and biomarkers for response to steroid as well. A recent study shows that lipopolysaccharides (LPS), which is the product of bacteria, can be measured and can be predictive of liver-related morbidity and mortality, which goes through a stepwise process of systemic inflammatory response syndrome, multi-organ failure, and death.15 Additional factors that could be predictive include procalcitonin and c-reactive protein; all part of the acute phase response. It has been proposed that these factors could be easily checked in the blood and may be effective for predicting which patients with alcoholic hepatitis will die. Paradoxically, although there is inflammation in alcoholic hepatitis, these patients are pre-disposed towards infection, and this happens through changes in a number of the blood cells whereby they are not able to achieve their function adequately.16 This may be because the LPS that is increased in alcoholic hepatitis may have adverse effects on these blood cells preventing them from doing their function. This may include effects on T-cells as well as leukocytes and their ability to phagocytose products, and this has significant effects on the risk of infection in a recent study out of a cohort of 94 patients with alcoholic hepatitis.16 Fifteen were found to have invasive Aspergillus with very detailed testing.17 The mortality of these individuals was severe. In fact, all of them succumbed to death by 60 days. Thus, the prevalence of fungal infections in patients with alcoholic hepatitis is high, especially those receiving corticosteroids, and additional screening and prophylaxis strategies may need to be considered in this population although perspective studies haven't been performed in this regard.
TREATMENT UPDATE IN ALCOHOLIC LIVER DISEASE
Owing to the significant healthcare utilization and prevalence of alcoholic liver disease, standardized cost effective patient-centered care models are underdevelopment to better manage this population. While aggressive treatment, such as liver transplantation, are considered for very few patients, there is important need for better management strategies of the larger patient base. Projects are focused on care team models which can focus on medical compliance, addiction issues, palliative care models, and psychosocial supports for these patients so that they have improved care coordination, enhanced quality of life, and reduce expenses and hospitalizations relating to their disease.
Other goals of treatment are to provide supportive care for nutrition and alcohol addiction. In fact, most pharmacotherapy helps only short-term survival in alcoholic hepatitis and after one month, pharmacotherapy has little beneficial effects in most trials. The bigger factors for survival at six months relate to abstinence and nutrition and then subsequently relate to the underlying cirrhosis and its complications. This highlights the importance of supportive care and nutritional support in these individuals and also suggests that potentially pharmacotherapy may need to be administered for longer than one month and that pharmacotherapy may be required for alcohol addiction as well.
Pharmacological options for abstinence are complicated by underlying liver disease. A recent study suggests that baclofen may be safe and effective in patients with alcoholic hepatitis.18 Two recent studies have shown no serious adverse effects of baclofen in this population in terms of liver or renal deterioration and beneficial effects on abstinence.18 Acamprosate is another compound that can be utilized in patients with earlier stage liver disease. Naltrexone has also been evaluated, although its safety is not established in advanced liver disease.
In terms of pharmacotherapies for alcoholic hepatitis itself, this is largely focused around corticosteroids and pentoxifylline. A recent survey study shows that despite guidelines supporting the role of corticosteroids is a primary therapy in selected populations, less than 50% of practicing clinicians utilize corticosteroids, and this is largely due to their concerns of infection and sepsis in these patients.19 The American Association for the Study of Liver Diseases (AASLD) guidelines from 2010 suggest that patients with severe disease as defined by discriminant function over 32, with or without hepatic encephalopathy, and there was lacking contraindications to steroid use such as GI bleeding and infection should be considered for prednisolone therapy.20 Alternatively, they can consider pentoxifylline therapy if they have contraindications to corticosteroids. However, a number of new studies have emerged since these guidelines were published. The most prominent study was published in the New England Journal of Medicine recently and was approximately a 1,000-patient study which is the largest to date which randomized patients to steroids versus pentoxifylline versus both versus placebo.21 Subsequently, analysis was done to compare the various arms with a combination of groups to compare the effects of individuals receiving prednisone versus no prednisone. There was a trend towards improved survival with prednisone, but this did not reach statistical significance with a P-value of 0.06 for one-month survival, and there was no benefit to six-month survival. In groups receiving pentoxifylline versus not, there was no beneficial effect of pentoxifylline and when comparing all the groups, essentially there was no significant difference between any of the groups. So, this study reduces enthusiasm for the use of pentoxifylline and also is essentially a negative trial for the role of corticosteroids albeit with a trend towards beneficial effect. This trial was also included a recently-conducted network meta-analysis of randomized control trials of alcoholic hepatitis network methodologies provide additional discrimination and power compared to traditional meta-analysis.22 This network meta-analysis to various trials that included corticosteroids, pentoxifylline and other combinations or associated combinations could all be compared. The summary results of this analysis showed that corticosteroids alone or in combination with N-acetylcysteine or pentoxifylline decrease short-term mortality based on moderate quality evidence. They show that pentoxifylline decreases short-term mortality and is comparable to corticosteroids based on low-quality evidence. No intervention was able to decrease medium-term mortality. Pentoxifylline, but no other interventions, decreases risk of acute kidney injury and no intervention, including corticosteroid base strategy increases the risk of infections. So there is some conflicting information between the meta-analysis and the large trial published in the New England Journal of Medicine.
A number of other recent trials have been published and may also provide guidance. In a recent study that was designed to test if pentoxifylline was equivalent to prednisone, 121 patients were randomized to one or the other drug, the drugs were not statistically equivalent in this inferred a beneficial role or prednisone compared to pentoxifylline.23 Another recent trial combining both drugs, corticosteroids, and pentoxifylline were not shown to be superior corticosteroid monotherapy.24 This was a very large trial with 270 patients and survival curve for interchangeable and two arms. All of these trials have been included in the network meta-analysis.22 Another recent trial shows that steroids plus anti-oxidants had no further beneficial effect compared to steroids alone, although there was a beneficial effect at one month.25 This was not the primary end-point, and the primary end-point was six months, where no beneficial effect was seen. It should be noted that prior studies have not shown beneficial effects of antioxidants such as N-acetylcysteine in alcoholic hepatitis.26 Another large study a few years' back showed the pentoxifylline does not improve survival in patients with alcoholic cirrhosis, many of whom had concurrent alcoholic hepatitis. Finally, conversion of steroid non-responders to pentoxifylline is also not effective since these individuals probably have a poor biology and regardless of which drug is used is not able to be effective.27 It's very important to develop a precision medicine approach in alcoholic hepatitis so that the right drug could be targeted, because there may be certain individuals who might benefit from corticosteroids, and this may not be detected in clinical trials where large cohorts of patients are all administered the same drug. A recent analysis is consistent with a number of other studies that were published that show that analysis of lymphocytes from patients with alcoholic hepatitis and in vitro measurement of their steroid sensitivity can predict in vivo clinical response to steroids as well.28 Such individualized medicine approaches are needed, and they also utilize genetic modifications that have been detected in patients with alcoholic liver disease such as PNPLA3.
Liver transplantation has recently been proposed for patients with alcoholic hepatitis and supported by a large well-conducted trial.29 However, the reality of the current era is that there are not adequate organs available for large populations of patients with alcoholic hepatitis. The study was published in the New England Journal of Medicine and showed that individuals who did not respond to corticosteroids after one week of attempted treatment will have markedly improved survival if they undergo liver transplantation. Transplantation was carried out quite quickly in this study within weeks, and they had two to three-fold improvement in survival compared to individuals who did not respond to steroids and did not undergo liver transplantation.29 Again, when the community is surveyed about liver transplantation for alcoholic hepatitis, approximately 30% of transplant centers have transplanted a patient for alcoholic hepatitis (A. Singal, personal communication - manuscript submitted). The information shows that approximately 50 liver transplants have been done for this indication in the United States, and the outcomes are quite reasonable with 90% one-year survival and the rate of alcohol relapse of less than 20%. Additionally, studies have recently shown that the outcomes of patients who undergo liver transplantation for alcoholic cirrhosis, as compared to those who have hepatitis on their explant is quite similar, again suggesting that hepatitis may have good outcomes after liver transplantation and similar to alcohol-related cirrhosis.30 The key factor is identifying the right patients who could undergo such an aggressive intervention and, in fact, very few individuals fall into this group. This requires coordinated interactions between a number of physicians in the team including the hepatologist, psychiatrist, surgeon, as well as the broader team including the social worker, addiction counselor, and the nurse coordinator (Fig. 2). Often times, a contract is pursued with the patient and a detailed psychosocial assessment is also performed. It's controversial whether patients should wait six months prior to undergoing liver transplantation. This delay can allow assessment of whether a patient will recover spontaneously and might not require liver transplantation.31 However, in the setting of alcoholic hepatitis, most individuals with severe disease will not survive six months and therefore attempts to treat their alcoholism during this time, which is another goal of the six-month delay, also cannot be pursued. Therefore, transplantation for alcoholic hepatitis probably is medically effective and patients would certainly have better outcomes than if they did not undergo transplantation. In the broader arena of alcoholic liver disease, a delay prior to transplant is useful to see the natural history of whether the patient may recover spontaneously with abstinence and also to undergo alcohol addiction treatment. However, in alcoholic hepatitis, a delay is probably not feasible. Overall relapse rates have been described with great heterogeneity, but probably occurring in about 1 in 5.31 However, the risk of graft loss from relapse is quite low. It's very important to select the right psychosocial patients and, in the setting of alcoholic hepatitis where alcohol consumption has occurred until very recently, there is very few of those individuals who will indeed qualify for this aggressive-type treatment. There are also a number of societal and logistical issues relating to the number of organs available and the high prevalence of alcohol-related liver disease, and societal perceptions may also be relevant since the majority of organs come from donated organs from the broader society. In summary, a very small percent of the total alcoholic hepatitis population of patients should be considered for such an aggressive treatment such as liver transplantation in the acute setting. These will be individuals with therapy failure, remarkably strong social support, positive factors for predicting long-term abstinence, and a lack of psychiatric co-morbidities.
In summary, individuals with a recent onset of jaundice and a history of heavy alcohol consumption and laboratory and clinical parameters consistent with alcoholic hepatitis can be evaluated for treatment with pharmacotherapy, and this may be stratified based on their discriminant function or MELD score and their other co-morbidities. Individuals at the present time with MELD scores <20 or discriminant function <32 should receive supportive care, management of liver complications, nutritional support and encouragement of abstinence. Individuals with scores higher than these cut-points, who do not have contraindications such to corticosteroids, could be considered for corticosteroids given all of the caveats of the recent trials that were shown, indicating that the largest recent clinical trial could not show a beneficial effect of corticosteroids, although there was a trend and that meta-analyses combining many trials showed and may still be a beneficial effect of corticosteroids. If corticosteroids are not used, it is appropriate to consider pentoxifylline, but the data is not very strong and therefore this simple conservative management without pharmacotherapy is also reasonable. If steroids are used, they should be discontinued at one week if there is no improvement in the bilirubin. A very small subset of patients could be considered for liver transplantation if they don't respond to steroids, but this will be less than 1% of these patients.
NEW CLINICAL TRIALS BASED ON NEW PATHOLOGIC CONCEPTS IN ALCOHOLIC LIVER DISEASE
In the normal liver, there is a stable situation between the intestines and the liver; there is a microbial population in the intestine. There are strong tight junctions in the epithelial cells that reduce the amount of microbial products that enter the liver. The liver also has feedback effects on the microbiome as well for release of bile acids. However, during alcoholic liver disease, it has been shown that alcohol causes a number of changes in the intestine including leakiness of the epithelial cells and impairment in the tight junctions as well as changes in the microbiota.32 This leads to the production of various bacterial products including endotoxin or LPS that goes to the liver and stimulates injury in the liver, which is also compounded by direct effects of alcohol on liver cells and alcohol metabolites. All of this in turn stimulates inflammation and fibrosis. Though a number of trials and studies are now proposed through the National Institutes of Alcohol and Alcoholism to combat this problem and this epidemic, these studies can be organized under three very broad concepts. One relates to targeting the intestine, another relates to targeting the injury response in the liver, and the third relates to targeting inflammation in the intestine.33 A number of approaches are targeting the microbiome and gut permeability while, in injury they target the alcohol effects and the toxin effects in the liver, and, during inflammation, they target white blood cells and cytokines. One example is the use of an anti-LPS antibody which can reduce the amount of LPS that crosses from the gut bacteria across into the blood vessels to the liver, and this is a study that is ongoing to the support of the NIAAA. Another study relates to the role of the protective cytokine interleukin-22 (Fig. 3). This is produced from blood cells and promotes liver repair.34 It also reduces liver fibrosis and does not cause immunosuppression, which is one of the major problems of most of the current drawings that are used in alcoholic hepatitis. Trials are ongoing in other conditions and will also commence in alcoholic hepatitis. Another interesting compound that is being studied is called Anakinra, which is an inhibitor of the interleukin-1 beta receptor.32 When hepatocytes are damaged by alcohol, they release interleukin-1 beta, and this stimulates activation of hepatic stellate cells and also recruitment of the inflammatory white blood cells, and Anakinra, by blocking the receptor for interleukin-1 beta on these cells, is able to reduce the effects of this interleukin-1 which has been termed the inflammasome response. A number of other trials are also ongoing that target the intestine injury and inflammation. These include studies evaluating zinc, obeticholic acid (which has received a great deal of attention recently for cholestatic disease and NASH) as well as CellCept, which is another immunosuppressant drug. Finally, on the horizon, newer therapies are also being evaluated that can target cytokine, that utilize antibiotics or probiotics and antioxidants, and further trials are awaited in this regard.
In summary, alcoholic liver disease will account for increase in percentage of liver disease case mix with declines in hepatitis C in the future. There is a need to focus on preventative standardized cost-effective healthcare approaches. The precise role of corticosteroids and pentoxifylline still remain undefined despite expansive study and highlights the need for individualized medicine approaches for this condition. Very selected patients with alcoholic hepatitis may be candidates for liver transplantation. Certainly, patients with alcoholic cirrhosis with established abstinence are very good candidates for transplantation. Ongoing studies are needed to further evaluate treatment options.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




