Transient elastography versus hepatic venous pressure gradient for diagnosing portal hypertension: a systematic review and meta-analysis
Article information
Abstract
Background/Aims
Transient elastography (TE) has been proposed as a promising noninvasive alternative to hepatic venous pressure gradient (HVPG) for detecting portal hypertension (PH). However, previous studies have yielded conflicting results. We gathered evidence from literature on the clinical usefulness of TE versus HVPG for assessing PH.
Methods
We conducted a systematic review by searching databases for relevant literature evaluating the clinical usefulness of non-invasive TE for assessing PH in patients with cirrhosis. A literature search in Ovid Medline, EMBASE and the Cochrane Library was performed for all studies published prior to December 30, 2015.
Results
Eight studies (1,356 patients) met our inclusion criteria. For the detection of PH (HVPG ≥6 mmHg), the summary sensitivity and specificity were 0.88 (95% confidence interval [CI] 0.86-0.90) and 0.74 (95% CI 0.67-0.81), respectively. Regarding clinically significant PH (HVPG ≥10 mmHg), the summary sensitivity and specificity were 0.85 (95% CI 0.63-0.97) and 0.71 (95% CI 0.50-0.93), respectively. The overall correlation estimate of TE and HVPG was large (0.75, 95% CI: 0.65; 0.82, P<0.0001).
Conclusions
TE showed high accuracy and correlation for detecting the severity of PH. Therefore, TE shows promise as a reliable and non-invasive procedure for the evaluation of PH that should be integrated into clinical practice.
INTRODUCTION
Portal hypertension (PH) is a major consequence of chronic liver disease that can lead to serious complications, such as variceal bleeding and ascites [1,2]. PH is responsible for significant morbidity and mortality, particularly in patients with decompensated cirrhosis [1-4]. In this regard, the diagnosis and precise discrimination of PH severity allow prediction of prognosis and essential for managing chronic liver disease (CLD) appropriately. Measurement of the hepatic venous pressure gradient (HVPG) has been accepted as the gold standard for assessing the degree of PH. Clinically significant PH (CSPH) defined as HVPG ≥10 mmHg, has been associated with formation of esophageal varices and poor prognosis [5-7]. However, the routine use of this method in clinical setting has been limited by its invasiveness and the need for expertise and specialized equipment.
Therefore, an alternative, non-invasive technique allowing clinicians to diagnose and grade PH in patients with cirrhosis and that could replace HVPG is needed. Transient elastography (TE) has been established as a non-invasive method of measuring liver stiffness due to its diagnostic accuracy in hepatic fibrosis [7]. Accumulating evidence suggests that TE adequately reflects the findings of HVPG, indicating that it is a useful modality for evaluating PH and cirrhotic complications [8-14]. However, some studies have reported conflicting results indicating TE is not sufficiently accurate to replace HVPG due to its insufficient sensitivity or specificity [15]. Hence, controversy remains regarding the usefulness of TE for assessing PH. Systematic reviews (SRs) and meta-analyses (MAs) have facilitated objective evaluation of existing evidence [16-20]. Shi et al. [21] reported the results of their MA for TE in the diagnosis of PH and esophageal varices and further studies should be performed to confirm their conclusion.
Thus, the present SR and MA identified the clinical usefulness of non-invasive TE for assessing PH as an alternative to HVPG in patients with CLD.
MATERIALS AND METHODS
Literature search
We performed a literature search to identify published study articles that examined TE for the diagnosis of PH in patients with CLD. We searched Ovid Medline, the Cochrane Library and EMBASE for the studies published prior to December 30, 2015, using the following search terms: elastography, liver stiffness, portal hypertension, chronic liver disease and diagnostic test. Then, a manual search of the reference lists of the primary studies was performed to locate any other studies. The present study was performed according to the PRISMA Statement [22].
Study inclusion/exclusion
The inclusion criteria for primary studies were as follows: (1) studies that evaluated the accuracy of liver stiffness performed using TE for the prediction of PH in patients with CLD; (2) studies that measured portal pressure using the HVPG; PH defined as ≥6 mmHg, CSPH ≥10 mmHg and severe PH ≥12 mmHg; (3) studies that reported the data necessary to calculate the true positive, false positive, true negative and false negative diagnostic results of TE for the diagnosis of PH, significant PH and severe PH based on cut-off values. If such data were unavailable, the corresponding author was contacted.
Quality assessment of the primary studies
The quality of the studies included in the MA was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) questionnaire, which was designed to assess the internal and external validity of the diagnostic accuracy of studies in this analysis. This tool is a 14-item instrument that allows the identification of important design elements in diagnostic accuracy studies, such as the patient spectrum, the presence or absence of observer blinding and verification bias, the handling of indeterminate results and the reporting of patients lost to follow-up. Each study that met the inclusion criteria was analyzed by two independent reviewers. Discrepancies in the results were handled by a consensus review. If the QUADAS score was less than 10 points, the study was classified as having low methodological quality.
Data extraction
Two reviewers independently extracted required information from the primary studies based on a fixed protocol. In each study, the following information was obtained: author; study publication year; country; study design; number of patients; patient age and sex; CLD etiology; prevalence of PH and significant PH; TE cut-off for PH; number of true positives, false positives, true negatives, and false negatives; sensitivity; specificity; positive predictive value; negative predictive value; area under the receiver operating characteristic curve (AUROC); and correlation coefficient estimate.
Data analysis/synthesis
The integrated results of each study were presented to show their combined effect, measured as summary sensitivity values, specificity values, likelihood ratios and summary correlations with 95% confidence interval (CI) used to examine the TE accuracy for PH. The effect size regarding the correlation coefficient between TE and HVPG was calculated with transformation using Fisher’s Z. Correlation forest and radial plots were also constructed to determine the diagnostic accuracy of the test parameters.
The heterogeneity of all diagnostic test parameters was initially evaluated with a graphic examination of forest plots for each parameter. Then, a statistical assessment was performed with the inconsistency index (I2). The I2 statistic was defined as the percentage of variability due to heterogeneity beyond that from chance; values >50% represented the possibility of substantial heterogeneity.
Finally, publication bias analysis and sensitivity analysis were conducted to verify the validity of the results. The analyses were performed using Review Manager (RevMan) version 5.3 (The Cochrane Collaboration, London, UK), comprehensive meta-analysis software version 3.0 (Biostat, Inc., Englewood, NJ, USA) and R statistical software (The R Foundation, Vienna, Austria).
RESULTS
Characteristics of studies in our analysis
Based on the described search strategies, 163 studies were retrieved. After eliminating the duplicates (n=86) or studies that were unrelated to the topic (n=35), 42 potentially relevant studies were identified for further evaluation. Ultimately, 34 studies were excluded for undesirable article type (n=17), not written in English (n=1), failing to evaluate TE accuracy (n=7), irrelevant to CLD (n=7), or containing insufficient data (n=2). Thus, eight studies fulfilled the inclusion criteria. The flow chart of the study selection is shown in Figure 1.
Flow diagram of study selection for the systematic review and meta-analysis.
The main study characteristics included in this analysis are summarized in Table 1; 1,356 patients (mean age: 55.1 years, 69.2% male) were included. The overall prevalence of PH, significant PH and severe PH were 59.4% (range: 46.0-72.9%), 58.3% (range: 21.7-80.4%), and 58.9% (range: 57.4-60.5%), respectively.
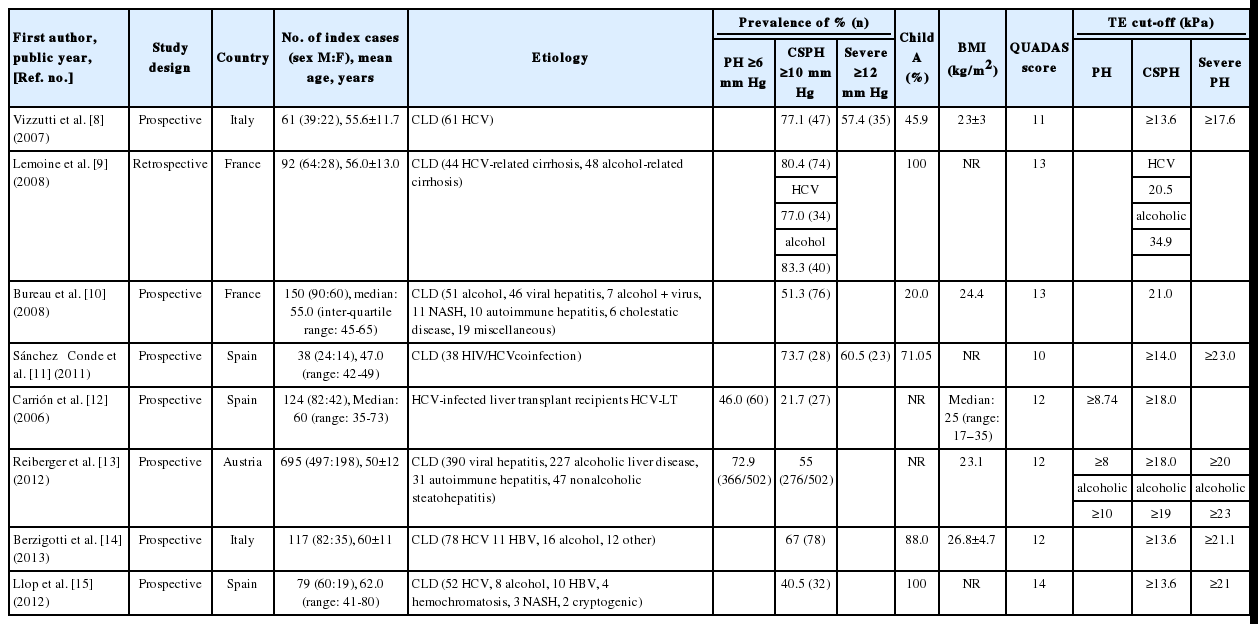
The main characteristics of studies evaluating the performance of TE for detection of portal hypertension, clinically significant portal hypertension, and severe portal hypertension
Based on the QUADAS scale, the included studies had very good methodological quality (Table 1).
Accuracy of TE for the detection of PH/CSPH/severe PH
Two [12,13] studies evaluated the diagnostic accuracy of TE for PH (Table 2). The cut-off value of liver stiffness ranged from 8-8.74 kPa. The sensitivity and specificity were 0.88 (range: 0.86-0.90) and 0.74 (range: 0.67-0.81), respectively. The positive predictive value (PPV) and negative predictive value (NPV) were 0.83 (range: 0.81-0.84) and 0.88 (range: 0.85-0.90), respectively. The AUROC for the diagnosis of PH (HVPG ≥6 mmHg) was 0.86 (range: 0.79-0.92). One study reported a significant correlation between TE and HVPG for the diagnosis of PH (r=0.84, P<0.001).
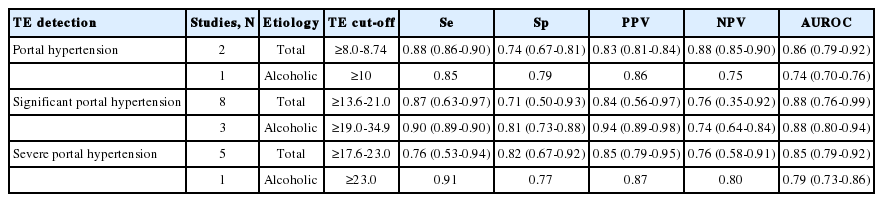
Summary accuracy of TE detection of PH, clinically significant PH, and severe PH
A forest plot of the eight studies showed pooled correlation between HVPG and TE (Figs. 2 and 3). Five studies demonstrated a relationship between TE and HVPG for the diagnosis of CSPH [9-11,14,15] and a significant correlation was observed with an effect size of correlation (COR) 0.7480 (95% CI, 0.6464; 0.8236, P<0.0001) according to the random effects model (Figs. 2 and 3). The I2 statistic value was 84.7%, indicative of substantial heterogeneity caused by the inconsistent characteristics of the included studies, including patient characteristics, cirrhosis etiologies, and varying diagnostic thresholds.
Pooled correlation between transient elastography and hepatic venous pressure gradient. COR, correlation; CI, confidence interval; W, weight.
Radial Plot for Correlation between transient elastography and hepatic venous pressure gradient.
Eight studies [8-15] evaluated the diagnostic accuracy of TE for CSPH (Table 2). The cut-off value of liver stiffness ranged from 13.6-21.0 kPa (alcoholic 19-34.9 kPa). The sensitivity and specificity were 0.85 (range: 0.63-0.97) and 0.71 (range: 0.50-0.93), respectively. The PPV and NPV were 0.84 (range: 0.56-0.97) and 0.76 (range: 0.35-0.92), respectively. The AUROC for the diagnosis of CSPH (HVPG ≥10 mmHg) was 0.88 (range: 0.76-0.99).
Five studies [8,11,13-15] evaluated the diagnostic accuracy of TE for severe PH (Table 2). The cut-off value of liver stiffness varied from 17.6-23.0 kPa (alcoholic 23.0 kPa). The sensitivity and specificity were 0.76 (range: 0.53-0.94) and 0.82 (range: 0.67-0.92), respectively. The PPV and NPV were 0.85 (range: 0.79-0.95) and 0.76 (range: 0.58-0.91), respectively. The AUROC for the diagnosis of CSPH (HVPG ≥12 mmHg) was 0.85 (range: 0.79-0.92).
Assessment of publication bias and sensitivity analysis
We used a funnel plot to examine publication bias. The results of the MA showed a symmetrical shape for pooled correlation in 5 studies. The adjusted pooled correlation calculated using the trim-and-fill method was 0.80 (95% CI, 0.71; 0.86, P<0.0001), which was slightly higher than the observed effect size of 0.75 (95% CI, 0.65; 0.82, P<0.0001), but it had no major impact on this study (Fig. 4).
Trim and fill funnel plot on the pooled correlation.
We performed sensitivity analysis to assess the extent to which our results were sensitive to the analysis restricted only to those studies. No significant difference was found for the pooled results of any of the assessed outcomes.
DISCUSSION
The objective of this SR and MA was to identify the clinical usefulness of non-invasive TE for assessing PH in patients with CLD. There has been considerable interest in developing and validating non-invasive methods to detect PH among patients with cirrhosis [5-15,17]. Accordingly, this review can help researchers compare and select the most appropriate non-invasive evaluations for PH in patients with CLD.
To the best of our knowledge, this is the first SR and MA to focus on the utility of measuring TE for diagnosing PH by thorough comparison with HVPG in CLD. Although a Chinese group presented the MA results of TE for diagnosing PH and the presence of esophageal varices, only five published studies have evaluated the performance of TE for significant PH in a small number of patients, limiting the robustness of any conclusion reached [21]. In addition, considerable variability existed across different investigations as well as small sizes of individual studies. However, more accumulating data are now available, allowing a more precise analysis of TE versus HVPG for diagnosing PH.
TE has the advantage of being non-invasive and many attempts have been made to assess the degree of hepatic fibrosis using TE. Recently, several lines of evidence have indicated that TE can be useful for assessing the severity of PH [8-15].
This systematic review identified eight studies that evaluated the diagnostic performance of TE with PH in patients with cirrhosis and fulfilled the inclusion criteria and reported sufficient data.
The diagnostic accuracy of TE for CSPH was high in the present SR and MA (COR 0.7480, 95% CI, 0.6464; 0.8236, P<0.0001). Furthermore, the sensitivity and specificity were 0.85 (range: 0.63-0.97) and 0.71 (range: 0.50-0.93), respectively; the AUROC was 0.88 (range: 0.76-0.99).
However, Llop et al. [15] demonstrated a moderate correlation between TE and HVPG (r=0.552) compared to other studies (r=0.68-0.86). Furthermore, patients with a TE value between 13.6 and 21 kPa had insufficient sensitivity and specificity to detect CSPH (HVPG >10 mmHg). The reason for this varying performance of TE might be that only less severe forms of CLD, such as Child-Pugh A with hepatoma, were included, since this is the target population for identifying CSPH in patients with potentially resectable hepatomas. Most of the studies on patients without hepatoma showed a higher correlation between TE and HVPG than the studies evaluated in this study. Accordingly, the presence of hepatoma and the Child A population in this study were attributed to different results obtained using TE.
Since PH is initiated by an increase in intrahepatic resistance, TE appropriately reflects mild to moderate PH or the initiation of CSPH. However, in cases of severe PH, its severity becomes more dependent on the amount of portal blood inflow and peripheral hemodynamic changes than the stiffness of the hepatic parenchyma; thus, the predictive power of TE for PH is limited [8]. This explanation was supported since TE could not accurately predict the hemodynamic response to a non-selective ß blocker.
The currently favored method for determining portal venous pressure involves catheterization of the hepatic vein and measurement of HVPG, which provides independent prognostic information on survival and the risk of decompensation. CSPH is also necessary for esophageal varix formation, bleeding and initial decompensation [5-7].
Although HVPG is the most accurate test for diagnosing PH, a readily available, non-invasive method is preferable for the assessment of PH because most of the patients with CLD require long-term follow-up. This study demonstrated that due to the correlation between TE and HVPG, TE can potentially reduce the number of HVPG procedures performed in order to examine the severity of PH [8-15].
The present study had the following potential limitations. First, only eight studies were used to evaluate the usefulness and performance of TE, thus limiting the robustness of the conclusions reached. Second, the characteristics of the included studies, including patient characteristics, cirrhosis etiologies and varying diagnostic thresholds, were not completely consistent. Third, we only included studies written in English, thus language bias might have influenced the results.
In conclusion, the TE results were similar to those obtained using HVPG. Additionally, TE is a simple and safe method due to its non-invasiveness. Although further investigation is needed, TE could be a reliable, non-invasive supplementary tool for diagnosing the severity of PH.
Notes
Author’s contributions
GK and SKB designed the analysis. MYK and SKB formulated the model. GEK and SKB analyzed the data. GK and SKB wrote the manuscript. All authors reviewed and approved the manuscript.
Conflicts of Interest: The authors have no conflicts to disclose.
Acknowledgements
This study was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (HI15C2364) and by the Yonsei University Future-Leading Research Initiative of 2014.
Abbreviations
AUROC
area under the receiver operating characteristic curve
CI
confidence interval
CLD
chronic liver disease
COR
correlation
CSPH
clinically significant PH
HVPG
hepatic venous pressure gradient
MA
metaanalysis
NPV
negative predictive value
PH
portal hypertension
PPV
positive predictive value
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
QUADAS
Quality Assessment of Diagnostic Accuracy Studies
SR
systematic review
TE
transient elastography