

INTRODUCTION
The hepatitis C virus (HCV) infection was discovered fairly recently, and HCV infection is now known to exhibit a higher rate of transition into chronic infection, compared to hepatitis B virus (HBV) infection. However, an HCV vaccine has not been developed (despite the development of an HBV vaccine); therefore, HCV infection is difficult to prevent. As with HBV infection, when an HCV infection transitions into chronic infection, it can subsequently result in cirrhosis, hepatic decompensation, and hepatocellular carcinoma.1
The global prevalence of HCV infection is known to be approximately 3%, although the prevalence in Asia is typically reported to be 1-2%, with the exception of several countries.2 In Korea, the reported prevalence varies according to the clinical features of the target population, age, and region; the reported prevalence ranges from 0.41% to 2.1%.3
A recent large-scale Korean study has targeted participants receiving a medical checkup, and reported that the age-, sex-, and area-adjusted anti-HCV positive rate was 0.78%. In contrast, the rates in Busan and Jeonnam were reported to be 1.53% and 2.07%, respectively, which were more than double the national average.4 Another study that used Korean national health insurance data reported that Busan exhibited the highest prevalence, followed by Jeonnam and Gyeongnam.5
However, the study didn't compare the prevalence according to region, age, or sex, and the indirect method for standardization has made direct comparisons difficult. Therefore, in-depth analysis of HCV infection's epidemiologic features is needed to establish policies for the management and prevention of HCV infection in high-prevalence regions. This study compared the prevalences in 16 Korean cities and provinces over an 8-year period, using Korean national health insurance data. For high-prevalence regions (Busan, Gyeongnam, and Jeonnam), the characteristics of the prevalences were analyzed through investigation according to cities and towns there in detail.
MATERIALS AND METHODS
We retrospectively reviewed Korean national health insurance (NHIS) data between 2005 and 2012 to identify cases of HCV infection. This data covers the entire Korean population through the National Health Insurance Program and the Medical Aid Program for low-income households. The subjects of the study were defined as those who visited medical facilities and were diagnosed or received treatment for acute (B17.1) or chronic HCV (B18.2) as a primary or a secondary disease according to ICD-10 code. When a patient received treatment for the same disease several times in a year, this was only counted as one patient in that year.
The registered population at the end of each year was used as the denominator for the yearly prevalence. In this study, we only included patients who were Ōēź20 years old, as this population is most comparable to international studies (which typically target adult patients) and the prevalences among younger patients are very low. To correct for the effect of the age structure of population by year and region, the age-adjusted prevalence was calculated using the direct method, based on the registered population in 2010. The age of each patient was recorded as the age on the final day of treatment in the relevant year.
The study was approved by the Institutional Review Board (IRB) of Inje University hospitals and National Cancer Center (NCC2014-0182).
RESULTS
In Korea, approximately 60,000-70,000 adults (Ōēź20 years old) receive treatment for HCV infections each year. The national prevalence of HCV infection gradually increased from 0.14% in 2005 to 0.18% in 2012. Busan exhibited the highest prevalence (2005: 0.34%, 2012: 0.37%) among the regions that were examined, and this prevalence was approximately double the national average.
The prevalence of Busan for the last 8 years showed gradual increase from 0.34% to 0.37%. Jeonnam and Gyeongnam provinces also had elevated prevalences of 0.32% and 0.24%, respectively (Table 1).
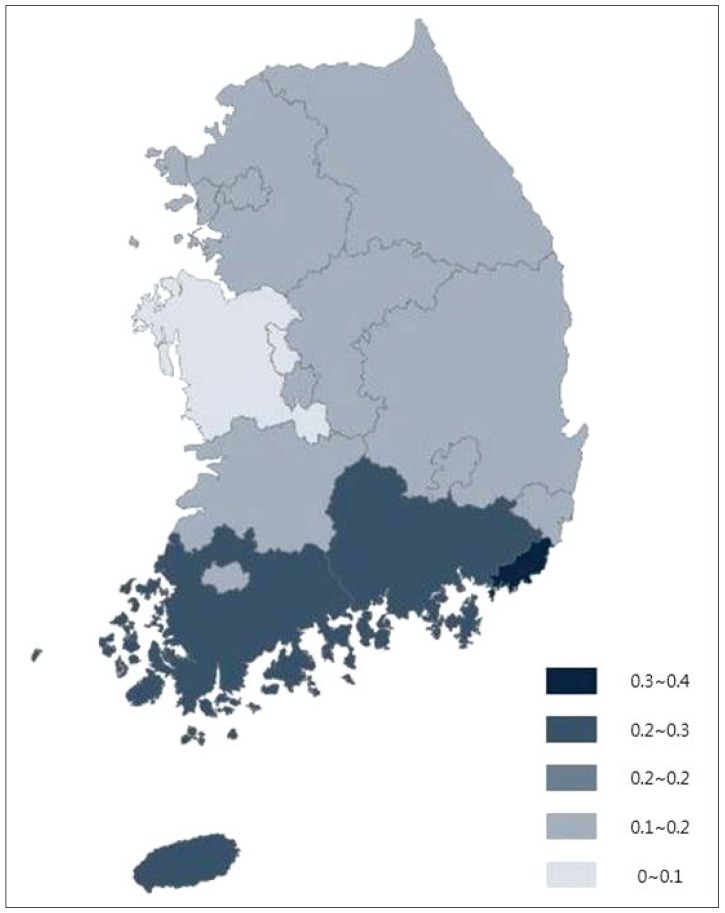
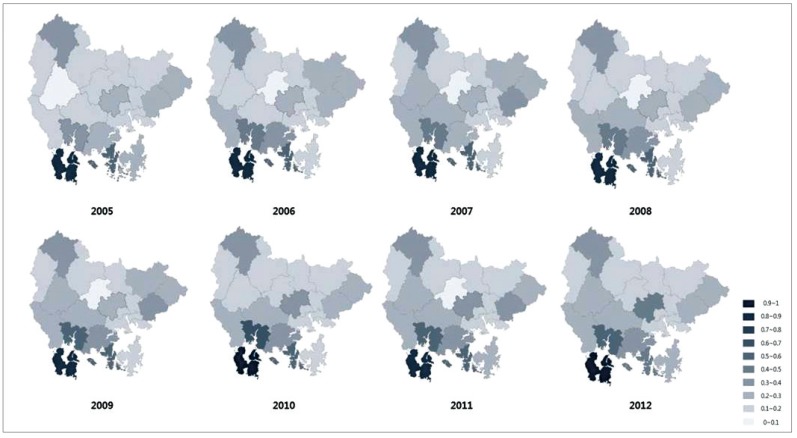
According to the age and region-adjusted prevalence of HCV infection in 2012, there was no significant difference according to sex, with prevalences of 0.19% for men and 0.18% for women. However, the prevalence according to age exhibited a significant increase with increasing age, from 0.04% among those who were 20-29 years old to 0.38% among those who were 60-69 years old. According to the region, the prevalence in Chungnam was the lowest (0.06%) and the prevalence in Busan (0.35%) was approximately 6-fold higher than that in Chungnam (Table 2). Figure 1 shows a regional map of the HCV infection prevalences, and the southern region (E.g., Busan, Gyeongnam, Jeonnam, and Jeju) typically had high prevalences.
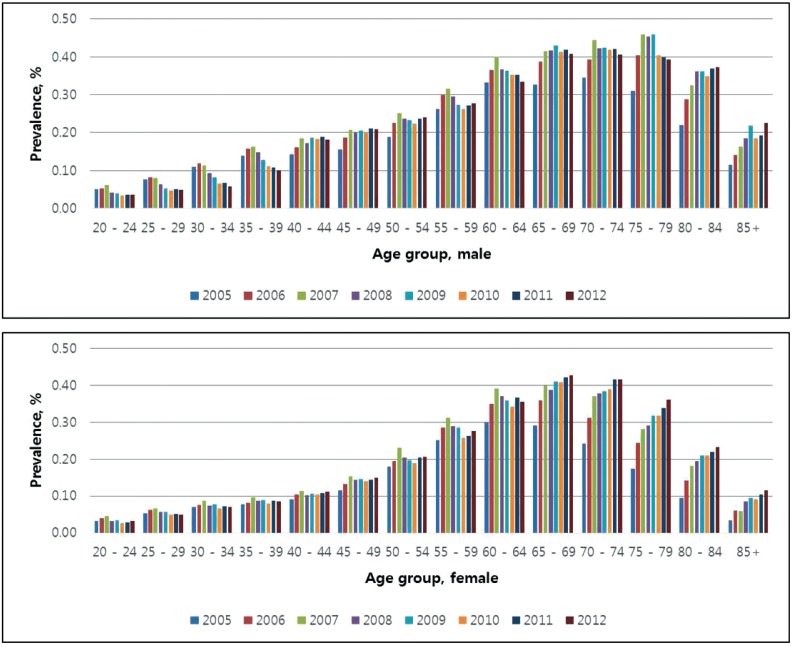
Regarding changes in age- and sex-specific prevalences, the prevalence among men continuously increased from the 20-29 year old group to the 70-79 year old group, and then decreased. The prevalence among women also gradually increased with age, although the rate of the increase was smaller than that among men and it was similar to that among men who were 55-59 years old, and peaked among women who were 65-69 years old. This trend was observed consistently from 2005 to 2012, although the prevalence increased over time, and the group with the highest prevalence also grew older over the study period (Fig. 2).
Regarding the prevalences according to sex and age in the high-prevalence regions, Busan and Gyeongnam exhibited a recent decreasing trend among men who were <40 years old, and a gradually increasing trend among men who were >45 years old. Similar trends were observed among younger women (who were 40-49 years old showed a slow decrease) although older women exhibited an increasing prevalence. In Jeonnam, both men and women who were >65 years old exhibited gradually increasing prevalences recently, while no significant change was observed among those who were <65 years old. (Supplementary Fig. 1, 2, 3)
In Busan, men exhibited a higher prevalence (0.46%) than women (0.36%), and a sharp increase was observed among those who were 40-49 years old; this trend continued into the 60-69 year old group (Supplementary Table 1). Among the towns in Busan, the prevalence in Seo-gu has consistently been the highest since 2005 (2005: 0.86%, 2012: 0.89%), followed by that in Jung-gu (0.65%) and Yeongdo-gu (0.49%). The prevalence in Jung-gu increased from 0.58% in 2005 to 0.67% in 2012, and the prevalence in Dong-gu also increased from 0.28% to 0.40% over the same period (Supplementary Table 1, Fig. 3).
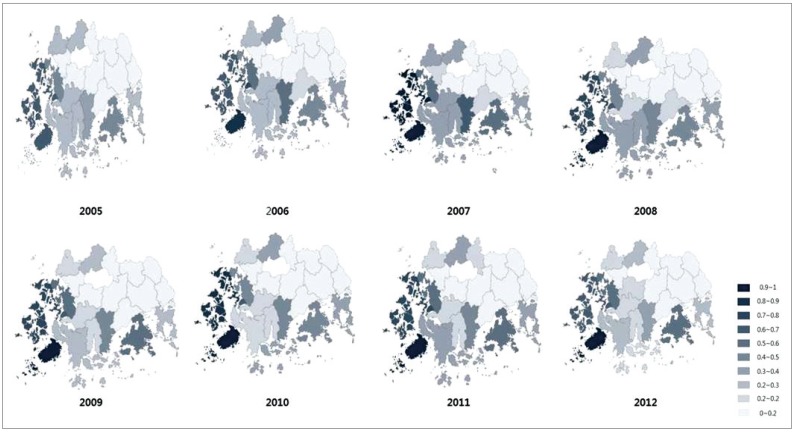
In Jeonnam, only a minor difference in sex-specific prevalence was observed (men: 0.34%, women: 0.31%), although the age-related prevalence increased noticeably (50-59 years old: 0.42%, 60-69 years old: 0.70%). Among the towns in Jeonnam, Jindo exhibited the highest prevalence in Korea (0.97%), followed by Mokpo (0.70%) and Shinan (0.68%) (Supplementary Table 2, Fig. 4). The age-adjusted prevalence in Jindo exhibited an especially large increase from 0.66% in 2005 to 0.96% in 2012; this was the greatest increase among the high-prevalence cities and provinces.
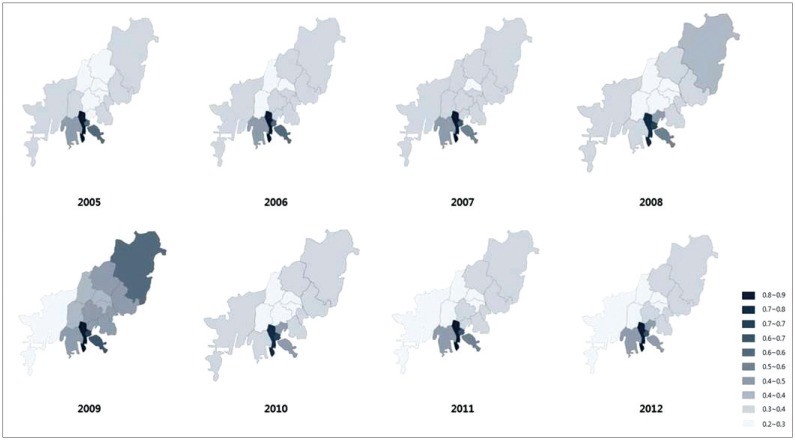
In Gyeongnam, the prevalence among men was 0.31% and the prevalence among women was 0.27%; those who were 60-69 years old exhibited the highest prevalence (0.50%). Among the towns in Gyeongnam, Namhae had the highest prevalence (0.90%), followed by Sacheon (0.59%) and Tongyoung (0.48%) (Supplementary Table 3, Fig. 5).
DISCUSSION
Our results indicate that the prevalence of HCV infection among Korean adults (Ōēź20 years old) who visited medical facilities for diagnosis or treatment of HCV increased gradually from 0.14% in 2005 to 0.18% in 2012.The exact reason for the increase in the number of patients with HCV infection is not known. It may be due to the increase of people who participate in medical check-up or the inclusion of HCV infection test in the medical check-up list. Busan exhibited the highest regional prevalence, followed by Jeonnam and Gyeongnam. Among the towns, Jindo (in Jeonnam) exhibited the highest prevalence (0.97%), followed by Namhae (0.90%) in Gyeongnam and Seo-gu (0.86%) in Busan. These prevalences are all approximately 5-times higher than that of the national average. In the high-prevalence regions, prevalences tended to increase with age (similar to the national trend), and significantly higher rate was observed among men compared with women while greater increase was found among older age groups in these high-prevalence regions. In Korea, HCV infection is not classified as a national notifiable disease; therefore, there are no relevant national data. However, one large-scale study targeted participants who were >20 years old and who received medical checkups in 30 tertiary hospitals nationwide, and the study found that the age-, sex-, and area-adjusted anti-HCV positive rate was 0.78%. However, it was difficult to accurately identify actual number of HCV infected patients, as not all anti-HCV-positive people receive treatment for this infection.4
Another study used the national health insurance data in Korea, and reported that the prevalence among all age groups ranged from 0.12% to 0.13% between 2007 and 2011.5 However, the study did not include cases of acute HCV infection, and only included cases in which the patient received treatment for HCV infection as the primary diagnosis, which likely explains why our prevalence is slightly higher, as we also included cases with a secondary diagnosis of HCV infection.
In previous studies, the reported prevalences of HCV infection vary according to region and target group. For example, studies that have evaluated the anti-HCV positive rate targeting participants in medical checkups have suggested very different results, including 0.41% among adults in Seoul (>20 years old) from 1995 to 1998,6 1.31% among adults in Ulsan (>20 years old) in 1997,7 2.1% among adults in Jeonnam (>30 years old) from 1998 to 2000,8 and 0.89% among adults in Daegu (>20 years old) from 1997 to 2001.9 The reason for the differences in the prevalence presented in the previous studies is because the scope of study subjects and the method of calculating the prevalence rate are different. For the case of hospital-and community-based cohort, the prevalence shows the anti-HCV positive prevalence which includes recovered patients who had HCV infection in the past and for the case of community-based cohort, although it is possible to estimate prevalence in a specified region, it requires a large-scale cohort with at least 100,000 people because HCV infection has low prevalence. Likewise, the present study shows the different result compared to the previous studies because it includes only those who received treatment for HCV infection for that year. In addition, one study, which conducted a pooled analysis of all studies from the 1990s, reported that the prevalence among Korean adults who are >40 years old was 1.68% (95% CI: 1.51-1.86) and that the prevalence among men (0.77%, 95% CI: 0.72-0.83) was slightly lower than the prevalence among women (1.06%, 95% CI: 0.97-1.16).10 These results are noticeably different from the findings of the present study.
Our analysis of the town-specific prevalences in the 3 main high-prevalence regions revealed alarming results. Among the towns in Busan (which had the highest prevalence in Korea), Buk-gu and Sasang-gu had the lowest prevalence (0.28%), although this was still higher than the national average. In addition, Seo-gu had the highest prevalence (0.86%) in Busan, and this was more than 3-times higher than the lowest prevalence in Busan. Unfortunately, the reason(s) for the significantly elevated prevalence in Seo-gu are not clear.
It is possible that Seo-gu had a higher diagnosis rate for HCV infection, as 3 of 4 university hospitals in Busan are located in Seo-gu. However, Dong-gu and Jung-gu (which are neighbor towns of Seo-gu) exhibited the greatest increase in the prevalence of HCV infection in Busan over the last 8 years. Therefore, attentive management of HCV infection is needed in these areas.
In Jeonnam, the lowest prevalence was observed in Seoncheon and Ganggyeong (0.11%), and other cities with a prevalence below the national average were Gogseong (0.13%), Damyang (0.14%), Gurye (0.15%), Boseong (0.15%), and Hwasoon (0.16%). In contrast, Jindo had the highest prevalence of all Korean cities/towns (0.97%), and this was more than 8-times higher than that in Seoncheon and Ganggyeong.
One previous study has targeted participants at their medical checkups in Gwangju and Jeonnam, and that study reported that the age-adjusted anti-HCV positive rate was higher in Jeonnam (2.7%) than in Gwangju (1.6%).4 In addition, among the 80 persons who were anti-HCV positive in Jeonnam, those who lived near the seaside (3.5%, 45/1,274) were more likely to be anti-HCV positive than those who were living inland (2.2%, 35/1,554); even after age-adjustment, the positive rate near the seaside (3.7%) was higher than that of inland (2.2%).8
Our study also found that inland areas in Jeonnam had prevalences below the national average, compared with other areas in Jeonnam, and that Jindo and Shinan (located in seaside area) had high prevalences.
In Gyeongnam, the prevalence in Namhae (0.90%) was 7.5-times higher than that in Uiryeong and Habcheon (0.12%). Therefore, further studies are needed and the implementation of disease control policies that focus on small areas with demonstrated high prevalences should be considered, as many relatively close towns (even in the high-prevalence regions of Busan, Jeonnam, and Gyeongnam) exhibit significant differences in prevalence. Although these small areas are all located near the sea, it would be difficult to confirm whether proximity to the sea is a risk factor for HCV infection, as there is a low prevalence even in areas near the sea.
Among the 16 cities and provinces that were examined, Jeju exhibited the greatest increase in the age-adjusted prevalence, with a rapid increase from 0.15% in 2005 to 0.23% in 2012. One study in Tsushima, Japan has also reported that the anti-HCV positive rate in the southwest coast of Japan was significantly higher than that in other regions, although no specific causal factor was identified.11
Our results indicate that the annual prevalence of HCV infection in Korea has gradually increased, and that the infection has spread, given the yearly increases in prevalence among older age groups in the high-prevalence regions (despite a decreasing trend among younger age groups). This finding may be related to insufficient treatment, despite a previous report that the success rate for treatment of HCV infection is very high in recent years.12
One study has surveyed 18,636 patients at the National Cancer Center in Korea (from 2002 to 2008) regarding their awareness of HCV/HBV infection. Among the participants, 74.2% of HBV carriers (904 persons, 5% of the study population) were aware that they were infected with HBV, although only 34.9% patients who were anti-HCV positive (146 persons, 0.8% of the study population) were aware of their infection.13 Therefore, the actual number of patients with HCV infection is likely higher than that indicated by the prevalence reported in this study. The limitation of this study is that the prevalence is based only on those patients who visited the medical center for HCV because the health insurance data were used. Furthermore, it excludes those who did not receive the treatment after diagnosed with HCV as well as those who are not aware of their HCV infection status. Therefore, the prevalence calculated in this study is the prevalence of HCV-infected patients who received the treatment, not the prevalence among all patients who are infected with HCV. However, the present findings are likely representative of Korean patients, as Korean health insurance covers whole nationals, and all hospitals and clinics treat patients who are covered by the health insurance program.
The reason(s) for these high prevalences in those specific regions should be identified, as this could help prevent HCV infection in the future. In addition, active treatment policies should be introduced to stop any further spread of infection in these high-prevalence regions.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Supplement1
Supplement1 Print
Print




