


INTRODUCTION
There has been controversy regarding the most effective firstline treatment modality for the patients who have small solitary hepatocellular carcinoma (HCC) (tumor size of 2–5 cm); radiofrequency ablation (RFA) or percutaneous ethanol injection (PEI), surgical hepatic resection (HR) and liver transplantation (LT). For choosing treatment modality of HCC, it should be considered according to the underlying liver parenchymal disease with function as well as the tumor stage. If the liver function is good enough, HR may be the first choice for the solitary HCC regardless of the tumor size. However, recent studies comparing RFA with resection showed comparable outcome and similar survival rates. LT offers an excellent long term outcome, addressing both the underlying liver disease as well as tumor stage. Herein, we reviewed the role of HR, RFA and LT for small sized HCC and would suggest updated new strategy to get the best short- and long-term outcome (Table 1, 2) [1-10].
TREATMENT MODALITY
Radiofrequency ablation
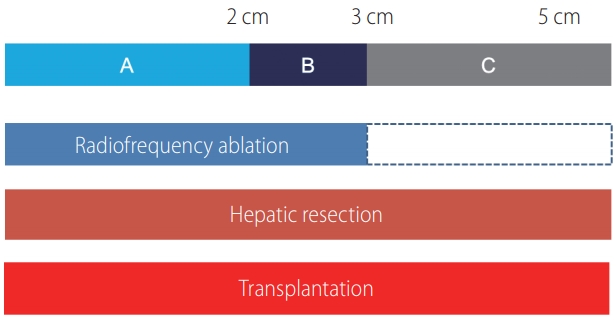
RFA has been applied for the patients who have poor liver function with limited tumor size up to 5 cm and has shown similar outcome in terms of overall and disease-free survival (DFS) in comparison to HR [1]. Treatment modality does not affect DFS for the patients with the tumor size smaller than 2 cm, but the underlying parenchymal status is more important effect on long term survival. RFA is preferred if there is no survival benefit with HR because percutaneous RFA provide better post-treatment health related quality of life than HR [2]. In a cohort study based on a Japanese nationwide survey, of 28,510 patients with HCC tumors no more than 3 tumors (≤3 cm) treated by PEI, RFA and HR, HR results in longer overall survival and better time to recurrence than either RFA or PEI [3]. And in another large population based study using the Surveillance, Epidemiology and End Results database a total of 1,894 patients with HCC less than 5 cm, it can be treated with RFA for the tumors size less than 3 cm, survival outcome treated with RFA is worse than HR, no difference in overall survival but significant difference in DFS. Of note, for the patients with tumors measuring over 3 cm, even small increases in tumor size (<0.5 cm) were found to result in significantly shorter survival for patients treated with RFA compared with those treated with HR [4]. Although RFA can be successful as first line treatment with size cutoff of 2 cm, 3 cm and 5 cm, the maximum tumor size for which RFA is safe and effective remains highly controversial. A 3 cm cutoff value has been recommended by the American Hepato-Pancreato-Biliary Association and in the Barcelona Clinic Liver Cancer staging system algorithm (Fig. 1) [11]. There are concerns that RFA is ineffective for lesions measuring over 3 cm [2,4,5,12], although some reports have shown that lesions measuring up to 5 cm can be ablated safely [13-15]. Although RFA is ineffective in larger than 3 cm tumor or unfavorable location, combined PEI may improve reducing recurrence in others [16,17].
Microvascular invasion (MVI) is known as significant factor for disease recurrence and survival after HR [18,19]. Therefore, HR may be preferred to RFA in patients with MVI. However, presence of MVI cannot be estimated preoperatively. Recent studies showed larger tumor (>3.5 cm or >5 cm) and high AFP (>200 ng/mL or 400 ng/mL) are significant predictable factor for presence of MVI [19,20]. Therefore, tumor marker should be considered for treatment decision of small HCC as well as tumor size. In summary, RFA would be desired in patients who have small tumor (less than 3.0 cm) and low AFP (<200 ng/mL).
Hepatic resection
Regarding HR, the complication rate including surgical mortality rate is higher than RFA. However, it has been persistently decreased, down to less than 1% mortality, even close to zero mortality in high volume liver surgery centers [21,22]. Furthermore, minimal invasive laparoscopic HR was dramatically established for last 10 years. For another issue of HR, benefit of anatomical resection in comparison to non-anatomical resection has been controversy for long time. According to the three papers based on a case control study with propensity score matching have shown no survival benefit [23-25]. If it is true, hepatic surgeon may not insist to do anatomical resection better obtainable by open surgery. In apart, according to the improvement of advanced laparoscopic technique, laparoscopic anatomical resection has been well established particularly for resection more than sectionectomy, even for segmentectomy [26-28]. Through gradual introduction of laparoscopic anatomical HR, the perioperative and oncological outcomes are comparable to those with open anatomical resection by experienced laparoscopic surgeon [29]. For the tumors located on the surface of the liver, even though the tumor size is less than 3 cm, local recurrence rate is high with RFA. However it is privileged indication for laparoscopic resection with enough tumor free margin [30].
In a very well-designed meta-analysis using a total of 16,103 patients to evaluate the therapeutic effects of RFA and surgical HR in the treatment of small HCC mostly ≤5 cm, thirty-one studies were included in the analysis, they achieved very good conclusion in this debatable issue. Compared to the RFA group, the 3-, 5-year overall and DFS rates in the HR group were significantly higher. In subgroup analyses, the overall and DFS in the HR group significantly higher than in the RFA group for HCCs ≤3 cm, whereas there was no significant difference between two groups for HCCs ≤2 cm. For patients with HCCs of 2 cm or less, RFA is an alternative to HR because of their comparable long term efficacy remaining less procedure related complications [12]. However, in small HCCs with high tumor marker, HR should be considered because it has high recurrence risk after RFA.
Liver transplantation
LT can provide better survival outcome than RFA or HR. LT has been established and propagated as a good option showing better long-term survival benefit for the patients whose liver function is not optimal for resection, if the tumor status is within Milan criteria including solitary 2–5 cm HCC. As mentioned previously, a well-designed case control study with propensity score matching has shown no survival benefit in anatomical resection, laparoscopic resection is feasible in terms of surgical and oncologic outcomes. Furthermore it is much better for the patients in salvage liver LT later on, because it results in less adhesion and derangement of liver anatomy. A propensity score-matched case-control comparative study of laparoscopic and open resection for the HCC has shown similar short-term and long-term outcomes [31,32]. Salvage living donor liver LT is significantly better survival than repeatetive HR, particularly for the Child B liver cirrhosis [33]. In compensated cirrhotics with early HCC, survival rate is better with primary LT compared with HR group. And salvage LT was comparable with primary LT in terms of short and long-term outcomes. Therefore, better patients selection for the ‘resection first’ approach and early detection of recurrence can achieve better outcomes of the salvage LT strategy [34]. Another benefit of resection first strategy is enlistment of LT for patients before recurrence at high risk of HCC recurrence after resection on the basis of pathologic aggressiveness, MVI and/or satellites nodules [35]. In consideration of salvage LT, laparoscopic resection first strategy is a very good option, because salvage LT after laparoscopic resection is comparable to primary LT in terms of operative time, oncologic radicality, morbidity and mortality [36]. On the contrary, patients with poor liver function or low level of tumor markers, RFA can be considered instead of HR in consideration of salvage LT.
CONCLUSION
RFA, HR and LT provide good outcome for patients who have small HCCs. RFA would be desired in patients who have small tumor (less than 3.0 cm) and low AFP (<200 ng/mL). However, in small HCC with high tumor marker, HR should be considered. Better patients’ selection for the ‘resection first’ approach and early detection of recurrence can achieve better outcomes of the salvage LT strategy. Another benefit of resection first strategy is enlistment of LT for patients before recurrence at high risk of HCC recurrence after resection on the basis of pathologic aggressiveness, MVI and/or satellites nodule. They should be applied appropriately according to the tumor size, location, tumor markers and underlying liver parenchymal disease. Each procedure itself of RFA, HR or LT or combination is a kind of art, and selection process of the treatment modality for individual patients to apply is another kind of art, to obtain the best short-term and long-term outcome.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print





