

INTRODUCTION
Hepatocellular carcinoma (HCC), one of the most common malignant tumors worldwide,1 is usually treated by surgical resection, particularly in patients with American Joint Committee on Cancer (AJCC)-TNM stages I or II and reserved liver function.2 Because postoperative recurrence is the main obstacle to the success of this aggressive treatment, 3,4 various pathological features of surgical specimens have been established as predictors of risk of recurrence. They include tumor size and number, microvascular invasion, portal vein tumor thrombosis, the presence of satellite nodules, differentiation grade of the tumor cells, and the encapsulation state.4-6 Tumor size (usually greater than 5 cm), multiplicity, a cut margin narrower than 1 cm, and tumor stage (including vascular invasion) are independent factors associated with early (within 2 years) recurrence after surgical resection.3,4 The preoperative hepatic functional reserve and microscopic vascular invasion can enhance early recurrence of small HCCs.7 Early multinodular recurrence after surgical resection is not unusual in HCCs with multiple tumor nodules and portal vein thrombi.3 Furthermore, late recurrence (>2 years after resection) is significantly associated with Ishak hepatic inflammatory activity >6; indocyanine green (ICG) retention rate at 15 min (ICG-15) >10%; and hepatitis B virus (HBV) DNA level >106 copies/mL.4 Alpha-fetoprotein (AFP) and Lens culinaris agglutinin-reactive AFP (AFP-L3) are serological biomarkers of HCC with a more malignant nature.6
Multiple intrahepatic or extrahepatic metastases are associated with poor prognosis after recurrence.8 Reportedly, the proportions of intra- and extrahepatic recurrences of HCC following surgery are 80% and 20%, respectively.9 In brief, the organs involved in extrahepatic recurrence are lung (10.4-12.6%), adrenal glands (11%), peritoneum (6%), pancreas (3%), bone (1.5%), and brain (1.5%).9-11
Given the increasing chances of earlier diagnosis by an HCC screening program for high-risk individuals selected from patients with chronic liver diseases, it is critical to identify the characteristic patterns of molecules that are associated with HCC recurrence and the preferred organ sites of relapse after surgical treatment. Candidate molecules associated with prognosis or risk of recurrence include osteopontin9 and stathmin12 in relation with intrahepatic recurrence of HCCs, the acquisition of p53 mutation (p53Mut) as a poor prognostic molecular marker,13 and loss of E-cadherin with causal relationship to the invasiveness of HCC.14
In our previous study, we have suggested that an orchestration of multiple molecules engage in the regulation of malignant cancer cell behaviors such as invasion and proliferation.15 Further, we arbitrarily defined the co-expression patterns of Notch1, Snail, and p53 (NSP) proteins based on immunoblot analysis of clinical samples and matched them with experimentally observed malignant behavior.15 We proved that the expression status of the wild type of p53 (p53WT)/p53Mut interactively regulated Notch1 expression, and simultaneous upregulation of p53WT together with Notch1 and Snail expressions represented the invasive nature of HCCs.15 In this study, we verified the clinical utility of the NSP pattern as postoperative prognostic molecular markers for HCC. Because most of the p53 mutations occurred in grade III HCCs, data analyses were restricted to grade III HCCs to compare the effects of NSP patterns on the prognosis of HCC patients with p53WT and p53Mut.
MATERIALS AND METHODS
Inclusion of patients with immunoblot data for Notch1, Snail, and p53 and data for p53 mutations in HCCs
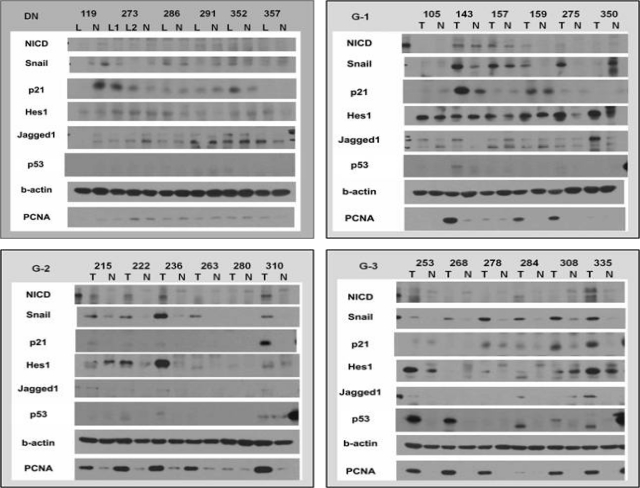
For this study, we obtained 162 immunoblots for the expression of Notch1, Snail, and p53 proteins and 110 sequences for p53 mutations in HCCs. All experiments were performed as described in the previous study.15 Briefly, rabbit monoclonal anti-Notch1 (diluted 1:100, Cell Signaling, Danvers, MA), rabbit polyclonal anti-Snail (diluted 1:100, Abcam, Cambridge, MA), and mouse monoclonal anti-p53 (diluted 1:100, Santa Cruz Biotechnology) antibodies were used to detect each protein in paraffin sections, and automated sequencing was performed to detect p53 mutations in frozen tissues (Appendix Fig. 1). Of the 162 immunoblots obtained, 147 were from patients with HCC (33 grade I, 40 grade II, and 74 grade III); their corresponding non-HCCs and 15 dysplastic nodules (DN) were used as controls. All tissue specimens, along with clinicopathological information, were obtained from Severance Hospital, Yonsei University College of Medicine (Seoul, Korea). The analyses focused on the effects of differentiation grade III HCC on postoperative prognosis, for which 47 cases were chosen on the basis of well-defined clinical records (mean age, 53±13 years; range, 28-76 years; 38 men and 9 women). Together with biochemical liver function, HBV viral markers, and serum AFP and protein induced by vitamin K absence (PIVKA) tests, all patients underwent a liver spiral computed tomography (CT) scan every 3-6 months to detect recurrent HCC after surgery. All patients had HBV infection and reserved liver function (Child-Pugh A). The reason for this selection criterion was that the differentiation grade4,5 and poor liver function7 themselves influenced the postoperative prognosis, and etiological factors could influence molecular expression patterns.16,17 For the evaluation, we kept a routine histological examination data file on differentiation grades, tumor size, tumor capsule formation (encapsulation), capsular infiltration, microvascular invasion, portal vein invasion, and satellite nodules. Differentiation was graded according to Edmondson and Steiner's criteria.18 Informed consent was obtained from each patient, and tissue collection was approved by the Institutional Review Board.
Statistical analysis
Statistical analysis was performed using R statistics software (Ver.2.12.2.; The R Foundation for Statistical Computing, Vienna, Austria), which is a free software used under the terms of the Free Software Foundation's GNU General Public License in source code form.19 The relationship between the expression of several proteins and the HCC grade was analyzed by calculating Spearman's correlation and by Fisher's exact test for count. Logistic regression analysis and a chi-square test were done to analyze the significance of the relationships among the expression patterns of the molecules. P-values of less than 0.05 were considered statistically significant.
RESULTS
Association of grade III HCC with pathological features indicating the risk of postoperative recurrence
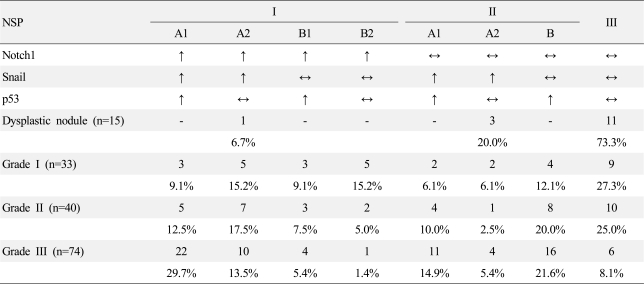
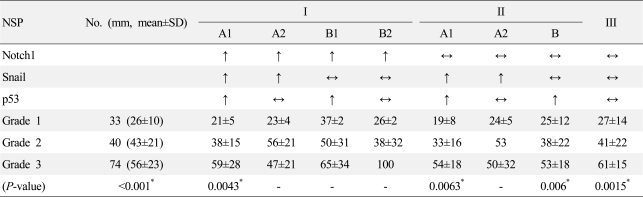
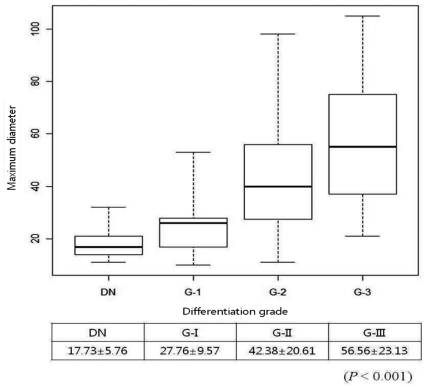
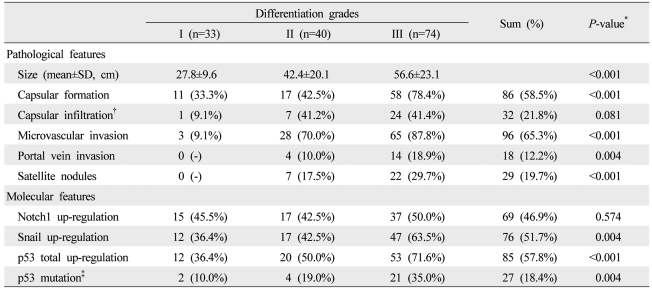
Because HCCs are classified on the basis of cellular morphology, differentiation grades do not directly depict the malignant nature of HCC. Therefore, in comparison with grades I and II HCCs, we characterized grade III HCC in view of their relationship with other pathological features that directly indicated postoperative prognosis, such as tumor size, encapsulation status, capsular infiltration, microvascular invasion, portal vein thrombosis, and satellite nodules. As summarized in Table 1 and Figure 1, the correlation between differentiation grades and other pathological features suggests that grade III HCC was more malignant than grade I and/or II HCCs.
Characteristic changes of both individual and co-expression statuses of Notch1, Snail, and p53 proteins in grade III HCC
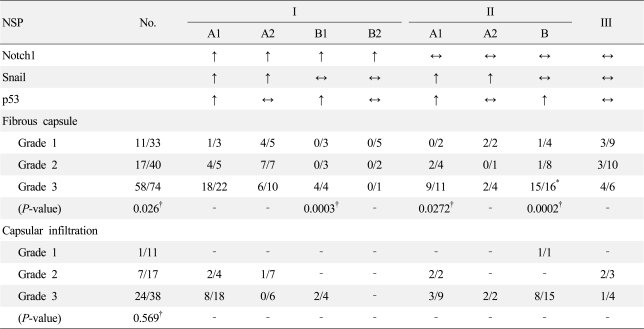
Of the 3 core molecules Notch1, Snail, and p53 proteins, which are components of the NSP pattern, the expression of Snail and p53 proteins were more significantly upregulated in grade III HCC than in grade I or II HCCs (P<0.01 and P<0.001, respectively), whereas Notch1 expression was not (P>0.1) (Table 1). Of the 8 NSP patterns, the proportional rates of NSP-IA1 (Notch1↑/Snail↑/p53↑), NSP-IIA1 (Notch1↔/Snail↑/p53↑), and NSP-IIB (Notch1↔/Snail↔/p53↑) patterns increased according to the differentiation grade; the NSP-IA2 (Notch1↑/Snail↑/p53↔) pattern was stationary; and the NSP-III pattern decreased (Appendix Table 1). This observation strongly suggests that the co-expression of these 3 core molecules may be regulated differently according to the differentiation grade of HCC.
Association of the p53 mutation rate with NSP patterns according to differentiation grades
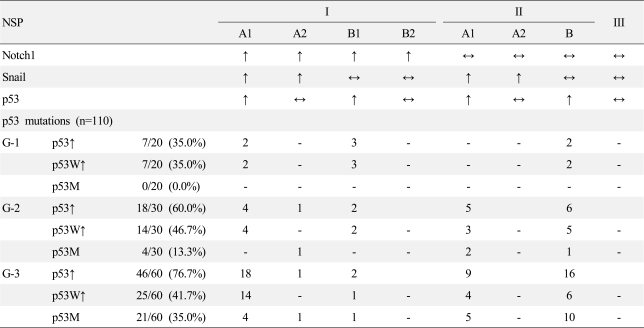
In our previous study, we demonstrated that both the expression level and the mutation of p53 protein were key factors regulating the nature of co-expression of the 3 core molecules selected for this study.15 Although there was a positive correlation between differentiation grade and the total incidence of p53 upregulation by immunoblot analysis, the incidence of upregulation of wild-type p53 was not altered in the various differentiation grades, whereas the majority of p53 mutations occurred in grade III HCC (Table 1 and Appendix Table 2).
In this study cohort with grade III HCC, the p53 upregulation rate was 36.3% (16/47), but the majority of the p53 mutations (75%, 12/16) were found in the NSP-II category. The distribution of p53 mutation rates differed significantly according to the NSP pattern: 71.4% (5/7) occurred in NSP-IIA1 and 63.6% (7/11) in NSP-IIB, whereas 20% (3/15) occurred in NSP-IA1 (P<0.001) (Table 2). The p53 mutation rate was different between the NSP-I and NSP-II categories.
Association of pathological features with NSP patterns according to differentiation grades
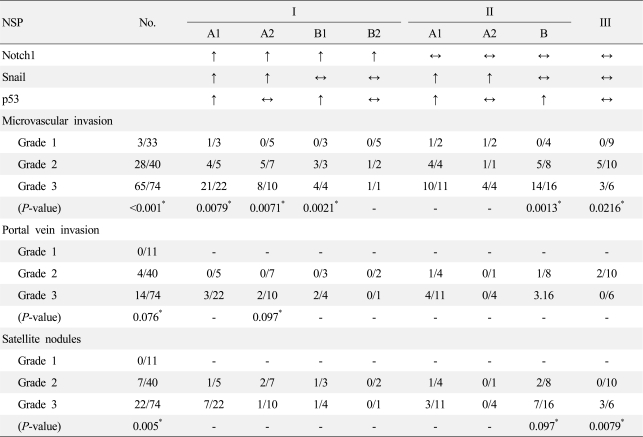
Of the pathological features associated with differentiation grades, tumor size, microvascular invasion, portal vein invasion, and satellite nodules did not differ according to the NSP pattern (Appendix Table 3 and 4). Interestingly, the NSP-IIB pattern (Notch1↔/Snail↔/p53↑) showed a drastic increase in the incidence of fibrous capsule formation in grade III HCC than in grade II HCC (93.8% (15/16) vs. 12.5% (1/8), respectively) (Appendix Table 5). Furthermore, both NSP-IA1 (Notch1↑/Snail↑/p53↑) and NSP-IIB patterns showed significant trends of capsular infiltration, compared to the NSP-IA2 (Notch1↑/Snail↑/p53↔) pattern with incidences of 50% (8/18), 53.3% (8/15), and 0% (0/6), respectively (P=0.002 and P=0.004, respectively) (Appendix Table 5).
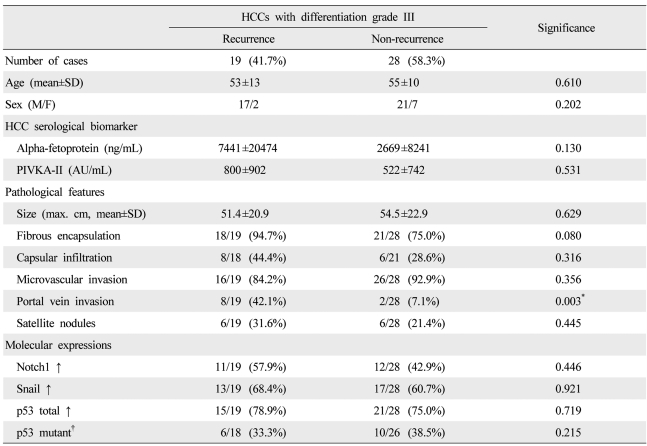
Characteristic pathological features related to postoperative recurrence of grade III HCC
On the basis of the data of pathological and molecular characterizations related to grade III HCC described above, we focused our analysis on how grade III HCC might affect postoperative recurrence. Of the 47 grade III HCC patients, 19 (41.7%) relapsed 8.6±5.9 months after surgical resection (range of DFI, 1-20.5 months). There were no significant differences in clinical variables, including age, sex, and preoperative serum AFP and PIVKA-II levels between the recurrent and non-recurrent groups (Table 3). In this cohort, only portal vein invasion was significantly correlated with recurrence (P=0.003): 42.1% (8/19) in the recurrence and 7.1% (2/28) in the non-recurrence groups (Table 3). These data suggest that, when limited to grade III HCC, portal vein invasion is the most important pathological feature for predicting the risk of postoperative recurrence.
Association of the NSP pattern with postoperative recurrence in grade III HCC
The individual expression status of Notch1, Snail, and p53 proteins was not associated with recurrence. Moreover, p53 mutation was not a significant prognostic factor for postoperative recurrence when the analysis was restricted to the grade III HCC group (Table 3). In addition, the recurrence rates of the NSP-IA1 (Notch1↑/Snail↑/p53↑) with p53 wild dominant and NSP-IIB (Notch1↔/Snail↔/p53↑) with p53 mutant dominant were 53.3% (8/15) and 18.2% (2/11), respectively (P=0.1092) (Table 2).
In HCCs with the NSP-I pattern, the mean tumor size was not significantly different between the recurrence and non-recurrence groups (smaller than 5 cm in both groups). However, in HCCs with the NSP-IIA1 and NSP-IIB patterns, the mean tumor size was significantly larger in the recurrence group than in the non-recurrence group (Table 2). Other pathological prognostic features were not significantly different between the recurrence and non-recurrence groups according to the NSP patterns.
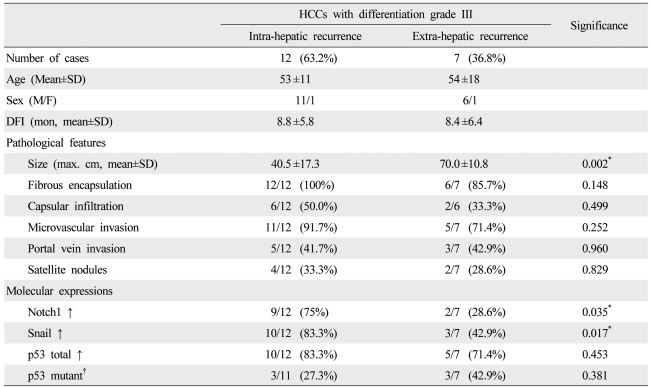
Characteristic pathological features associated with the relapse sites of grade III HCC
Twelve of 19 cases (63.2%) recurred within the liver and 7 (36.8%) recurred at extrahepatic sites, including 6 lung and 1 mediastinal lymph node metastases (Appendix Table 1). Two of 6 cases of pulmonary recurrence were accompanied by metastasis in other sites: 1 in the brain and 1 in an abdominal lymph node. There were no significant differences between the intrahepatic and extrahepatic recurrence groups in clinical parameters, including age, sex, and DFI (Table 4).
Among the pathological prognostic features, only tumor size was significantly associated with relapse sites (P=0.002): 40.5±17.3 cm in cases with intrahepatic recurrence and 70.0±10.8 cm in cases with extrahepatic recurrence (Table 4). The presence of microvascular tumor emboli, portal vein invasion, non-capsulation, or satellite nodules were not significant (Table 4). These data suggest that, of all clinicopathological parameters, only tumor size is important as an indicator for extrahepatic recurrence of grade III HCC and that the maximum cut-off size would be a diameter of 5 cm.
Association of the NSP pattern with postoperative relapse sites in grade III HCC
While the Notch1 and Snail proteins were not associated with the recurrence itself, the upregulation of Notch1 and Snail proteins were individually associated with the relapse sites (P=0.035 and P=0.017, respectively) (Table 4). In NSP pattern analysis, intrahepatic recurrence tended to be clustered in the NSP-IA1 pattern, while scattered in the non-NSP-IA1 patterns, although there was no statistical significance between both (87.5% [7/8] vs. 45.5% 5/11), respectively, P=0.1473). Extrahepatic recurrence rate of the NSP-IA1 and non-NSP-IA1 patterns was 12.5% (1/8) and 54.5% (6/11), respectively (P=0.1473) (Table 2). There was no deviation of the NSP patterns in cases with extrahepatic recurrence.
Although the NSP-IA1 pattern and tumor size showed potential as significant markers for indicating postoperative recurrence in grade III HCC, the Kaplan-Meier curve analysis showed no significant difference in the recurrence time based on NSP patterns (NSP-IA1 vs. non-IA1) and tumor size (cut-off diameter, 5 cm), as well as the relapse sites.
DISCUSSION
In this study, we focused primarily on the analyses of grade III HCC to clarify the association between NSP patterns and pathological malignant features indicating postoperative prognosis, including tumor size, fibrous encapsulation, capsular infiltration, microvascular invasion, portal vein invasion, and satellite nodules. The rationale for restricting the cases to the differentiation grade III is based on the observation that the majority of p53 mutations develop in grade III HCCs. Our data suggest that, even though the p53 is not mutated, the co-expression of three core molecules (Notch1↑/Snail↑/p53↑) in grade III HCC might be associated with postoperative recurrence risk, particularly in patients with HCC smaller than 5 cm in diameter, most of which fall within the best criteria for surgical treatment on the basis of AJCC-TNM staging.
Although p53 mutation was noticed as a prognostic marker of HCC,13 our data suggested that, when the analyses was limited to grade III HCC, the p53 mutation is not the sole molecular marker for indicating the postoperative recurrence risk. Instead, it was suggested that HCC cases with the co-expression of Notch1, Snail and p53 (with wild dominant, NSP-IA1 pattern) is a preferred cluster for intrahepatic relapse.
In accordance with conventional knowledge, our study also revealed that pathological prognostic features including tumor size, fibrous capsule formation, capsular infiltration, microvascular invasion, portal invasion, and satellite nodules, were well-correlated with differentiation grades of HCCs. These findings explain why grade III HCC is more malignant than grade I or II HCC, but do not address the following 2 concerns: the presence of any molecular type more prone to postoperative recurrence, and the nature of organ preference when relapse occurs.
When we focused on grade III HCC, our results revealed that only portal vein invasion was a significant pathologically independent prognostic factor for postoperative recurrence, whereas tumor size, encapsulation, capsular infiltration, microvascular invasion, and satellite nodules were not. However, the utility of portal vein invasion is limited because it occurs in only 18.9% of cases treated by surgical resection. Although microvascular invasion is an important predictor of postoperative recurrence, it was not a significant discriminating factor in grade III HCC because its rate of occurrence was 87.8%. Therefore, our results suggest that conventional pathological malignant features for predicting the postoperative recurrence risk are not useful in cases of grade III HCC.
Fibrous capsule formation surrounding an HCC nodule has been reported as a good prognostic marker for surgical treatment,5 and capsular infiltration by cancer cells as a poor prognostic marker for intrahepatic recurrence following surgical resection.5 Our study revealed that the prevalence of encapsulated tumors was positively correlated to the differentiation grade, and when compared to that of NSP-IA2 (Notch1↑/Snail↑/p53↔), capsular infiltration was significantly associated with the NSP-IA1 (Notch1↑/Snail↑/p53↑) pattern. Therefore, in combination with activation of the Notch1-Snail signal axis, p53 upregulation may contribute to the acquisition of an invasive nature as suggested in our previous study.15
Therefore, with respect to grade III HCCs, it can be concluded that together with tumor size, only portal vein invasion is significant as a pathological prognostic factor to indicate postoperative recurrence, whereas microvascular invasion and satellite nodules are not. Likewise, p53 mutation is not a significant molecular marker for indicating postoperative recurrence in grade III HCCs. The most significant marker for predicting extrahepatic recurrence is the tumor size larger than 5 cm in maximum diameter. Although the data is insufficient, our preliminary study focusing on the inter-relationships between pathological prognostic features and NSP patterns in grade III HCC may provide new insights into the role of molecular pattern analyses for predicting postoperative recurrence risk.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




