Differences in the patterns and outcomes of enhanced viral replication between hepatitis C virus and hepatitis B virus in patients with hepatocellular carcinoma during transarterial chemolipiodolization
Article information
Abstract
Background/Aims
Enhanced replication of hepatitis C virus (HCV) is well described in the setting of moderate to severe immunosuppression. The aims of this retrospective study were to determine the incidence of enhanced HCV replication in hepatocellular carcinoma (HCC) patients undergoing transarterial chemolipiodolization (TACL) and to identify the factors associated with enhanced replication of HCV. The clinical pattern of enhanced HCV replication was compared with hepatitis B virus (HBV) reactivation during TACL.
Methods
This study enrolled 49 anti-HCV-seropositive patients who were diagnosed with HCC between January 2005 and December 2010 and who underwent TACL using epirubicin and/or cisplatin with consecutive HCV RNA copies checked. For comparison, 46 hepatitis B surface antigen1-positive patients with HCC who were treated with TACL were also enrolled. The frequency, associated factors, and clinical outcomes of enhanced HCV replication were analyzed and compared with those of HBV reactivation during TACL.
Results
Enhanced replication of HCV occurred in 13 (26.5%) of the 49 anti-HCV-seropositive patients during TACL. Of these 13 patients, 4 developed hepatitis, but none of the subjects developed decompensation due to the hepatitis. No significant clinical factors for enhanced HCV replication during TACL were found. Compared with HBV reactivation, the frequency of hepatitis attributed to enhanced HCV replication was significantly lower than that for HBV reactivation (8.2% vs. 23.9%, P=0.036).
Conclusions
TACL can enhance HCV replication; however, the likelihood of hepatitis and decompensation stemming from enhanced HCV replication was lower than that for HBV reactivation in patients undergoing TACL.
INTRODUCTION
Hepatitis C virus (HCV) is a major public health problem, with approximately 170 million people infected, corresponding to about 3% of the population worldwide. HCV causes a high rate of chronic infection, resulting in severe complications of chronic liver disease such as liver cirrhosis (LC) and hepatocellular carcinoma (HCC).1 Regarding disease progression, the host immune response has a unique role in HCV infection because it contributes not only to viral control and clinical recovery but also to chronic hepatitis and liver cirrhosis. The coordinated activities of cellular immune responses are initiated on antigen-presenting cells and play critical roles in the control of HCV replication. However, mutations in viral epitopes targeted by cytotoxic CD8+ T cells can allow the virus to escape immune-mediated clearance, leading to chronic hepatitis and liver cirrhosis.2
An immune-compromised status, such as after liver transplantation, can enhance HCV viral replication, and it is probably secondary to impairment of cellular immunity. Likewise, data from patients infected with HCV receiving cytotoxic chemotherapy for hematological malignancies show that liver dysfunction by enhanced replication of HCV may be a possible complication, whereas it is less common and less severe than that due to hepatitis B virus (HBV) reactivation.3-5 However, cases of severe hepatitis with hepatic decompensation from enhanced HCV replication have been reported.5
Transarterial chemo-embolization (TACE) has become the most common non-surgical management for unresectable HCC. Because TACE increases the survival rates in patients with unresectable HCC, it is currently considered the primary therapy.6-8 However, TACE is not indicated for those with poor hepatic reserve, as it is related to more complications and worse prognoses in those cases. Yoshikawa et al9 indicated that transarterial chemo-lipiodolization (TACL) may be a successful alternative for the palliative treatment of high-risk HCC patients with poor hepatic reserve. Using an infusion of a lipiodol emulsion mixed with anticancer drugs via the hepatic artery, micro-embolization of tumor vessels and slow release of anticancer drugs from the lipiodol were achieved. However, this procedure can also lead to worsening of liver function, although the frequency was relatively low.9
TACL was reported to possibly reactivate HBV replication in HBsAg-positive HCC patients irrespective of baseline viral status.10 According to that study, performed at our institution, HBV reactivation during TACL resulted in hepatitis, hepatic decompensation, and even death.10 However, no detailed study has examined enhanced HCV replication in HCC patients during TACL. In this retrospective study, the frequency, associated factors, and clinical outcomes of enhanced HCV replication were analyzed and compared with those of HBV reactivation during TACL.
PATIENTS AND METHODS
Patients
From January 2005 to December 2010, 71 patients who were diagnosed with unresectable HCC at Liver Clinics of Seoul St. Mary's Hospital and Incheon St. Mary's Hospital, were positive for anti-HCV antibody, and who had both basal and follow-up HCV RNA titers checked were included in the study. The exclusion criteria for these patients were as follows: extrahepatic metastasis, main portal vein thrombosis, and positive results for HBs Ag or human immunodeficiency virus (HIV). As a result, 13 patients were excluded from the analysis. Primary treatments for the remaining 58 patients were TACL (n=49), external radiation (including cyberknife therapy) (n=3), and conservative management (n=6). The diagnosis of HCC was based on histologic evidence or elevated serum α-fetoprotein (AFP) levels (>400 ng/mL) with typical radiologic findings.
For the comparisons, 116 consecutive patients with positive HBsAg newly diagnosed with unresectable HCC were included. Patients were excluded from the study if they fulfilled any of the following criteria: a previous history of antiviral therapy for HBV, extrahepatic metastasis, a serum HBV DNA level greater than 107 copies/mL, main portal vein thrombosis, or positive tests for antibody to hepatitis C virus or human immunodeficiency virus. Finally, 46 patients were eligible for analysis. There was a discrepancy in the year of enrollment between HCV and HBV seropositive groups because preemptive lamivudine treatment during TACL has been used after February 2005.
Laboratory tests
Seropositivity for anti-HCV antibody was determined using third-generation enzyme immunoassays (Abbott Laboratories, North Chicago, IL, USA). Baseline HCV RNA titers were checked before commencement of treatment, and follow-up titers were checked before each course of treatment using real-time polymerase chain reaction (Biosewoom, Inc. Seoul, Korea). All patients were followed up at intervals of less than 2 months. At baseline, HCV genotype was determined by the VERSANT HCV genotype assay (LiPA 2.9, Belgium). All patients were tested for HBsAg, antibodies to HBsAg (anti-HBs) (Abbott Laboratories, IL, USA), and HIV at the time of enrollment. Serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin, bilirubin, alkaline phosphatase, gamma glutamyl transpeptidase, prothrombin time, and AFP were checked before each course of treatment and again when necessary.
HBV DNA test (VERSANT 3.0, branched DNA assay, Bayer HealthCare LLC, Tarrytown, NY, USA; detection range: 2×103 to 1×108 copies/mL) was performed before each course of treatment and again when necessary. Genotyping of HBV was performed via ELISA (Institute of Immunology, Tokyo, Japan) using monoclonal antibodies to the preS2 region, as previously described.11 All patients were followed up at intervals of less than 2 months in a similar manner to those with positive anti-HCV antibodies.
TACL-related ischemic injury of the liver can also elevate liver enzymes, but it did not seem to last more than two weeks.10 We checked the liver enzymes at least 1 month after prior TACL to discern hepatitis due to enhanced viral replication from ischemic injury.
Definitions
Enhanced replication of HCV was defined as the reappearance of HCV RNA for spontaneously resolved or treated patients or an increase of over 10 fold in serum HCV RNA compared with the baseline level. Hepatitis attributed to enhanced HCV replication was defined with a three-fold or greater increase in serum ALT level that exceeded 100 IU/L (reference range, <36 IU/L) in patients with HCV reactivation in the absence of clinical features of tumor progression, hepatotoxic drugs, treatment-related hepatic damage, or other systemic infections. Hepatic decompensation during TACL was defined by the occurrence of any one of the following: newly developed encephalopathy or ascites, increase in the prothrombin time by >3 second greater than the level before TACL, and increase in the bilirubin level to twice the upper limit of normal (ULN) (reference range: <1.2 mg/dL) if initially normal or an increase to twice the baseline level if initially abnormal.
We defined HBV reactivation as reappearance or an increase of over 10 fold in serum HBV DNA compared with the baseline level, as mentioned in previous reports.12,13 Hepatitis attributed to HBV reactivation and hepatic decompensation during TACL were defined in the same manner as enhanced HCV replication.
Treatment methods
The assignment of treatment options for unresectable HCC is done according to a standard protocol developed by the Barcelona Clinic Liver Cancer Group.14 Specifically, patients with a single nodule less than 5 cm in diameter or up to three nodules less than 3 cm in diameter were considered candidates for radiofrequency ablation, percutaneous ethanol injection therapy, or liver transplantation as available. For patients with HCC beyond this tumor extent, transarterial chemotherapy was performed for Child-Pugh classification A, whereas suboptimal or conservative management was given for Child-Pugh classification B or C. TACL was usually performed at 1- to 2-month intervals. The chemotherapeutic regimens used for TACL included epirubicin (50 mg/m2) or doxorubicin (25-70 mg) monotherapy, cisplatin monotherapy (60 mg/m2), and epirubicin and cisplatin combination therapy. Lipiodol (5-10 mL) was given with each regimen during the procedure, but Gelfoam® was not used. No patients were given glucocorticoid therapy.
Statistical analyses
Analyses were conducted using the independent-sample t-test, Mann-Whitney U-test, chi-square test, or Fisher's exact test, as appropriate. Two-tailed P-values <0.05 were considered significant. Significant variables from the univariate analysis were then included in a multivariate analysis using a logistic regression model to identify the independent predictors of each phenomenon. Data were analyzed using SPSS software (SPSS 15.0; SPSS, Inc., Chicago, IL, USA).
Ethics statement
The study was approved by the Ethics Committee of the Catholic University of Korea (KC11RISI0508). All subjects provided signed informed consent to participate in this research study.
RESULTS
Study population
Table 1 shows the baseline characteristics of all 95 patients newly diagnosed with HCC and either HCV or HBV seropositivity who underwent TACL as their initial modality of treatment. Among 49 patients positive for HCV, detectable HCV RNA was observed in 41 patients, and HCV RNA was below 50 copies/mL for eight patients. It is impossible to test HCV genotype in patients with HCV RNA titers below 10,000 copies/mL, and 36 patients had HCV genotype tested. Among them, 19 (52.8%) patients were genotype Ib, and 17 (47.2%) patients were other types.
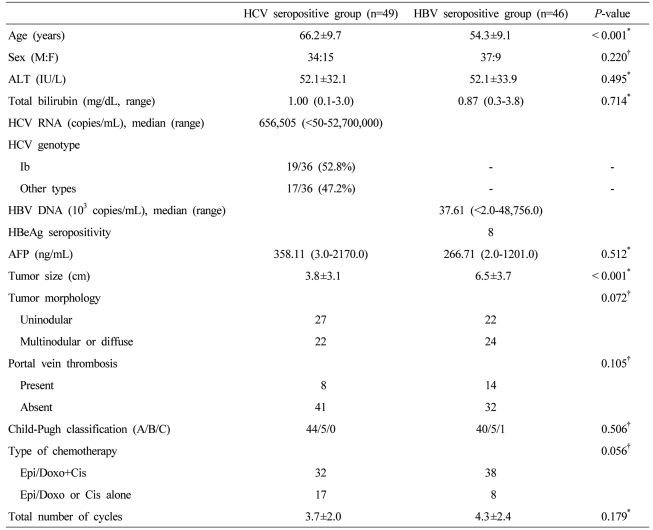
Baseline characteristics of the entolled patients
In the HBV seropositive group, eight (17.4%) patients were HBeAg-positive. For 13 patients, HBV DNA was below 2000 copies/mL, and they were all HBeAg negative. HBV genotyping performed in 46 patients showed that all were genotype C (100%).
The age of diagnosis and tumor size was significantly different between these two groups. The patients in the HBV seropositive group were younger, and their tumor size was larger.
Enhancement of HCV replication and occurrence of hepatitis compared with HBV reactivation
Table 2 summarizes the frequency of enhanced viral replication, hepatitis attributed to enhanced viral replication or other causes, and hepatic decompensation.
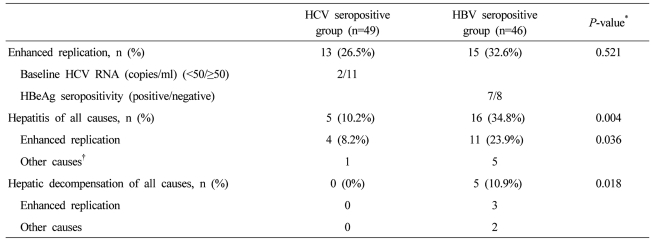
Comparison of enhanced viral replication, hepatitis, and hepatic decompensation in the HCV- and HBV-seropositive groups during transarterial chemolipiodolization (TACL)
Among 49 HCV seropositive patients who underwent TACL, 26.5% (13/49) developed increased HCV replication during the follow-up period. Hepatitis attributed to enhanced HCV replication was observed in 8.2% (4/49) of patients, and there was no case of hepatic decompensation. Two patients initially had undetectable HCV RNA titers but later developed enhanced viral replication. One patient had no history of treatment, and the other had received interferon therapy 10 years before diagnosis of HCC. Both of these patients developed hepatitis attributed to enhanced viral replication.
Eleven out of thirteen patients with enhanced HCV replication, including three patients with hepatitis, got subsequent TACL, although the time interval between each subsequent TACL was longer than scheduled with three hepatitis patients. None of the patients with enhanced HCV replication during TACL underwent further antiviral treatment.
Comparison of the HCV seropositive group (n=49) with the HBV seropositive group (n=46) revealed no significant difference in the frequency of viral reactivation. However, statistically significant differences were observed in the frequency of hepatitis (P=0.036) due to viral reactivation and hepatic decompensation (P=0.018) between these two groups. The mean number of treatment cycles to enhanced viral replication was 2.3 for HCV seropositive group (n=13) and 1.9 for HBV seropositive group (n=15), but the difference was not statistically significant.
The clinical features of four patients with hepatitis attributed to enhanced HCV replication during TACL are shown in Table 3. The elevation of ALT was mild, except in one person (patient 2), who had a past history of excessive alcohol use. Hepatitis due to enhanced HCV replication was usually milder than in cases with HBV reactivation, with a median ALT level of 142.5 IU/L versus 303.5 IU/L, respectively. None of the four patients with hepatitis evidenced hepatic decompensation due to enhanced HCV replication during TACL. Follow-up HCV RNA was checked in three of four patients with variable time intervals, and HCV RNA titer and ALT level decreased without antiviral treatment (Table 3).
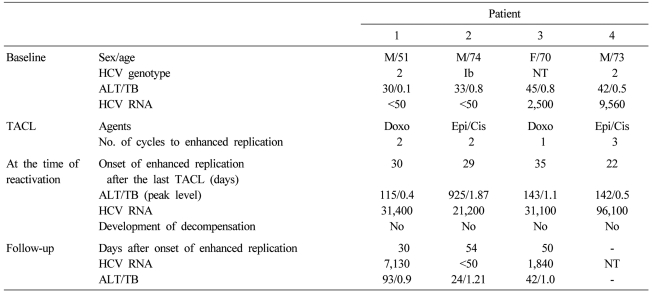
Characteristics of the four patients with hepatitis attributed to enhanced replication of HCV
Factors associated with enhanced HCV replication
To evaluate the clinical factors related to the enhancement of HCV replication during TACL, 10 variables were compared in patients with and without enhanced HCV replication during TACL (Table 4). No statistically significant factors were found, including baseline HCV RNA copies or HCV genotypes.
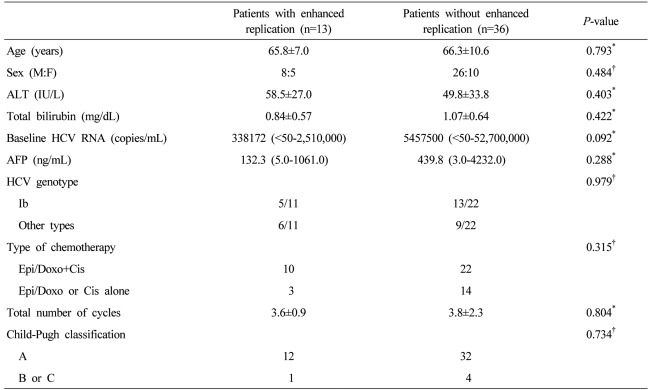
Univariate analysis of factors related to enhanced replication of HCV during TACL
DISCUSSION
The reactivation of hepatitis virus during systemic chemotherapy for malignancies is a significant problem that can lead to hepatic failure.15 The mechanism of viral reactivation is unclear but may involve a two-stage process, as described by Xunrong et al.16 The first or initial stage is characterized by a dramatic increase in viral replication and active infection of hepatocytes while the patient is being treated with cytotoxic agents. After withdrawal of the cytotoxic agents, a second stage with restoration of the immune function mediated by T-cells and destruction of infected hepatocytes occurs.17 This immune reconstitution phase can lead to biochemical and clinical hepatitis, with transient elevation of ALT, possible jaundice, development of constitutional symptoms, and even hepatic decompensation. This process has been emphasized more frequently in HBV infection than in HCV, and preemptive antiviral therapy against HBV has been proven to be efficacious to prevent hepatitis attributed to viral reactivation during systemic chemotherapy and TACE.17-22
TACL has been shown to reactivate HBV infection in previous reports, and its immunosuppressive effect on chemotherapeutic agents infused during TACL was the suggested mechanism.10,19 HCV replication was also enhanced during TACL, and no statistically significant difference in the frequency of viral reactivation between HBV and HCV was observed in this study. However, no relevant clinical factors that contributed to HCV reactivation during TACL were identified. Previous studies reported that genotype 2c carriers are at high risk of hepatitis reactivation in an untreated cohort of patients with chronic HCV infection.23 There was also a case series suggesting that HCV genotype 2 might be a risk factor for reactivation in patients with B-cell lymphoma undergoing rituximab combination chemotherapy.24 But we were unable to identify an association between enhanced replication of HCV and viral genotype.
Interestingly, two patients with initially undetectable HCV RNA titers later developed enhanced viral replication. Anti-HCV positive patients without HCV RNA for more than 6 months are considered to be cured of hepatitis C. These patients have cleared the virus either spontaneously or due to treatment. Of our two patients, one had no history of treatment, and the other had undergone interferon therapy. It is generally believed that hepatitis C virus is not completely eliminated from the body but is under control of the immune system. HCV RNA has been reported to be present in the liver and peripheral blood mononuclear cells of patients with no detectable serum HCV RNA.25,26
The possible cause for enhanced replication of HCV during TACL can be suggested, considering the attenuated activity of cellular immune response in liver by TACL. Previous studies showed that HCV viremia recurred in a patient and in a chimpanzee after serum samples consistently tested negative for HCV RNA using a nested reverse-transcription PCR method for 4 months after normalization of ALT levels.27,28 In both cases, loss of HCV specific CD4+ T-cell responses preceded HCV recurrence. Additionally, in vivo depletion of CD8+ T cells resulted in prolonged viremia, which was controlled only when HCV-specific CD8+ T cells reappeared in the liver.29 Taken together, these studies indicate that the adaptive cellular immune system, whose important components are CD4+ and CD8+ T cells, is crucial in controlling HCV replication, and attenuated activity of the cellular immune response can result in enhanced HCV replication in the liver.
Our study showed that the hepatitis and/or hepatic decompensation attributed to enhanced replication of HCV during TACL was significantly less frequent than that of HBV. This phenomenon may be the result of different immunogenic characteristics between these two viruses. A recent study described that human HCV-specific T cells differ in their effector functions from human HBV-specific T cells. Whereas HBV-specific CD8+ T cells express high levels of perforin and show vigorous proliferation, IFN-γ production, and cytotoxic activity on in vitro stimulation,30 these effector functions are reduced in HCV-specific T cells.30-32 The different degree of cytotoxicity between HBV-specific and HCV-specific CD8+ cells may contribute to a different pattern of viral reactivation and of hepatitis due to reactivation.
Additionally, HCV has escape mechanisms that contribute to the high chronicity rate of the viral infection and the attenuated course of new infections. These escape mechanisms might also prevent serious immune-mediated hepatic damage after enhanced viral replication during TACL. One important escape mechanism is viral-sequence mutations,33 and several other mechanisms might also contribute to the observed impairment of HCV-specific immune responses.
In conclusion, TACL can enhance replication of HCV, but the possibility of hepatitis and hepatic decompensation attributed to enhanced HCV replication would be lower than that of HBV reactivation in patients undergoing TACL. This discrepancy may result from differences in immunogenicity between HBV and HCV. Further prospective studies with large numbers of patients are required to confirm this suggestion. Concomitantly, the necessity of preemptive and/or targeted antiviral therapy for enhanced HCV replication during TACL should be evaluated.
Abbreviations
HBV
hepatitis B virus
HCV
hepatitis C virus
TACL
transarterial chemolipiodolization
TACE
Transarterial chemo-embolization
AFP
α-fetoprotein
ALT
alanine aminotransferase