A case of pedunculated hepatic hemangioma mimicking submucosal tumor of the stomach
Article information
Abstract
Hepatic hemangioma is the most common benign tumor of the liver. Most such hemangiomas are small, asymptomatic, and have an excellent prognosis. Giant hepatic hemangioma has been reported in the literature, but the exophytic and pedunculated forms of hepatic hemangioma are rare. A 56-year-old woman was referred to our hospital under the suspicion of having a gastric submucosal tumor. Abdominal computer tomography (CT) scans showed a pedunculated mass from the left lateral segment of the liver into the gastric fundus, exhibiting the atypical CT findings of hepatic hemangioma. We therefore decided to perform laparoscopic resection based on the symptoms, relatively large diameter, inability to exclude malignancy, and risk of rupture of the exophytic lesion. The pathology indicated it to be a cavernous hemangioma of the liver. Herein we report a case of pedunculated hepatic hemangioma mimicking a submucosal tumor of the stomach due to extrinsic compression of the gastric fundus.
INTRODUCTION
Hepatic hemangiomas are the most common benign tumor of the liver, which occur more frequently in woman. They are usually solitary and the lesions are frequently in subcapsular location, more commonly in the right lobe, especially the posterior segment. They are usually less than 3 cm in diameter. Those larger than 4 cm have been classified as giant hemangioma.1
Although most hepatic hemangiomas are asymptomatic and discovered incidentally,2 large lesions may cause a variety of symptoms such as abdominal mass, pain, hemorrhage, jaundice, nausea, vomit,1,3 and are associated with Kasabach-Merritt syndrome characterized by thrombocytopenia and consumptive coagulopathy.1,4 Exophytic forms of hepatic hemangiomas, especially pedunculated forms are very rare.5,6
We recently experienced pedunculated hepatic hemangioma that could be misdiagnosed as gastric submucosal tumor (SMT) caused by extrinsic compression. Herein, we report our case together with a review of the literatures.
CASE REPORT
A 56-years-old woman was referred to our hospital under the suspicion of having a 4 cm-sized SMT in the gastric fundus on the upper gastrointestinal series (Fig. 1). From one year ago, she had epigastric discomfort and dyspepsia, nonetheless, weigh loss was not shown. She had been diagnosed as chronic hepatitis B 18 years ago, but not performed regular examinations. She denied any medication and family history of diseases.

UGI findings showed an intraluminal protruding mass (arrows) of about 4.5 cm at the fundus, covered with normal gastric mucosa.
At the time of admission, blood pressure was 120/80 mmHg, pulse rate was 70/minute, respiration rate was 20/minute, and body temperature was 36.7℃. On physical examination, there were no abnormal findings. Esophagogastroduodenoscopy showed a 4 cm-sized mass in the gastric fundus, which was covered with normal gastric mucosa. When pushed with a pair of forceps, it could not be pushed and the change of its shape during inhaling and exhaling was observed. Dynamic abdominal computed tomography (CT) scan showed two masses. The one was well demarcated 3 cm sized mass in the right posterior superior portion of the liver (segment 7), showing hypoattenuation on precontrast images and centripetal fill-in of the contrast material after administration of contrast material. Whereas, the other was 4.5 cm sized pedunculated mass originated from the left lateral segment of the liver compressing the gastric fundus and showed inhomogeneous enhancement (Fig. 2). Complete blood count, liver function test and blood coagulation test were within normal ranges. Tumor markers including α-fetoprotein, carcinoembryonic antigen, carbohydrate antigen 19-9 and protein induced by vitamin K antagonist-II, were all within normal ranges. In regard to viral markers, hepatitis B surface antigen and hepatitis B e antigen were positive, and serum HBV-DNA level was more than 1×108 copies/mL.

CT scans revealed two hemangiomas; one was in segment 7 and the other was a pedunculated mass of the left lobe that showed inhomogeneous enhancement on the delayed phase (A, precontrast; B, arterial phase; C, delayed phase). It was connected to the left lateral segment of the liver by a thin neck and it compressed the gastric fundus (D-F).
She had epigastric discomfort and the pedunculated mass of the left lobe had atypical CT findings unlike the lesion in the right lobe, which made it difficult to differentiate from malignant tumor. Also, there was the possibility of rupture. Taken together, it was an indication of surgical treatment. Therefore, we decided to laparoscopic resection because it had a long peduncle and its resection was considered to be easy. During surgery, a mass with a long peduncle originated from the left lateral segment compressing the gastric fundus was observed. In gross anatomy, the size was 4.5×2.5×1.2 cm, the surface was smooth, and the color was dark red (Fig. 3A). The cut section showed spongy-shaped cystic lesions beneath the capsule (Fig. 3B). In microscopic examinations, there were various sized, large vascular channels, which were lined with single-layered flattened endothelial cells (Fig. 4A) and separated and supported by fibrous septa (Fig. 4B). After operation, the patient was discharged without complications, and currently, she is under the regular follow-up for chronic hepatitis B.

The external surface was bulging slightly (A), and a cut section showed a dark-red spongy-like soft mass beneath the capsule (B).
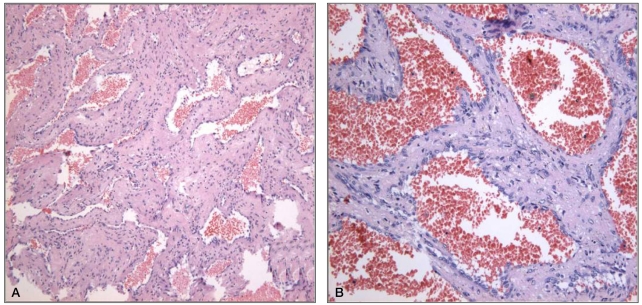
Microscopic examinations showed large vascular channels of various sizes (A: H&E stain, ×100) that were lined with single-layer flattened endothelial cells and separated and supported by the fibrous septa (B: H&E stain, ×400).
DISCUSSION
Hemangioma is the most common benign tumor of the liver, and a diagnosis of typical hemangioma is rather straightforward with the combination of various imaging techniques.5 In the upper gastrointestinal series, extrinsic compression could be observed in the lesser curvature of the stomach.7 In our study, it was misdiagnosed as gastric SMT caused by extrinsic compression of the gastric fundus because of the pedunculated characteristic. Typical hemangioma presents a homogenous, hyperechoic mass with well defined margin on ultrasonography, and early peripheral enhancement of the tumor on dynamic contrast CT, followed by centripetal fill-in of the contrast medium with persistently enhancement on delayed phase images.1,5,7,8 Magnetic resonance imaging also may provide more specific diagnostic features for hemangioma, especially small hemangioma, including markedly high signal intensity on T2-weighted images.1,5,9 Nonetheless, only 55-62% of the hepatic hemangioma shows typical features in image modalities.1 As in our case, giant hemangioma could show inhomogenous enhancement on CT images and it is very important to distinguish hemangioma from other hepatic neoplasm.1,8,10 Although angiography has been regarded as gold standard test for hemangioma, it is invasive. Therefore, recently, it is applied only to cases difficult to differentiate from other neoplasm in other image modalities.1,11
Hemangioma has female predominance and may occur in all age groups but more frequently in the 30-50s, and the mean age is 44 years.12 It is usually solitary and the lesions are frequently in subcapsular location, more commonly in the right lobe, especially the posterior segment. It is usually less than 3 cm in diameter.1 Brancatelli et al13 have reported that 12% of hemangiomas demonstrate exophytic growth. However, as in our case, pedunculated cases are very rare.9,14,15
Although most hemangiomas are asymptomatic, larger lesions may produce a variety of symptoms such as abdominal mass, pain, early satiety, nausea, vomit, jaundice, hemorrhage, and even rupture. Also, giant hemangioma may cause congestive heart failure result from arteriovenous shunt which is caused by hemangioma, and is associated with Kasabach-Merritt syndrome characterized by thrombocytopenia and consumptive coagulopathy.1,16
Hemangioma is usually small in size and asymptomatic and thus follow-up is considered enough without treatment. However, some cases need treatment for symptoms (palpable mass, pain, etc.), increasing size, uncertain diagnosis and complications (consumptive coagulopathy, rupture, etc.).3-5,12,17 Although most hemangiomas rarely increase in size or rupture, the possibility of its rupture increases in giant hemangioma.5,18 In our case, we decided to perform laparoscopic resection considering symptoms, relatively large diameter, inability to exclude malignancy and risk of rupture of the exophytic lesion. Regarding the treatment, surgery is principle.4,7,12 As in our case, if it is pedunculated mass, laparoscopic resection could be considered depending on the size and location of hemangioma.3,19,20 If there are contraindications to surgery, other treatment modalities such as radiation therapy, hepatic artery ligation and transcatheter arterial embolization could be performed, nonetheless, they do not produce satisfactory and sustained outcomes.4,12
Exophytic hemangiomas are rare. Moreover, pedunculated cases as our patient misdiagnosed as gastric SMT due to the extrinsic compression of the gastric fundus are very rare. In our case, laparoscopic resection was performed considering symptoms, inability to exclude malignancy due to atypical CT findings and risk of rupture of the exophytic lesion. However, even if it is asymptomatic and has typical features of hemangioma in imaging modalities, surgical treatment should be considered because of the risk of rupture.
Abbreviations
CT
computed tomography
SMT
submucosal tumor