

INTRODUCTION
IgG4-related autoimmune disease is a recently recognized clinical entity associated with autoimmune pancreatitis, various systemic extrapancreatic lesions and an elevated serum IgG4 level.1 IgG4-related sclerosing cholangitis (IgG4-SC) is one of the extrapancreatic manifestations of this entity, which needs to be differentiated from primary sclerosing cholangitis (PSC) as these two diseases appear similar at presentation, but follow different clinical courses. In this issue, we will discuss the histopathologic findings of IgG4-SC based on a liver biopsy case of a 65-year-old patient with autoimmune pancreatitis.
CASE SUMMARY
A 65-year-old previously healthy male presented with sharp epigastric pain and fever for the past two days. He had received a pylorus-preserving pancreaticoduodenectomy under the impression of a distal common bile duct cancer 3 years ago. He had a smoking history of 40-packs per year and a recent history of alcohol ingestion before surgery. Initial aspartate aminotransferase and alanine aminotransferase levels were 147 IU/L and 150 IU/L, respectively. The initial laboratory data showed an increased white blood cell count (13,300/┬ĄL) and C-reactive protein level (5.3 mg/dL). Serologic markers for hepatitis B surface antigen (HBsAg), IgM anti-HBc, IgM anti-hepatitis A virus antibody, and anti-hepatitis C virus antibody were all negative. Tumor markers and antinuclear antibody were also negative. Abdominal computed tomography and ultrasonography demonstrated a soft tissue infiltration around the common hepatic duct with bile duct dilatation and an ill-defined thickening of the bile duct wall at the hilar portion, suggestive of IgG4-SC. Serum IgG4 level was increased up to 196 mg/dL, and the serum IgG4/IgG ratio was 16.6%. A needle biopsy of the liver was performed.
PATHOLOGIC FINDINGS
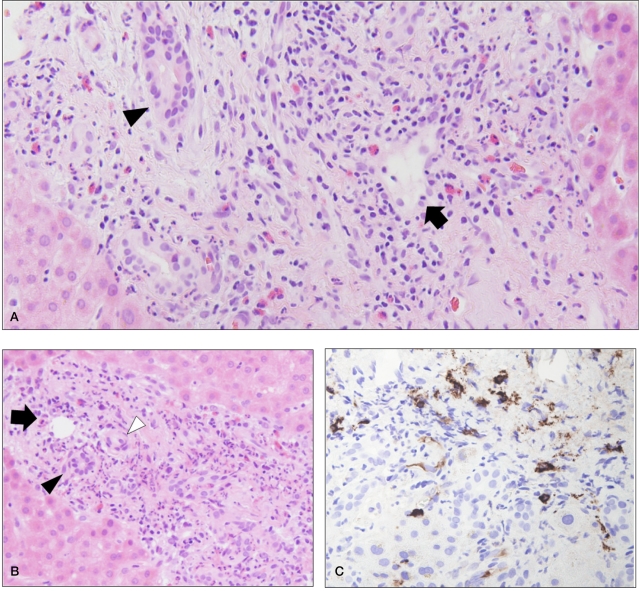
Microscopic evaluation of liver biopsy revealed moderate inflammatory cell infiltrates in a few portal tracts (Fig. 1A, 1B). The inflammatory cells comprised lymphocytes, plasma cells and eosinophils. The infiltration was mainly centered around the portal veins with endothelial damage. The hepatic arteries and bile ducts were spared by the inflammatory infiltrates and degeneration of bile duct epithelial cells was not identified. Mild ductular reaction was seen in at the portal-parenchymal interface. The portal fibrosis was mild, and there was no evidence of an 'onion-skin' pattern. The lobular inflammatory infiltrate was mild. Immunohistochemical stain revealed a few portal tracts containing up to 12 IgG4-positive plasma cells per high-power microscopic field (Fig. 1C).
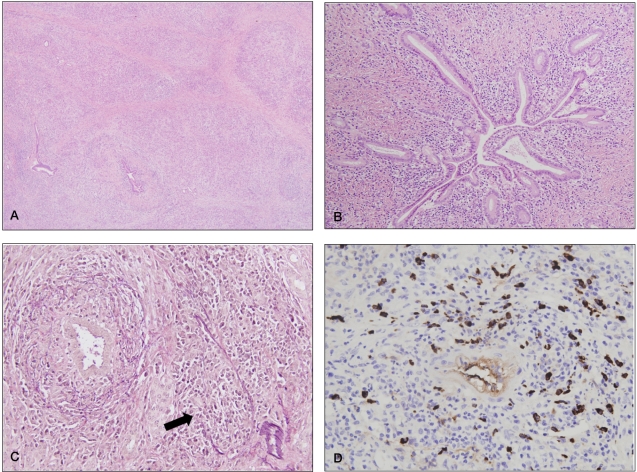
The previously resected pancreas demonstrated a dense lymphoplasmacytic infiltrate affecting the parenchyma with septal fibrous bands (Fig. 2A). The ductal epithelium was relatively intact despite the periductal dense inflammatory cell infiltrate (Fig. 2B). Obliterative phlebitis was frequently noted in the pancreatic parenchyma (Fig. 2C). Immunohistochemistry demonstrated abundant IgG4-positive plasma cells with an average of 43 IgG4-positive plasma cells per high power field (Fig. 2D).
DISCUSSION
The discrimination between IgG4-SC and pancreaticobiliary malignancies and PSC is an important issue. IgG4-SC responds well to steroid therapy or biliary drainage, while PSC is progressive and resistant to steroid therapy, resulting in the involvement of both the intra-and extrahepatic ducts and culminating in biliary cirrhosis.2 Clinically, PSC usually occurs in younger patients and presents with obstructive jaundice more commonly than IgG4-SC. PSC is commonly associated with inflammatory bowel disease, whereas IgG4-SC is associated with autoimmune pancreatitis.3 The measurement of serum IgG4 levels is useful for differentiating between these two disorders; according to previous studies, increased serum IgG4 levels exceeding 135 mg/dL are frequently seen in these patients.4
Hepatic involvement of IgG4-SC can manifest as an overt mass-like lesion or as a mild to moderate portal lymphoplasmacytic infiltration.5 Tumefactive lesions characterized by diffuse lymphoplasmacytic infiltration and prominent eosinophilic infiltration have been classified as the "lymphoplasmacytic type" of inflammatory pseudotumors by Zen et al,6 and these lesions have been proposed to belong to the spectrum of IgG4-related diseases. In addition to the lymphoplasmacytic and eosinophilic inflammatory infiltrates, obliterative phlebitis and cholangitis with periductal fibrosis have been found to be common features.
The liver pathology of IgG4-SC is different from that of PSC in the following aspects. IgG4-SC usually leaves the epithelial cells of the bile ducts intact, despite the remarkable periluminal inflammatory cell infiltration, while PSC is characterized by degenerative bile duct lesions and ductopenia.7 The portal inflammatory infiltrate of IgG4-SC consists of a dominant proportion of lymphocytes and plasma cells and also numerous eosinophils, whereas PSC shows a lesser degree of portal inflammation and neutrophilic infiltration.5 The periductal "onion-skin" fibrosis formed by well-organized lamellated collagen bands seen in PSC is absent in IgG4-SC,3 and obliterative phlebitis is more commonly identified in IgG4-SC.5,8 Lobular inflammation composed of lymphocytes and scattered plasma cells and eosinophils is a common finding in IgG4-SC, while it is significantly less frequently seen in PSC.7 Finally, it is important to demonstrate by immunohistochemistry the increased number of IgG4-positive plasma cells in the tissue in order to differentiate between the two diseases.
There is currently no established scoring criteria for IgG4 immunostaining in the biliary tract; however, most reports have demonstrated that the number of IgG4-positive plasma cells in extrahepatic bile ducts affected by IgG4-SC usually exceeds 30 per high-power field.5 As for the peripheral bile ducts of small portal tracts, marked heterogeneity in the degree of IgG4-positive plasma cell infiltration has been noted: for example, several portal tracts may lack the IgG4-positive cells entirely.7 Nevertheless, although there are discrepancies regarding the amount of IgG4-positive plasma cell infiltrates seen in small portal tracts obtained by needle biopsies, immunohistochemistry for IgG4 is an important part of the diagnosis of IgG4-SC, as IgG4-positive plasma cells are absent or rare in PSC.5,7
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




