

INTRODUCTION
During the recent two decades, neucleos(t)ide analogues (NAs) have been a cornerstone in the treatment of chronic hepatitis B (CHB), targeting the reverse transcription of hepatitis B virus (HBV) polymerase.123 A high level of serum HBV DNA is known to be associated with the progression of hepatic fibrosis and the development of hepatocellular carcinoma (HCC).45 The wide use of antiviral agents with a low genetic barrier, such as lamivudine (LAM), adefovir (ADV), telbivudine, and clevudine (in Korea), as the first treatment option is one of main causes of the high prevalence of genotypic resistance to NAs among CHB patients in Asian countries.6 Especially, switching to ADV monotherapy instead of an add-on therapy increased the number of CHB patients with multidrug resistance or a suboptimal response to NA combination therapy.6789 Sequential ADV monotherapy after the emergence of LAM resistance failed to achieve an adequate virologic response in up to 25% of patients and additionally caused the development of genotypic resistance.1011 LAM and ADV combination therapy has also failed to achieve complete response in approximately 70% of LAM-resistant CHB patients.712 A suboptimal response to antiviral therapy might result in a higher risk of developing resistance to multiple NAs, leading to an increased risk of end-stage liver disease and HCC.1314 Therefore, most guidelines suggest that the ideal treatment for CHB is to reduce the serum HBV DNA level to below the detection limit of real-time polymerase chain reaction (PCR).13 There is little consensus on the adequate antiviral therapy for CHB patients showing a suboptimal response after LAM and ADV combination therapy. Before the approval of tenofovir (TDF), entecavir (ETV)+ADV was the most potent combination therapy for CHB patients with a suboptimal response to LAM and ADV therapy.15 As TDF was available in clinical practice, it became an important potent NA used as an antiviral regimen against CHB.16
Therefore, in this study, we aimed to compare the efficacy of ETV and TDF combination therapy with that of ETV and ADV therapy in CHB patients with genotypic resistance to LAM who showed a suboptimal response to LAM and ADV combination therapy.
PATIENTS AND METHODS
Eligible patients
We reviewed 258 CHB patients who developed genotypic resistance to LAM during LAM therapy at Kyungpook National University Hospital and Kyungpook National University Medical Center between 2009 and 2011, and identified 63 patients with a suboptimal response to LAM and ADV combination therapy.
The inclusion criteria were CHB patients (i) with serum HBV DNA level of >20 IU/mL during at least 3-month intervals after the treatment with LAM and ADV for at least 12 months, (ii) those with documented genotypic resistance to NAs, and (iii) those aged from 16 to 80 years.
The exclusion criteria were patients with (i) coinfection of chronic hepatitis C virus or human immunodeficiency virus; (ii) serum creatinine level of >1.5 mg/dL; (iii) decompensated liver cirrhosis; (iv) HCC; (v) diagnosis of a malignancy other than HCC within 3 years or an untreated malignancy; (vi) current alcohol or substance use; and (vii) major organ transplantation including the heart, lungs, and kidneys.
Study design
Of the 63 patients with a suboptimal response to the combination of LAM and ADV during at least 12 months, 30 patients received ETV and ADV (ETV+ADV group) and the remaining 33 patients received ETV and TDF (ETV+TDF group). We evaluated the liver function parameters, serum creatinine level, HBeAg positivity, prothrombin activity, platelet counts, and imaging tests for the diagnosis of liver cirrhosis. The serum HBV DNA level was quantified with a real-time PCR assay (Amplicor HBV Monitor Test; Roche Diagnostics, Basel, Switzerland; detection limit, ~12 IU/mL). Serum blood samples were stored for the analysis of the resistance profile of NAs. Multiplex restriction fragment mass polymorphism assays of the HBV genome were done to analyze the genotypic resistance profiles at baseline.
The primary end-point of the study was the rate of virologic response at 12 months (VR12, serum HBV DNA <20 IU/mL in realtime PCR). The secondary end-points included virologic response at 6 months (VR6, serum HBV DNA <20IU/mL in real-time PCR), serum HBV DNA reduction during the follow-up period, factors associated with VR12, and the rate of loss or seroconversion of HBeAg in patients with the antigen. The study protocol was approved by the local ethics committee and was conducted in accordance with the principles of the Declaration of Helsinki.
Definition of treatment response
The serum HBV DNA level was assessed every 3 months during the first 12 months. Virologic response was defined as a serum HBV DNA level of <20 IU/mL. Suboptimal response was defined as a decrease in serum HBV DNA level of >2 log10 IU/mL at 24 and 48 weeks after therapy without a virologic response. The upper limit of normal alanine aminotransferase (ALT) was defined as 30 IU/L in men and 19 IU/L in women.
Statistical analysis
The variables were expressed as mean with standard deviation, or number with percentage. Categorical and continuous variables between groups were analyzed by using the chi-square test and Student t-test, respectively. The cumulative probability of VR12 during treatment was calculated with the Kaplan-Meier method and compared with a log-rank test. The mean reductions of serum DNA level between the groups were analyzed by using the Student t-test. Factors related to achieving VR12 were analyzed by using the logistic regression model with backward elimination. P-values <0.05 ware considered statistically significant. All data were analyzed by using SPSS (version 20.0; IBM, Somers, NY, USA).
RESULTS
Baseline characteristics of the patients
A total of 63 patients were included in the study. Thirty patients were treated with a combination of ETV and ADV (ETV+ADV group), and 33 patients were treated with a combination of ETV and TDF (ETV+TDF group). There was no significant difference between the two groups except for ETV resistance mutation (Table 1). Overall, 55 (87%) patients were HBeAg positive and 24 patients were found to have liver cirrhosis on the basis of ultrasonography findings. The mean serum HBV DNA level of the patients was 4.61 log10 IU/mL at baseline. In the HBV mutation test at baseline, all patients had a LAM resistance mutation, including rtM204V/I (n=61, 96.8%) and rtL180M (n=43, 68.3%). Approximately half of the patients had an ADV resistance mutation, including rtA181V/T (n=30, 48%) and rtA181V/T+rtN236T (n=9, 14%). Although it was observed in a relatively small proportion of patients, ETV resistance mutation was more frequent in the ETV+TDF group than in the ETV+ADV group (n=4, 13% vs. n=12, 36%; P=0.036). However, there was no significant difference between the two groups in multidrug resistance, defined as the presence of resistance mutation with LAM+ADV or LAM+ETV (n=17, 57% vs. n=20, 61%; P=0.751).16
Virologic response
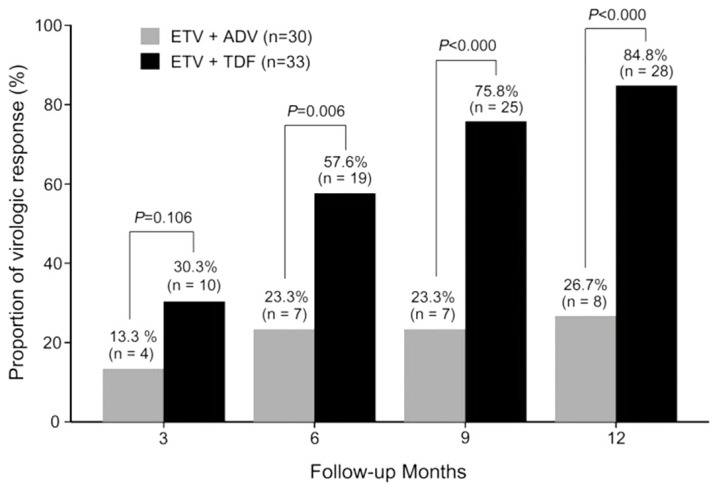
The primary end-point, the proportion of patients who achieved VR12, was significantly different between the two groups (26.7% vs. 84.8%, P<0.001) (Table 2, Fig. 1). The rate of patients who achieved VR6 was significantly higher in the ETV+TDF group than in the ETV+ADV group (23.3% vs. 57.6%, P=0.006). In univariate analysis for factors associated with achieving VR12, a lower serum baseline HBV DNA level and rescue therapy with ETV+TDF were associated with achieving VR12 (Table 3). In multivariate analysis with the logistic regression model, patients with a lower baseline serum HBV DNA level (odd ratio [OR], 0.19; 95% CI, 0.07-0.50; P=0.001) and rescue therapy with ETV+TDF (OR, 54.78; 95% CI, 7.15-418.54; P<0.001) had a significantly higher probability of achieving VR12. However, the HBV resistance mutation profiles, including ADV, ETV, and multidrug resistance, were not associated with VR12 in both univariate and multivariate analyses.
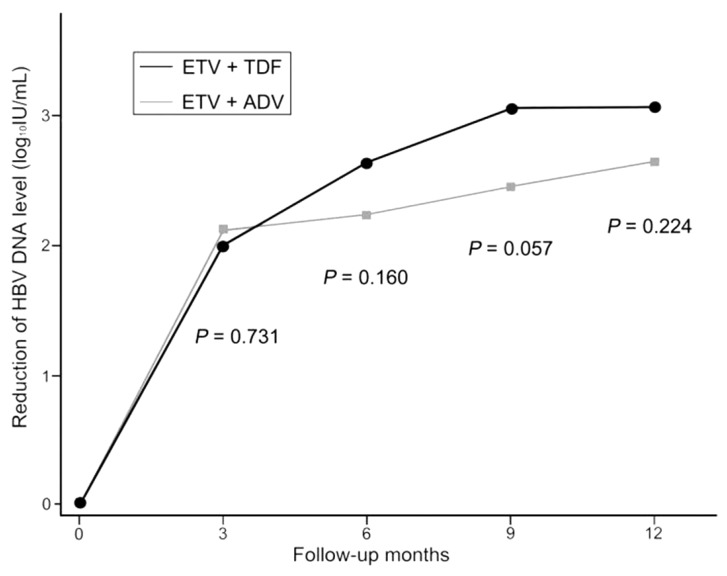
The serum HBV DNA level tended to decrease more in the ETV+TDF group than in the ETV+ADV group (Table 2, Fig. 2). Both the ETV+ADV and ETV+TDF groups showed an initial rapid reduction of serum HBV DNA level during the first 3 months (2.12 log10 IU/mL vs. 2.00 log10 IU/mL, P=0.731). While the serum HBV DNA level showed further decreases at 9 months in the ETV+TDF group (2.40 log10 IU/mL vs. 3.02 log10 IU/mL, P=0.057), the serum HBV DNA level at 12 months did not differ significantly between the ETV+ADV and ETV+TDF groups (2.60 log10 IU/mL vs. 3.02 log10 IU/mL, P=0.224).
Safety
No serious adverse effects of antiviral agents were observed during the treatment period in both groups. None of the patients experienced elevation of serum creatinine of ≥0.5 mg/dL or a serum ALT flare-up (>10-fold of the normal upper limit). All patients continued antiviral agent treatment without dose interruption.
DISCUSSION
After the approval of ETV and TDF, the management of CHB has markedly improved during the last decade.123 ETV and TDF, which have a high genetic barrier to resistance development, are the most potent NAs for the suppression of viral load in CHB patients.1718 The 5-year resistance rate to ETV and TDF was reported to be 1.2% and 0%, respectively, in NA-naïve CHB patients1718 However, in cases with the presence of LAM resistance, this profile is disappointing. In patients with LAM-resistant CHB, ETV monotherapy showed virologic, serologic, and biochemical improvement for 48 weeks.1920 As LAM-resistant HBV is less susceptible to ETV, the probability of achieving an adequate virologic response is lower in patients with LAM-resistant HBV than in NA-naïve patients.1920 Moreover, the emergence of ETV resistance mutation is more frequently observed during the long-term treatment of patients with LAM resistance.20 In this regard, previous multiple sequential monotherapy or use of NAs with a low genetic barrier induced the sequential development of resistance mutations. Multidrug resistance not only led to viral breakthrough but also limited the future therapeutic options. For these reasons, appropriate combination therapies are important in patients with multidrug-refractory CHB.
In a prior study, the combination of ETV and ADV was shown to suppress HBV replication significantly without the development of additional resistance mutation for 52 weeks in suboptimal responders to LAM and ADV.21 However, the proportion of virologic response was only 28.9% in patients treated with ETV and ADV combination therapy, which was similar to the results of our study. In the present study, the treatment for 1 year with the combination of ETV and TDF showed a significantly higher proportion of achieving VR12 than the combination of ETV and ADV in patients with NA-resistant HBV who showed suboptimal responses to the combination of LAM and ADV (ETV+ADV, 26.7% vs. ETV+TDF, 84.8%). However, the genotypic resistance profiles, including LAM, ADV, ETV, and multidrug resistance, did not affect the cumulative probability of achieving VR12. In the subgroup analysis, 9 patients with the rtA181T/V+rtN236T double mutation at baseline were treated with ETV+ADV (n=5) or ETV+TDF (n=4). HBV with rtA181T/V+rtN236T double mutation is known to reduce the virologic response in the treatment with TDF or with a combination of LAM and TDF in patients with a prior failure of LAM and ADV combination therapy.22 However, in patients with the rtA181T/V+rtN236T double mutation at baseline, the proportion of VR12 was similar to those of the entire study population (ETV+ADV, 40% vs. ETV+TDF, 75%, data not shown). This result was supported by a recent study that showed a negative association between predictors of virologic response and the genotypic resistance profile during ETV+TDF combination therapy.23 In another subgroup analysis, 6 patients with LAM, ETV, and ADV resistance mutation at baseline were treated with ETV+ADV (n=2) or ETV+TDF (n=4). Three patients (75%) who were treated with ETV+TDF achieved VR12, whereas none of the patients treated with ETV+ADV achieved VR12 (data not shown). However, these subgroup analyses were limited by the relatively small number of patients. Liver cirrhosis and HBeAg positivity also did not affect the suppression of HBV DNA level during the antiviral therapy. Only higher baseline HBV DNA levels independently predicted an unfavorable virologic response during the treatment with the combination of ETV and TDF. HBeAg loss or HBeAg seroconversion was not observed among patients with HBeAg at baseline during the entire study period. Although the mechanism was unknown, this result suggests that it is difficult to achieve serologic response in patients with a suboptimal response to LAM and ADV, regardless of rescue therapy.192124
TDF, which is metabolized by the kidneys, may induce renal proximal tubulopathy and cause renal tubular dysfunction.25 In the present study, no worsening of renal function was observed in patients during the antiviral therapy.
This study has some limitations owing to its retrospective design. In the baseline genotypic resistance profiles, ETV resistance mutation was more frequently found in patients treated with ETV and TDF. However, a previous study showed that genotypic resistance to ETV did not associate with the probability of virologic response during TDF rescue therapy.26 In addition, in a recent study that showed the efficacy of ETV and TDF combination therapy for multidrug-resistant CHB patients, the proportion of achieving VR12 was 79.6%, which was similar to the results in our study. The other limitations were the short study duration and the requirement for the evaluation for subsequent genotypic resistance mutation at 12 months. At present, although the development of subsequent genotypic mutation after an ETV and TDF combination therapy is not well known, a relatively high rate of VR12 could be expected to lower the possibility of additional genotypic mutation development.1314 Nevertheless, further long-term prospective studies might be needed to investigate the subsequent development of genotypic mutation.
In summary, this study demonstrated that the efficacy of ETV and TDF combination therapy is significantly higher than that of ETV and ADV combination therapy in patients with NA-resistant CHB who showed a suboptimal response to LAM and ADV. Regardless of the HBV genotypic resistance profile, the baseline serum HBV DNA level was independently associated with the cumulative probability of achieving virologic response during rescue therapy in patients who failed treatment with LAM and ADV. Because of the absence of important adverse effects or dose interruption, ETV and TDF were continued during the study period.
In conclusion, regardless of the HBV genotypic resistance profile, the efficacy of the ETV and TDF combination therapy is superior to that of ETV+ADV in patients with NA-resistant CHB who showed a suboptimal response to both LAM and ADV.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




