


INTRODUCTION
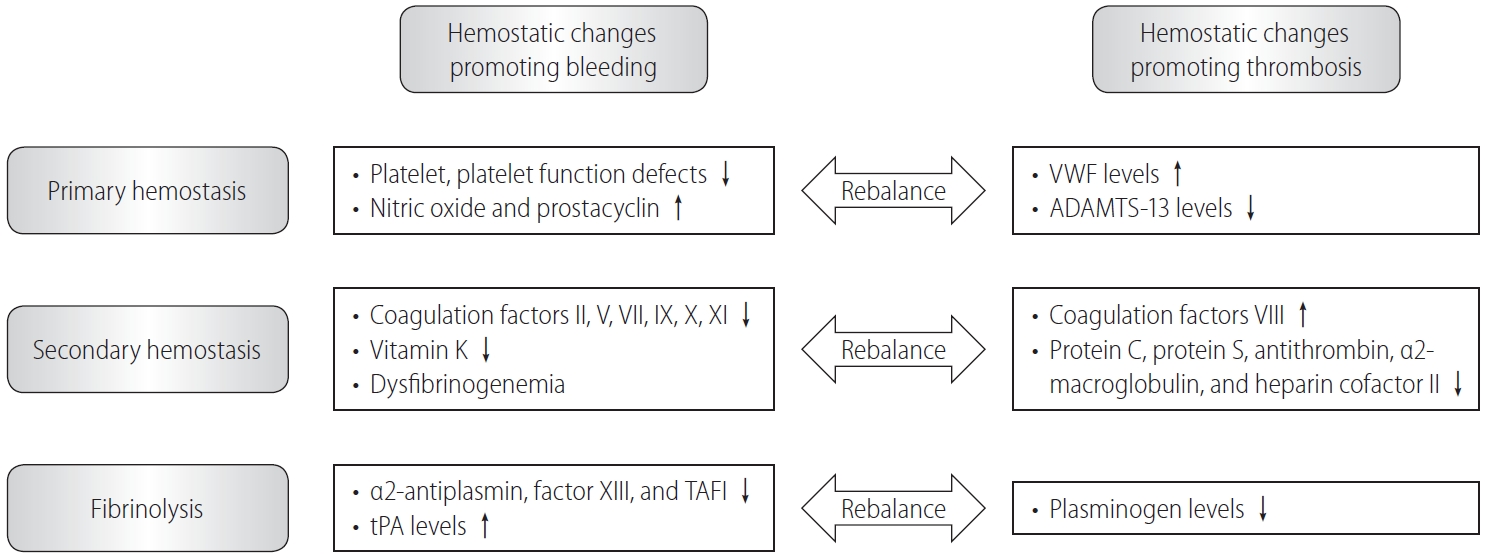
Liver cirrhosis is associated with a high risk of bleeding secondary to coagulopathy, and is characterized by prolonged bleeding time, thrombocytopenia, increased prothrombin time (PT), and a hypofibrinolytic state [1]. A simultaneous decrease in protein C and S levels, endothelial activation, and reduced antithrombin synthesis contribute to a prothrombotic state in these patients [2]. Reportedly, the von Willebrand factor level (an antihemostasis driver for low platelet counts observed in patients with cirrhosis) was significantly elevated in relation to the platelet-vascular wall interaction [3]. Concomitant alterations in pro- and antihemostatic processes lead to rebalanced hemostasis, although routine laboratory tests for hemostasis that focus on platelet count estimation or the international normalized ratio (INR) for PT suggest a hypocoagulable state (Fig. 1). A meta-analysis of 29 studies (n=13,276 patients with cirrhosis) reported that INR did not serve as a significant correlate for periprocedural bleeding; no significant association was observed between periprocedural bleeding and pre-procedural INR [4].
However, this hemostatic rebalance in patients with cirrhosis is not a fixed phenomenon compared with healthy individuals, and is affected by factors such as infection, renal failure, and surgery. Previous studies have reported new-onset major bleeding in 17ŌĆō20% of patients with cirrhosis admitted to the intensive care unit [5,6]. A recent meta-analysis of 27 studies (n=93,191) reported that the incidence of intracranial hemorrhage was 2.0% in patients with cirrhosis, who showed a significantly increased risk of subarachnoid hemorrhage (hazard ratio [HR], 2.36; 95% confidence interval [CI], 1.80ŌĆō3.09; P<0.001) and intracranial hemorrhage (HR, 1.48; 95% CI, 1.06ŌĆō2.05; P<0.05) [7]. In contrast, the incidence of venous thromboembolism (VTE), including deep vein thrombosis or pulmonary embolism, was 0.5ŌĆō6.3% in hospitalized patients with cirrhosis [8,9]. A recent study showed that hemostatic balance may fluctuate between a hypo- and hypercoagulable state in cases of decompensated cirrhosis with acute kidney injury (AKI) [10]. Among 80 patients with decompensated cirrhosis (40 patients each with and without AKI), those with cirrhosis and AKI had lower platelet aggregation and secretion (indicative of impaired platelet function) and lower protein C, protein S, and antithrombin levels together with increased thrombin formation, which indicate hypercoagulability [10]. Platelet function and coagulopathy improved in patients with decompensated cirrhosis after AKI resolution [10].
Patients with cirrhosis have shown varying hypo- or hypercoagulability tendencies; a recent study using a thromboelastography test (RoTEM®, which is a more accurate indicator of coagulation status than PT or platelet counts in patients with cirrhosis) showed that patients with cirrhosis were more likely to be predisposed to a hypocoagulable (bleeding risk) than a hypercoagulable state (thrombosis risk). Thromboelastography is a point-of-care viscoelastic test of hemostasis in whole blood for accurate measurement of real-time global clot formation and dissolution [11].
Despite a predominant bleeding tendency, portal vein thrombosis (PVT) is more common in patients with cirrhosis owing to PV flow impairment and vascular endothelial cell injury [12]. Serag et al. [13] reported that portal flow velocity was significantly lower in patients with cirrhosis who developed PVT compared to those without PVT (14.2┬▒2.3 cm/s vs. 17.8┬▒2.6 cm/s, P<0.001). These changes concomitant with endothelial injury contribute to PVT in patients with cirrhosis [12]. Studies have shown that PVT is significantly associated with progressive hepatic decompensation and a high mortality risk in patients with cirrhosis [14].
Several direct-acting oral anticoagulants (DOACs) developed in recent years are useful to overcome the limitations of previously popular anticoagulants, such as vitamin K antagonists (VKAs) and heparin [15]. The oral direct thrombin inhibitor, dabigatran etexilate (Pradaxa®), and oral direct activated factor Xa inhibitors, such as rivaroxaban (Xarelto®), apixaban (Eliquis®), and edoxaban (Lixiana®), are currently licensed for use in patients with indications for anticoagulation, including VTE prophylaxis, as well as for the treatment and prevention of stroke and systemic embolic events in cases of non-valvular atrial fibrillation [15]. Although betrixaban (Bevyxxa®) has also been recently licensed for VTE prevention, few reports have established the efficacy and safety of betrixaban in patients with cirrhosis [16]. We investigated the efficacy and safety, as well as the potential role of DOACs (dabigatran etexilate, rivaroxaban, apixaban, and edoxaban) in patients with cirrhosis with a focus on their role in PVT.
DEFINITION OF PVT
No standardized definition is available for PVT owing to its heterogeneous etiology, manifestations, natural history, and therapeutic options. Although the terminology and classification systems for PVT vary extensively in the literature, PVT is usually defined as thrombosis of the PV and/or its right or left branches with extension of the thrombus into the mesenteric or splenic veins, associated with complete or partial occlusion. PVT may also be classified into acute or chronic types. The European Association for the Study of the Liver (EASL) guidelines published in 2016 do not define the exact periods that correspond to acute and chronic PVT, but define acute PVT as PVT in patients ŌĆ£without malignancy and cirrhosisŌĆØ and ŌĆ£cirrhotic PVT.ŌĆØ Acute PVT is defined as ŌĆ£recentŌĆØ thrombosis of the PV and/or its right or left branches [17].
According to the American Association for the Study of Liver Diseases (AASLD) guidelines published in 2020, acute PVT is defined as ŌĆ£the sudden formation of a thrombus within the portal vein.ŌĆØ The thrombus can variably involve portions of the mesenteric and/or splenic vein [18,19]. The term ŌĆ£recent (present for <6 months)ŌĆØ is preferred over ŌĆ£acute,ŌĆØ as the latter implies both clinical symptoms and recent-onset thrombosis, considering that patients with acute PVT do not always develop clinical symptoms. According to the AASLD guidelines (2020), chronic PVT (duration Ōēź6 months) [19], also referred to as portal cavernoma, is attributable to replacement of the obstructed PV by a network of hepatopetal collateral veins that bypass the thrombosed vein segment [18]. Portoportal collaterals or periportal varices, which develop over 1ŌĆō3 months, represent a typical manifestation of chronic PVT [20] which is associated with an increased risk of portal cholangiopathy, acute decompensation, and mortality [21].
With regard to the treatment of ŌĆ£recent PVT,ŌĆØ the AASLD guideline recommends initial medical anticoagulation and local or systemic thrombolytics in selected patients in whom intestinal ischemia persists despite anticoagulation [19]. Observation alone with serial 3-month imaging without therapy is considered in patients with cirrhosis who show ŌĆ£recentŌĆØ thrombosis of small intrahepatic sub-branches of the PV or minimally occlusive main PV thrombosis (<50% luminal obstruction). However, anticoagulation should be considered to prevent progressive thrombosis and portal hypertension in patients with cirrhosis who have ŌĆ£recentŌĆØ occlusive or partially occlusive thrombosis of the main PV (>50% luminal obstruction) or mesenteric veins [19]. With regard to treatment of ŌĆ£chronic PVT,ŌĆØ the AASLD guideline indicates no confirmed benefit of anticoagulant or interventional therapy in patients with chronic complete occlusion of the main PV or cavernous transformation of the PV with established collaterals, and recommends that treatment should focus on the management of portal hypertension-induced complications [19]. PV recanalization (PVR) followed by transjugular intrahepatic portosystemic shunt (TIPS) should be considered in liver transplantation candidates with chronic PVT to create a physiological anastomosis between the graft and recipient PV. PVR followed by TIPS should also be considered in patients with chronic PVT and recurrent bleeding and/or ascites refractory to medical therapy. The AASLD guidelines do not explicitly define the treatment period between recent and chronic PVT; this period depends on clinical situations for the treatment of acute or chronic PVT [21,19].
The EASL guidelines recommend at least 6-month maintenance anticoagulation therapy for cirrhotic PVT, which should be initiated after ensuring adequate prophylaxis for gastrointestinal (GI) bleeding. The EASL guidelines do not provide detailed recommendations for acute PVT in patients with cirrhosis. Furthermore, TIPS was indicated in most cases for portal hypertension-induced complications, such as recurrent bleeding and/or refractory ascites, and not for PVT; therefore, the applicability of TIPS for PVT treatment is not discussed by the EASL guidelines.
The classification of PVT differs between the two aforementioned guidelines; therefore, treatment duration for PVT and the type of anticoagulation therapy (with or without DOACs) also differ between these guidelines. The AASLD guidelines highlight the role of medical anticoagulation to treat acute PVT in patients with cirrhosis, although medical anticoagulation is not clearly indicated in patients with chronic partial occlusion. The EASL guidelines emphasize the role of medical anticoagulation for cirrhotic PVT. Table 1 summarizes the EASL and AASLD clinical guidelines for the definition and management of PVT in patients with cirrhosis [17,19].
PATHOPHYSIOLOGY OF PVT
The pathophysiology of PVT in cirrhosis is multifactorial and results mainly from alterations in the different components of VirchowŌĆÖs triad: reduced portal blood flow, a hypercoagulable state, or vascular endothelial injury (Fig. 2) [22]. Recent studies have reported that cirrhosis patients with portal blood flow less than 15 cm/s were at increased risk of developing PVT [23,24]. In addition, an increase in portal blood inflow through portosystemic collaterals also seems to influence PVT development [25,26].
Second, hypercoagulability can contribute to pathologic thrombus formation in the PV in cirrhosis patients. Previous studies suggested that the low protein C levels directly impact thrombosis in patients with cirrhosis [27], and an increased ratio between factor VIII and protein C in cirrhosis appears to be responsible for the intrinsic resistance to the anti-coagulant activity of thrombomodulin, a key endothelial receptor in the inhibitory process of thrombin generation in the macro- and micro-circulation [3,28].
Lastly, vascular endothelial damage can lead to thrombosis with the exposure of tissue factor, subsequent stimulation of thrombin production, and promotion of platelet aggregation [29], and the presence of endotoxin increases tissue factor expression on the endothelial surface while simultaneously decreasing thrombomodulin expression [30].
GRADES OF PVT
PVT is historically classified into the following types: cirrhotic or noncirrhotic, acute or chronic, occlusive or non-occlusive, and malignant or nonmalignant [31,32]. However, the most widely used classification, which is of prognostic value in patients awaiting liver transplantation, is that proposed by Yerdel et al. [33] as follows: grade I, <50% luminal thrombosis of the main PV with or without minimal extension into the superior mesenteric vein (SMV); grade II, >50% luminal thrombosis of the PV, including complete thrombosis, with or without minimal extension into the SMV; grade III, complete PVT thrombosis with thrombus extension into the proximal SMV with patent distal SMV; and grade IV, complete PVT and SMV thrombosis (Table 2).
EPIDEMIOLOGY OF PVT IN PATIENTS WITH CIRRHOSIS
The relative risk of PVT is 7-fold higher in patients with cirrhosis than in the general population, which is estimated to be<1.0% [34]. The prevalence of PVT in patients with cirrhosis is 1ŌĆō26%, with an annual incidence of 3ŌĆō17%, depending on the severity of cirrhosis (PVT prevalence increases with cirrhosis progression) [35]. A recent national multicenter study including 753 patients with cirrhosis reported that the incidence rate of PVT was 6.1 per 100 patient-years [36]. A prospective cohort study that included a majority of patients with compensated cirrhosis (Child-Pugh class A) reported a 1-year cumulative incidence of PVT of 3.7ŌĆō4.6% [37,38]. Other cohort studies that included a majority of patients with decompensated cirrhosis (Child-Pugh B or C) reported a 1-year cumulative incidence of PVT of 16.4ŌĆō17.9% [23,39]. A recent large-scale multicenter retrospective study in China which investigated 2,826 patients with cirrhosis reported that the prevalence of PVT in patients with cirrhosis and acute decompensation was 9.36%, which was significantly higher than the 5.2% observed in those with cirrhosis without acute decompensation (P=0.04) [40].
CURRENT GUIDELINES FOR THE TREATMENT FOR PVT IN PATIENTS WITH CIRRHOSIS
Conventional treatments using low-molecular-weight heparin (LMWH) and VKAs
The AASLD guidelines recommend medical anticoagulation to treat recent PVT in patients with cirrhosis and recent occlusive or partially occlusive main PV thrombosis (>50% luminal obstruction) [19]. Additionally, local or systemic thrombolytic therapy can be considered in selected patients with recent PVT in whom intestinal ischemia persists despite medical anticoagulation [19].
The EASL guidelines recommend at least 6-month administration of anticoagulants, such as LMWH or VKAs, at therapeutic doses for chronic PVT [17]. The AASLD guidelines recommend TIPS concomitant with medical anticoagulation in patients with recurrent bleeding and/or refractory ascites. DOAC therapy is suggested for treatment ŌĆ£in partŌĆØ as a recommendation based on small cohort studies [19]. Both guidelines suggest sustained anticoagulation in patients with PVT awaiting liver transplantation until completion of the procedure [17,19]. TIPS or PVR followed by TIPS should be considered in patients with progressive PVT unresponsive to anticoagulation, who await liver transplantation [17,19].
Mechanism underlying the action of LMWH, VKAs, and direct anticoagulants
LMWH inhibits the final common pathway of the coagulation cascade, which is the conversion of fibrinogen into fibrin by the activity of thrombin, and blocks the coagulation pathway by activating antithrombin III that binds to and inhibits factor Xa [41]. VKAs block the function of the vitamin K epoxide reductase complex in the liver, leading to depletion of the reduced form of vitamin K that serves as a cofactor for gamma carboxylation of vitamin K-dependent coagulation factors [42]. Without gamma carboxylation, the vitamin K-dependent factors, such as factors II, VII, IX, and X, cannot function, as they cannot adequately bind calcium and phospholipid membranes needed for their hemostatic function [43]. The mechanisms of the DOAC (dabigatran, rivaroxaban, apixaban, and edoxaban) are as follows. Dabigatran is a reversible, potent, competitive direct thrombin inhibitor [44]. Unlike heparin, which can only bind free thrombin, dabigatran is capable of binding and inhibiting both free and clot-bound thrombin [45]. Rivaroxaban, apixaban, and edoxaban inhibit both free and clot-bound factor Xa, as well as prothrombinase activity, and do not require cofactors (such as antithrombin) to exert their anticoagulant effect [46]. Unlike indirect factor Xa inhibitors, they inhibit both free and clot-bound factor Xa, as well as prothrombinase activity. By inhibiting factor Xa, the three DOACs decrease thrombin generation and thrombus development.
Efficacy and safety of low-molecular-weight heparin and vitamin K antagonist treatments
LMWH is the preferred agent, typically followed by VKAs in patients with acute PVT [47]. LMWH offers the advantage of a fixeddose regimen without the need for laboratory monitoring. However, daily subcutaneous LMWH administration may reduce patient compliance and require dose adjustment based on renal function, which is relatively poor in patients with advanced liver cirrhosis [47]. VKAs are usually considered for long-term anticoagulation; however, maintaining the INR within the therapeutic range throughout treatment and interference with the model for end-stage liver disease (MELD) score are challenging in patients administered VKAs [47].
Two recent meta-analyses reported that conventional anticoagulants significantly increased the PVT recanalization rate of 71% (odds ratio [OR], 4.16; 95% CI, 1.88ŌĆō9.20) as compared to 42% in patients without anticoagulants, and lowered the PVT progression rate of 9% (OR, 0.06; 95% CI, 0.02ŌĆō0.20) as compared to 33% in patients without anticoagulants [48,49]. Both LMWH and warfarin effectively prevented thrombosis progression; however, LMWH, but not warfarin, was significantly associated with complete PVT resolution [48]. Cessation of anticoagulation after PV repermeation led to recurrent thrombosis in up to 38% of patients after a few months [50]. A recent meta-analysis of 33 studies (n=1,696 patients with cirrhotic PVT who received conventional anticoagulants) reported that decompensated cirrhosis may be associated with lower PVR rates in patients who are administered anticoagulants [51]. Early anticoagulation initiation (risk ratio [RR], 1.58; 95% CI, 1.21ŌĆō2.07; P<0.001) significantly increased PVR. Furthermore, decompensated cirrhosis (RR, 0.77; 95% CI, 0.62ŌĆō0.95; P=0.02) and higher MELD scores (mean difference, -1.48; 95% CI, -2.20 to 0.76; P<0.001) were significantly associated with low PVR rates [51].
Bleeding, one of the most common complications of anticoagulation therapy, occurred in 5% of patients with cirrhosis and PVT who received anticoagulants [50]. A meta-analysis of six studies that included 257 patients with cirrhosis and PVT reported no difference in total bleeding rates between the anticoagulation and noanticoagulation groups (11% in both groups) [48]. Moreover, the research showed PVT progression rates of 9% and 33%, respectively, in patients with and without anticoagulation therapy [48]. Non-portal hypertensive bleeding complications following therapeutic anticoagulation were similar between patients with cirrhosis and the general population [19]. Anticoagulants do not tend to affect portal hypertension-induced bleeding in patients with cirrhosis [19].
Role of TIPS for PVT treatment
Indications for TIPS in patients with cirrhosis and PVT include a poor response to anticoagulation or acute PVT accompanied by gastroesophageal variceal bleeding [52,53]. TIPS accelerates the PV inflow and improves PVT recanalization [54]. There are clinical benefits of TIPS for PVT treatment in patients with cirrhosis, such as the following: 1) it achieves effective endovascular recanalization of the thrombosed PV, 2) simultaneously resolves symptomatic portal hypertension, and 3) prevents thrombus recurrence or extension owing to portosystemic shunt creation [55]. Although TIPS is recognized as technically feasible in patients with PVT, it is challenging in patients with extensive obliteration of intrahepatic PV branches and fine collateral vessels [56]. Trans-splenic TIPS is feasible for PVR in patients with complete PVT occlusion, who await liver transplantation [47].
A recent meta-analysis of 13 studies that included 399 patients reported technical feasibility of TIPS in 95% of patients, and that this procedure effectively achieved sustained PVT recanalization. However, it showed a moderate risk of major complications, such as hemoperitoneum (10%) [57]. A randomized controlled trial performed by Lv et al. [58] included patients with cirrhosis (94%, ChildPugh class A or B) concomitant with PVT, with a history of variceal bleeding in the preceding 6 weeks. The patients were randomly assigned to the TIPS group (n=24) or the endoscopic band ligation (EBL) plus propranolol group (EBL+drug, n=25) [58]. During a median follow-up of 30 months in both groups, the incidence rate of variceal rebleeding was significantly lower in the TIPS than in the EBL+drug group (15% vs. 45% at 1 year and 25% vs. 50% at 2 years; HR, 0.28; P=0.008). Moreover, the incidence rate of PVR in the TIPS group was significantly higher than that in the EBL+drug group (95% vs. 70%, P=0.03), and the re-thrombosis rate in the TIPS group was relatively lower than that in the EBL+drug group (5% vs. 33%, P=0.06) [58], which indicate that TIPS can effectively maintain long-term PV patency and obviate the need for anticoagulation.
The effects of anticoagulation therapy after TIPS in patients with cirrhosis and PVT are controversial. A recent randomized controlled study showed that anticoagulation may not be necessary since TIPS placement alone can achieve long-term recanalization [59]. In contrast, Yue-Meng et al. [60] reported that warfarin could effectively promote recanalization in approximately 50% of patients within 1 year in those with de novo post-TIPS PVT. The incidence of PVT in the warfarin group (15%) was 3-fold lower than that in the control group (43%) [60].
DOAC treatment for PVT in patients with cirrhosis
Approval uses for DOACs in the general population
Currently, the following Food and Drug Administration (FDA)- approved DOACs are available clinically: dabigatran (a direct thrombin inhibitor), rivaroxaban, apixaban, edoxaban, and betrixaban (all factor Xa inhibitors) [61]. DOACs are approved for the following indications: prevention of thromboembolic events in atrial fibrillation, VTE prevention in patients who undergo hip or knee replacement, in patients hospitalized for acute illness, and for recurrent VTE or pulmonary embolism prophylaxis and prevention [62].
Studies have confirmed that compared with conventional anticoagulants, DOACs are safer in the general population [16]. A fixed-dose user-friendly regimen without the need to monitor the PT, with lesser food and drug interactions compared with other anticoagulants, are some of the advantages of DOACs [63]. However, studies that investigated the safety and efficacy of DOACs excluded patients with cirrhosis, a condition that is associated with an increased risk of PVT [16]. Table 3 summarizes the inclusion and exclusion criteria used for phase III trials for each DOAC (RE-LY, ROCKET-AF, ARISTOTLE, and ENGAGE-AF trials) [64-67]. Clinical trials that investigated dabigatran and edoxaban have excluded patients with active liver disease, including viral hepatitis A, B, and C, and patients who showed abnormalities on hepatic biochemical testing [64,67]. Similarly, a clinical trial that investigated rivaroxaban excluded patients with significant liver disease, such as acute clinical hepatitis, chronic active hepatitis, and cirrhosis, in whom alanine aminotransferase levels were >3-fold the upper limit of normal [65]. Patients with abnormalities on hepatic biochemical testing were also excluded in a clinical trial using apixaban[66]. Additionally, phase III trials for dabigatran, apixaban, and edoxaban excluded patients with platelet counts Ōēż100,000/mm3 [64,66,67]. Rivaroxaban trials did not define a strict platelet threshold; however, this trial excluded patients with ŌĆ£hepatic disease, which is associated with coagulopathy leading to a clinically relevant bleeding risk.ŌĆØ This might have led to the inclusion of individuals with undiagnosed cirrhosis and portal hypertension [65]. In some ambiguous ways, all four DOACs are contraindicated in severe liver disease. Few studies have reported DOAC therapy in patients with cirrhosis, and limited data are available in the literature. The exclusion criteria adopted by clinical trials may prevent the expansion of research with regard to DOAC use in patients with cirrhosis and could serve as obstacles, as medical insurance does not cover PVT treatment in patients with cirrhosis.
Efficacy of DOACs for PVT resolution in patients with cirrhosis
No standard criteria are available to evaluate the ŌĆ£efficacyŌĆØ of anticoagulants to treat PVT. Currently, the efficacy of DOACs in patients with cirrhosis and PVT has been evaluated only by means of various response states, such as recanalization rates (complete/partial resolution rates), PVT progression rates, or PVT recurrence (re-thrombosis) rates. Although response criteria of PVT in patients with cirrhosis were not standardized in each study, most previous studies have reported that DOAC efficacy was superior to that of conventional anticoagulants in patients with cirrhosis and PVT (Table 4) [68-75]. In a study that investigated DOAC efficacy in 36 patients with cirrhosis across 17 European centers [70], De Gottardi et al. [70] observed PVT in 61% of patients; these patients were treated with DOACs (rivaroxaban [83%], apixaban [11%], or dabigatran [5%]) with median follow-up of 15 months, and the post-DOAC PVT recurrence rates were low (4.5%) in patients who received these drugs [70]. Recently, a single-center study performed by Nagaoki et al. [71] compared the efficacy of edoxaban and warfarin as maintenance treatment in patients with cirrhosis concomitant with acute PVT. After 2-week intravenous danaparoid (a low molecular weight heparinoid devoid of heparin) administered at the time of diagnosis of acute PVT, all patients received edoxaban (n=20) or warfarin (n=30) for 6 months [71]. Comparison between the edoxaban vs. warfarin groups showed a significantly higher rate of complete PVT resolution (70% vs. 20%) and a lower rate of PVT progression (5% vs. 47%) in the edoxaban group [71]. In a recent randomized controlled trial that compared rivaroxaban with warfarin for the treatment of acute PVT in patients with hepatitis C-induced cirrhosis, who underwent splenectomy for symptomatic hypersplenism within 1 week prior to enrollment, Hanafy et al. [73] observed that PVR rates were higher in patients treated with rivaroxaban (85%) than in those treated with warfarin (45%). With regard to the efficacy of post-TIPS anticoagulation, a prospective observational study performed by Lv et al. [74] reported that compared to warfarin, post-TIPS enoxaparin or rivaroxaban administration was associated with a lower risk of re-thrombosis in patients with cirrhosis and PVT. During a median follow-up of 31.7 months, re-thrombosis rates were 2% in patients treated with TIPS+warfarin and 0% in those treated with TIPS+enoxaparin/rivaroxaban; these rates were 33.3% in those who received only warfarin and 0% in those who received only enoxaparin/rivaroxaban [74]. A prospective observational cohort study performed by Ai et al. [75] in patients with cirrhosis and PVT compared patients who received DOACs to those who did not receive anticoagulants. The post-DOAC complete/partial PVT recanalization rates were 12.8% in the DOAC group and 0% in the no-anticoagulant group at 3 months, and 28.2% in the DOAC group and 2.6% in the no-anticoagulant group at 6 months (P<0.05 for all) [75]. In this study, the baseline total bilirubin levels and Child-Pugh scores were improved, and the thromboelastography coagulation index was significantly improved in the DOAC group compared to the no-anticoagulant group (P<0.05) [75]. The efficacy of DOACs for PVT has mainly been investigated in patients with well-compensated cirrhosis; however, further studies are required to confirm whether DOACs show high efficacy against PVT even in patients with decompensated cirrhosis. There is a lack of conclusive evidence to prove that a specific type of DOAC is more effective for the treatment of PVT in patients with cirrhosis.
Safety of direct oral anticoagulants in patients with cirrhosis and PVT
Most previous studies have reported that DOACs had ŌĆ£at leastŌĆØ similar safety profiles as conventional anticoagulants in patients with cirrhosis; the rate of bleeding complications in patients who received DOACs was comparable to that observed in patients who received conventional anticoagulants (Table 4) [68-75]. Bleeding events were categorized as ŌĆ£total bleedingŌĆØ and ŌĆ£major bleeding.ŌĆØ The most frequent definition of major bleeding was fatal bleeding or overt bleeding that led to a reduction of at least 20 g/L in the serum hemoglobin level, or bleeding that necessitated transfusion of at least 2 units of packed blood cells, or hemorrhage at a critical anatomical site (e.g., intracranial or retroperitoneal bleeding) [76]. Intagliata et al. [68] compared the major bleeding rates between cirrhosis patients treated with DOACs (rivaroxaban [55%] or apixaban [45%]) and those treated with conventional anticoagulants (warfarin or LMWH), and observed no significant intergroup differences in the major bleeding rates (5% [1 of 20] in the DOAC group and 11% [2 of 19] in the conventional anticoagulation group, P=0.99). Hum et al. [69] reported that major bleeding rates observed during 3-year follow-up were higher in the conventional anticoagulation group (28%) than in the DOAC group (4%) for thrombosis or prevention of stroke in patients with atrial fibrillation and cirrhosis (P=0.03); however, the ŌĆ£total bleedingŌĆØ rates were similar in both groups. Nagaoki et al. [71] reported no significant difference in the prevalence of major GI bleeding between patients with cirrhosis and PVT treated with edoxaban (15%) and those treated with warfarin (7%) for 6 months (P=0.34).
Importantly, Hanafy et al. [73] reported no hepatic decompensation or mortality in patients with cirrhosis and concomitant PVT who received rivaroxaban (n=40), whereas those who received warfarin (n=40) showed higher incidence of hepatic decompensation manifested as ascites (41.0%), GI bleeding (43.3%), hepatic encephalopathy (31.8%), or death (20%).
Lv et al. [74] (n=396) recently reported that compared with warfarin, long-term anticoagulation using enoxaparin or rivaroxaban with or without TIPS did not increase the risk of major GI bleeding in patients with cirrhosis and PVT over a median follow-up of 31.7 months. The GI bleeding rates were 14.7% in the no-anticoagulation group (n=20/136), 14.2% in the warfarin group (n=31/218), and 14.2% in the enoxaparin/rivaroxaban group (n=6/42) (P=0.06) [74].
Upper GI bleeding was the most common cause of bleeding associated with DOAC therapy in patients with cirrhosis. Sasso et al. [77] recently reported that 18% of bleeding events, with upper GI bleeding (53%), occurred in patients with cirrhosis who received warfarin (n=183) or DOACs (n=133). Esophageal varices were significantly associated with a high risk of clinically relevant bleeding (OR, 5.7; 95% CI, 1.8ŌĆō17.7; P<0.05) [77], which highlights the importance of accurate and early diagnosis and treatment of esophageal varices based on the guidelines [78-80], prior to the initiation of anticoagulation therapy for cirrhotic PVT.
Notably, few studies have discussed the safety of DOACs and compared the complications based on DOACs for the treatment of PVT in patients with decompensated cirrhosis. However, Mort et al. [81] recently reported potential DOAC-induced bleeding risk in patients with decompensated cirrhosis. The authors observed that patients with decompensated cirrhosis had a significant risk of bleeding (25.8%, n=24 of 93), and 21% of the patients in this study discontinued DOAC therapy for 6 months [81]. Major bleeding predominantly occurred in patients with hepatocellular carcinoma (54%, n=7/13) who received DOACs for the treatment of atrial fibrillation and splanchnic or non-splanchnic venous thrombosis [81]. Further well-designed comparative studies are warranted to confirm the safety among DOACs and to investigate safety profiles in patients with decompensated cirrhosis concomitant with PVT.
Hepatic metabolism of individual direct oral anticoagulants
Table 5 summarizes the mechanism of action, metabolism, half-life, and reversal agent for individual DOACs. Dabigatran is a direct thrombin inhibitor, which is eliminated through the kidneys (80%) and the liver (20%) [82]. Its terminal half-life is 14ŌĆō17 hours in healthy individuals [83]. Dabigatran peak levels (Cmax) and exposure (area under the curve [AUC]) were slightly lower in patients with Child-Pugh class B than in healthy individuals [84]. The current guidelines do not include recommendations for dabigatran usage or dosing in patients with hepatic dysfunction. Idarucizumab is a humanized monoclonal antibody fragment approved by the FDA that has been developed as a specific reversal agent for dabigatran [85]. A phase 3 clinical trial, REVERSE-AD, showed that over 98% of 503 patients reached 100% reversal of dabigatran activity [85].
Rivaroxaban is a direct factor Xa inhibitor that undergoes renal elimination (unchanged drug) and metabolic degradation of the drug [82], and resulting metabolites are excreted via both renal and hepatobiliary routes. Its terminal half-life is 9ŌĆō13 hours in healthy individuals [83]. Peak drug levels (Cmax) and drug exposure (AUC) of a single rivaroxaban dose are slightly elevated in patients with Child-Pugh class A and moderately elevated in patients with Child-Pugh class B [86]. Rivaroxaban was shown to prolong the PT in patients with Child-Pugh classes A and B [16].
Apixaban is a direct factor Xa inhibitor that is eliminated through the kidneys (25%) and the liver (75%) [82]. Its terminal half-life is 8ŌĆō15 hours in healthy individuals [87]. Compared with healthy individuals, the peak drug levels of a single apixaban dose (5 mg) remained unchanged in patients with Child-Pugh classes A and B. Drug exposure (AUC) was slightly elevated in patients with cirrhosis. Apixaban does not require dose adjustment in patients with Child-Pugh class A [84].
Edoxaban is a direct factor Xa inhibitor that is eliminated through the kidneys (50%) and the liver (50%) [82]. Its terminal half-life is 9ŌĆō10 hours in healthy individuals [83]. Peak levels and drug exposure of a single edoxaban dose were elevated in patients with Child-Pugh classes A and B compared to healthy individuals [88].
Andexanet-╬▒ is a recombinant modified factor Xa protein approved by the FDA for the reversal of apixaban and rivaroxaban (not yet FDA-approved for edoxaban) [89]. A phase 3 clinical trial, ANNEXA, showed that 79% of 47 patients who received apixaban, rivaroxaban, edoxaban, or enoxaparin treatment achieved effective homeostasis [89].
No study has described the specific DOAC type that may be effective and safe for PVT treatment in patients with cirrhosis. Dabigatran may be considered relatively safe among the available DOACs in patients with cirrhosis, as it undergoes relatively lesser hepatic metabolism; however, few clinical studies have investigated the role of dabigatran for PVT treatment in patients with decompensated cirrhosis. The FDA [90] and European Medicines Agency (EMA) [91] recommend Child-Pugh score evaluation to guide DOAC treatment. According to the FDA and EMA guidelines, any DOAC is contraindicated in patients with Child-Pugh class C disease. Although apixaban, dabigatran, and edoxaban can be used with caution and/or after dose adjustment in patients with ChildPugh classes A and B, rivaroxaban administration is contraindicated in patients with Child-Pugh class B. Furthermore, DOACs should not be used in patients with Child-Pugh class C; and renal insufficiency, drug-drug interactions, a history of bleeding, and thrombocytopenia should be confirmed before the initiation of DOAC therapy.
CONCLUSIONS AND FUTURE DIRECTIONS
Patients with liver cirrhosis tend to show a more complicated coagulation state than is usually recognized based on standard coagulation tests. Rebalanced hemostasis involves the activity of both pro- and anticoagulant factors, and occurs secondary to various precipitating events. Worsening severity of cirrhosis predisposes patients to PVT and consequent portal hypertension-induced bleeding. This condition, particularly in patients with decompensated cirrhosis, often leads to a clinical dilemma, as it is difficult to determine whether to treat PVT in this clinical scenario in which two critical challenges oppose each other, specifically the high risk of bleeding vs. ongoing hepatic insufficiency caused by PV obstruction.
PVT, a common thrombotic complication observed in patients with cirrhosis, is invariably associated with poor outcomes and warrants at least 6-month maintenance anticoagulation therapy using LMWH or warfarin, according to the guidelines. Unfortunately, cessation of anticoagulation may be followed by recurrent thrombosis even after complete repermeation; therefore, an individualized long-term anticoagulation regimen is warranted.
The efficacy and safety of DOACs in patients with cirrhosis have been reported predominantly by small-sized, retrospective studies that only focused on patients with well-compensated cirrhosis; however, compared to conventional anticoagulants, DOACs appear to be ŌĆ£at leastŌĆØ safe and efficacious to treat PVT in patients with well-compensated cirrhosis and PVT. Notably, a few recent studies have reported that DOACs may cause significant bleeding and lower the recanalization rates in patients with decompensated cirrhosis and PVT [51,81]; therefore, DOACs should be cautiously administered to patients with decompensated cirrhosis. Therefore, it is important to decide whether prophylactic anticoagulation should be administered to patients with compensated cirrhosis at high risk for PVT or PVT progression, and to determine the optimal time to commence DOAC treatment to prevent PVT before the onset of decompensation.
There is a lack of convincing data regarding the benefits associated with the treatment of PVT, as PVR does not necessarily improve the course of chronic liver disease. Furthermore, it is necessary to conclusively establish the type of DOAC that shows the best efficacy and safety and to determine the optimal drug, dose, and treatment duration for management of PVT in patients with cirrhosis. Prospective studies with well-defined outcomes in a well-characterized cohort are warranted to gain a deeper understanding of these clinical issues.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print





