Imaging diagnosis of hepatocellular carcinoma: Future directions with special emphasis on hepatobiliary magnetic resonance imaging and contrast-enhanced ultrasound
Article information

Abstract
Hepatocellular carcinoma (HCC) is a unique cancer entity that can be noninvasively diagnosed using imaging modalities without pathologic confirmation. In 2018, several major guidelines for HCC were updated to include hepatobiliary contrast agent magnetic resonance imaging (HBA-MRI) and contrast-enhanced ultrasound (CEUS) as major imaging modalities for HCC diagnosis. HBA-MRI enables the achievement of high sensitivity in HCC detection using the hepatobiliary phase (HBP). CEUS is another imaging modality with real-time imaging capability, and it is reported to be useful as a second-line modality to increase sensitivity without losing specificity for HCC diagnosis. However, until now, there is an unsolved discrepancy among guidelines on whether to accept “HBP hypointensity” as a definite diagnostic criterion for HCC or include CEUS in the diagnostic algorithm for HCC diagnosis. Furthermore, there is variability in terminology and inconsistencies in the definition of imaging findings among guidelines; therefore, there is an unmet need for the development of a standardized lexicon. In this article, we review the performance and limitations of HBA-MRI and CEUS after guideline updates in 2018 and briefly introduce some future aspects of imaging-based HCC diagnosis.
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary liver cancer, which exacts a heavy disease burden and is the third most common cause of cancer-related death worldwide [1-3]. HCC mainly occurs in patients with chronic liver disease, with chronic hepatitis B and C virus infections being the most common causes [1]. One unique and important characteristic in the diagnosis of HCC is that it can be diagnosed noninvasively by imaging modalities without pathologic confirmation in high-risk patients, which renders it imperative to correctly diagnose HCC on imaging [4]. Thus, guidelines have been established in many societies such as the American Association for the Study of Liver Diseases (AASLD), Liver Imaging Reporting and Data System (LI-RADS), the European Association for the Study of the Liver (EASL), the Asian Pacific Association for the Study of the Liver (APASL), and the Korean Liver Cancer Association-National Cancer Center (KLCA-NCC) to standardize the acquisition, interpretation, and reporting of imaging studies for HCC diagnosis [5-9]. These guidelines have been updated to reflect the latest updated evidence around 2018, which included hepatobiliary contrast agent magnetic resonance imaging (HBA-MRI) and contrast-enhanced ultrasound (CEUS) in the diagnostic algorithm of HCC [10]. These two modalities are included as diagnostic tests in several later updated guidelines from other societies, including the Society of Liver Cancer of China (2019) and the Taiwan Liver Cancer Association and the Gastroenterological Society of Taiwan (2020) [11,12]. Accordingly, since 2018, the application and performance of updated guidelines using HBA-MRI or CEUS for HCC diagnosis have been evaluated in several studies [13-20].
Therefore, in this article, we summarize the studies evaluating the performance and limitations of HBA-MRI and CEUS for HCC diagnosis, which reflect the updated guidelines. We also briefly introduce the future aspects of HCC imaging that have not yet been adopted in the guidelines, but are being actively studied recently, namely abbreviated MRI and CEUS for surveillance of HCC and deep learning for imaging-based diagnosis of HCC.
HBA-MRI FOR HCC DIAGNOSIS
Imaging properties of HBA-MRI
HBAs are specialized contrast agents that are taken up by functioning hepatocytes and are excreted in the bile [21]. There are two currently available gadolinium-based HBAs: gadoxetic acid (Gd-EOB-DTPA) and gadobenate dimeglumine (Gd-BOPTA). However, Gd-EOB-DTPA is more widely used than Gd-BOPTA because of its better pharmacokinetics for clinical use: a higher rate of biliary excretion (50% vs. 3–5%) and earlier window for hepatobiliary phase (HBP) imaging (10–40 vs. 60–120 minutes) [21-24]. Therefore, HBA-MRI refers to Gd-EOB-DTPA-enhanced MRI in this review, unless otherwise mentioned.
Since HBA is taken up by hepatocytes via organic anion transporting polypeptide 8 (OATP8), expression of OATP8 is the main factor determining signal intensity in HBP [21,25,26]. OATP8 expression is known to be reduced during hepatocarcinogenesis; OATP8 is highly expressed in regenerative nodules and low-grade dysplastic nodules and is less expressed in many high-grade dysplastic nodules and HCCs [25]. Therefore, most HCCs and some high-grade dysplastic nodules are hypointense in HBP, while most regenerative nodules, low-grade dysplastic nodules, some high-grade dysplastic nodules, and only a minor portion (5–12%) of HCCs are isointense or hyperintense in HBP (Fig. 1) [26]. One important point is that the reduction in the expression of OATP8 occurs prior to portal venous flow reduction and neo-arterialization, which implies that even early HCCs without definite arterial phase hyperenhancement (APHE) can be detected in HBP as hypointense lesions [25,26]. The ability to detect early HCCs is one of the strengths of HBAs compared to conventional extracellular contrast agents (ECAs) in the diagnosis of HCC. In addition, strongly enhancing hepatic parenchyma in HBP against hypointense HCCs facilitates the delineation of HCCs (Fig. 1) [26]. Meanwhile, HCC diagnosis using HBP alone may lead to misinterpretation because HBP hypointensity is not a specific finding for HCC, as it can also be found in other hepatic lesions, including premalignant lesions of HCC, other cirrhotic nodules, hemangioma, and non-HCC malignancies [26,27].
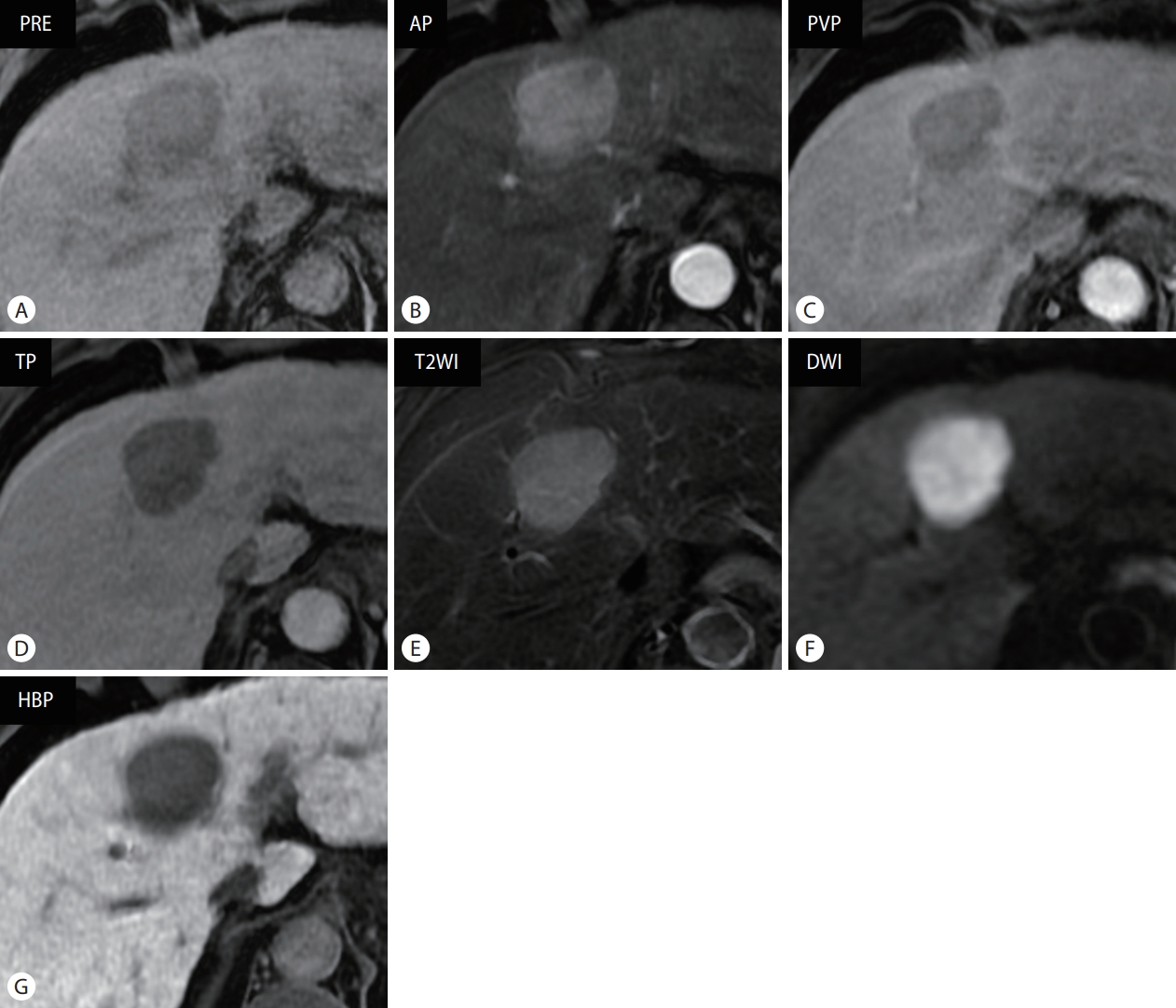
Typical magnetic resonance imaging findings of hepatocellular carcinoma using hepatobiliary contrast agent in a 61-year-old male patient with chronic hepatitis B. Approximately 4-cm sized mass lesion in liver segment 4, which shows (A) hypointensity in precontrast T1-weighted image, (B) arterial phase hyperenhancement, and (C) portal venous phase (PVP) and (D) transitional phase (TP) washout. It shows (E) moderate hyperintensity in fat-suppressed T2-weighted image and (F) diffusion restriction. (G) In the hepatobiliary phase (HBP) image acquired 20 minutes after contrast administration, the mass is clearly visualized with hypointense lesion in contrast to hyperintense hepatic parenchyma. PRE, precontrast; AP, arterial phase; T2WI, T2-weighted image; DWI, diffusion-weighted image.
Diagnostic performance and limitations of HBA-MRI
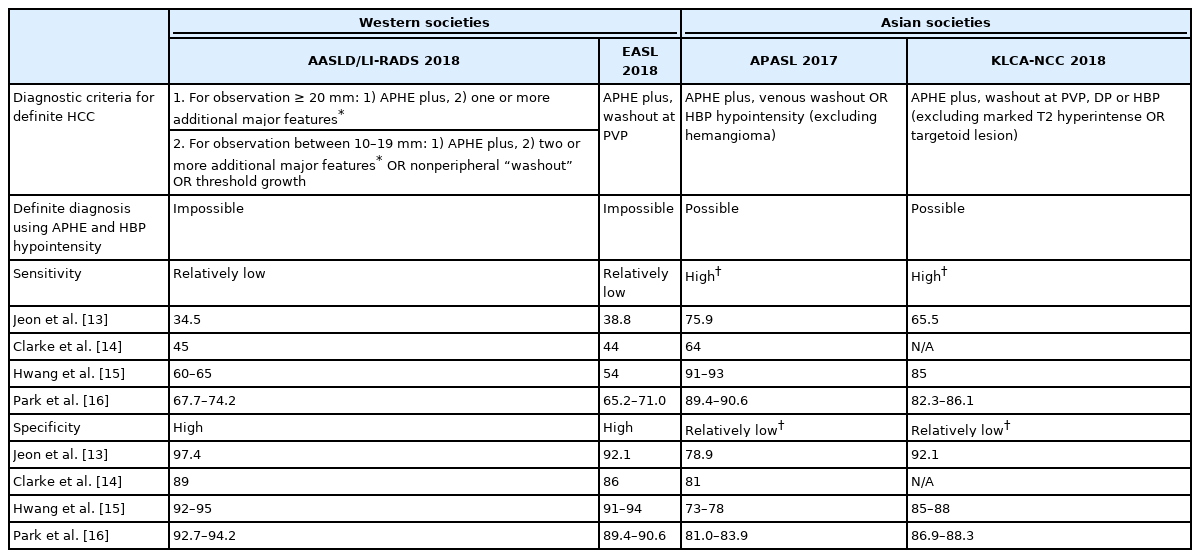
Since HBP hypointensity is sensitive but not specific for HCC diagnosis, whether the use of HBP hypointensity as a major imaging feature for the definite diagnosis of HCC differs among guidelines, which may be attributed to several factors including different treatment policies [4-10]. Guidelines from Western societies such as AASLD, LI-RADS, and EASL do not accept HBP hypointensity as a major feature for the definite diagnosis of HCC to avoid false-positive diagnoses. However, the guidelines from Asian societies such as APASL and KLCA-NCC permit the definite diagnosis of HCC using a combination of APHE and HBP hypointensity, regardless of portal washout, to achieve high sensitivity to enable initiation of early locoregional treatment [4-10]. The use of HBP hypointensity for definite diagnosis of HCC, however, may reduce specificity because it is not a specific feature of HCC [26,27]. Therefore, to maintain specificity, Asian guidelines have additional exclusion criteria. For example, KLCA-NCC excludes lesions with marked T2 hyperintensity or targetoid appearance, with a reported specificity of up to 92.1% [9,13]. APASL also excludes cavernous hemangioma, but does not exclude targetoid lesions, which may result in specificity loss [8]. Multiple retrospective studies evaluating the diagnostic performance of HCC diagnostic algorithms according to the updated guidelines in 2018 reflect these differences: Western guidelines showed greater specificity (LI-RADS, 89–97.4%; EASL, 86–94.9%) but lower sensitivity (LI-RADS, 34.5–74.2%; EASL, 38.8–71.0%), while Asian guidelines showed greater sensitivity (APASL, 64–90.6%; KLCA-NCC, 65.5–86.1%) with relatively lower specificity (APASL, 73–83.9%; KLCA-NCC, 85–92.1%). Among Asian guidelines, APASL seems to be more sensitive but less specific than KLCA-NCC, as expected (Table 1) [13-16].
Discrepancy in diagnostic criteria and performance for HCC using HBA-MRI between Western and Asian societies
Despite the potential benefits of the sensitive detection of HCC using HBP images, HBA-MRI has several disadvantages compared to ECA-MRI. The absence of a true interstitial phase and a challenging arterial phase acquisition are the most problematic disadvantages. In HBA-MRI, extracellular-dominant and hepatocellular-dominant enhancements overlap at the transitional phase (TP; which corresponds to the delayed phase in ECA-MRI); therefore, hypointensity in TP may be either due to true washout or increased background parenchymal enhancement [26,28]. Therefore, Western guidelines such as AASLD, LI-RADS, and EASL do not include TP for washout assessment to maintain specificity when using HBA, which may entail decreased sensitivity for the detection of washout [5-7]. The strong parenchymal enhancement at the TP can also hinder detection of the “enhancing capsule,” which is one of the major imaging features of HCC. Previous studies showed a lower frequency of identifying the “enhancing capsule” in HCC when using HBA compared to ECA (31–47.4% vs. 73–87.4%) [29-31]. In addition, a smaller dose of HBA (0.025 mmol/kg) compared to ECA (0.1 mmol/kg) and the considerable occurrence of transient severe motion artifact due to impaired breath-hold ability after HBA administration may decrease the sensitivity for APHE detection [32,33]. These disadvantages may hamper the detection of major imaging features (i.e., APHE, delayed washout, and enhancing capsule) and may lead to a lower sensitivity for the definite diagnosis of HCC. Indeed, a few studies after the revision of the guidelines around 2018 showed that HBA-MRI is less sensitive than ECA-MRI for the definite diagnosis of HCC when applying LI-RADS (sensitivity, 67.3–71.2% vs. 78.9–83.1%), and comparable or less sensitive when applying EASL (sensitivity, 63.0– 67.5% vs. 71.5–76.2%) [29,34,35]. However, another study showed that HBA-MRI had comparable sensitivity to ECA-MRI when using the LI-RADS LR-5 criteria (78.1% vs. 73.7%) and a higher sensitivity than ECA-MRI for HCCs <20 mm (70.8% vs. 50.0%) [36]. Further studies are needed to determine the effect of these disadvantages of HBA on the diagnostic performance of HBA-MRI for HCC.
Several efforts have been made to improve the sensitivity of HBA-MRI using strict criteria such as LI-RADS, mainly in Asia, by altering the criteria or imaging sequences. For instance, a study showed that modifying the LI-RADS LR-5 criteria by extending “washout” to hypointensity in portal venous phase (PVP) or TP and “capsule” to either enhancing capsule appearance or non-enhancing capsule appearance in PVP or TP can increase sensitivity (79.2% vs. 60.4%) without significantly reducing the specificity (93.5% vs. 95.7%) [37]. Another study showed that using one of the independently significant ancillary features such as mild-moderate T2 hyperintensity, HBP hypointensity, non-enhancing “capsule,” or mosaic appearance to upgrade from LR-4 to LR-5 increased sensitivity (69.4–76.9% according to ancillary features used to upgrade vs. 66.2%) without a significant decrease in specificity (95.3–96.5% vs. 96.5%) [38]. The use of arterial subtraction images may overcome the weak APHE of HBA-MRI. Using arterial subtraction images can increase the detection rate of APHE in HCC (91.9% vs. 80.6%, compared to conventional arterial phase images) and increase the sensitivity of LI-RADS LR-5 for HCC diagnosis (64.1% vs. 55.9%) without a significant reduction in specificity (92.9% vs. 94.9%) [39]. Other studies reported that using later acquisition of PVP images after 70 seconds from the contrast injection detected more “washout” (83.6–84.1% vs. 50.9–64.6%) and enhancing “capsule” (27.6% vs. 19.8%) in HCC compared to using conventional PVP images, and may increase sensitivity (83.6% vs. 53.5%, LI-RADS; 82.8% vs. 50.0%, EASL) without a significant decrease in specificity (93.2% vs. 93.2%, both) for the diagnosis of HCC using the LI-RADS criteria [40,41]. The combined use of conventional and subtraction PVP images aided the detection of “washout” (detection frequency, 83% vs. 77%, compared to using conventional PVP only) and enhancing “capsule” (62% vs. 36%) [42]. However, these studies were performed retrospectively within a single center; a multi-center study with a prospective design is warranted to validate these promising results.
Gd-BOPTA-enhanced MRI
To our knowledge, only a few studies regarding MRI using Gd-BOPTA for the diagnosis of HCC have been published recently [43-46]. Similar to MRI using Gd-EOB-DTPA, HBP hypointensity on MRI using Gd-BOPTA is sensitive (sensitivity, 94.1%) but not specific (specificity, 26.9%) for HCC [44], and adding HBP hypointensity as a major feature for the definite diagnosis of HCC may increase the sensitivity for the detection of HCC using LI-RADS [44-46]. One study showed that APHE was seen similarly on MRI using Gd-BOPTA and Gd-EOB-DTPA (91.5% vs. 88.0%), while MRI using Gd-BOPTA detected more “washout” (60.2% vs. 45.3%) and enhancing “capsule” (50.2% vs. 33.3%); this is because as Gd-BOPTA is taken up by hepatocytes later than Gd-EOB-DTPA, the disadvantages related to TP, restricting the detection of “washout” in the portal phase only and hindering the detection of enhancing “capsule,” do not occur when using Gd-BOPTA [43]. However, as mentioned above, Gd-BOPTA has a disadvantage in that 60–120 minutes delay is needed to obtain HBP image, which may raise logistical issues [21]. Currently, there is no head-to-head comparison between Gd-BOPTA and Gd-EOB-DTPA for HCC diagnosis using recently modified criteria, warranting further investigation.
Comparison with other modalities: computed tomography (CT) and ECA-MRI
Although most major guidelines do not set the preferred imaging modalities among CT, ECA-MRI, and HBA-MRI for HCC diagnosis, previous meta-analyses have shown that HBA-MRI has a greater diagnostic accuracy with higher per-lesion sensitivity than CT (85–85.6% vs. 68–73.6%) and comparable specificity (94% vs. 93%) [47,48]. However, there have been mixed results regarding the comparison between HBA-MRI and ECA-MRI. Previous meta-analyses reported higher per-lesion sensitivity for HBA-MRI than ECA-MRI (85.6–87% vs. 74–77.5%), whereas more recent meta-analyses showed similar diagnostic performance for HBA-MRI and ECA-MRI (sensitivity, 76% vs. 72%; specificity, 92% vs. 92%) [47,49,50]. Caution is warranted in interpreting these results, as these differences in diagnostic accuracy may also stem from different study populations in different geographic regions (i.e., the proportion of subjects with chronic hepatitis B without cirrhosis) or different criteria for HCC diagnosis in each study, aside from using different contrast agent properties. For instance, in the latter meta-analysis, the sensitivity of HBA-MRI was 75% in the subgroup with hepatitis B while 59% in the subgroup with hepatitis C or alcoholic hepatitis, although there was no significant difference in sensitivity values between ECA-MRI and HBA-MRI in both subgroups [49]. In addition, the latter meta-analysis showed that HBA-MRI using the modified LI-RADS or EASL criteria with extended washout had higher sensitivity (83%) with reduced specificity (85%) than HBA-MRI or ECA-MRI using the conventional LI-RADS or EASL criteria (sensitivity, 66% and 68%; specificity, 91% and 94%, respectively) [49]. Another recent meta-analysis showed that HBA-MRI using strict criteria (i.e., accept washout in PVP only) had a lower sensitivity (63%) than HBA-MRI using extended criteria (i.e., extended washout to TP or HBP) (74%) or ECA-MRI (76%), while there were no significant differences in specificity (98%, 93%, and 96%, respectively) [51]. Therefore, further studies are needed to optimize the imaging criteria for HCC using HBA-MRI.
CEUS FOR HCC DIAGNOSIS
Imaging properties of CEUS
CEUS is another useful imaging modality for the diagnosis of focal hepatic lesions, which has been recognized recently as an important tool for HCC diagnosis in LI-RADS, EASL, APASL, and KLCA-NCC guidelines [6-9]. CEUS uses microbubble contrast agents with a diameter of 2–5 µm, which cannot pass through the vascular endothelium into the interstitial space [52]. Therefore, most ultrasound contrast agents (i.e., SonoVue/Lumason, Bracco, Milan, Italy and Definity/Luminity, Lantheus Medical Imaging, N. Billerica, MA, USA) are intravascular agents. One exception is Sonazoid (Daiichi-Sankyo, Tokyo, Japan; GE Healthcare, Chicago, IL, USA), taken up by Kupffer cells, which will be discussed later [53,54].
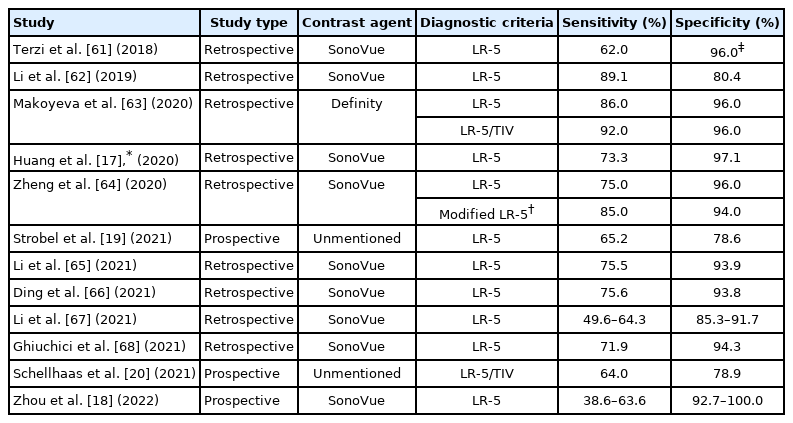
Due to the different pharmacokinetics of contrast agents used in ultrasound and CT/MRI, a substantial portion of intrahepatic cholangiocarcinomas (iCCAs) in cirrhotic livers show homogeneous APHE with washout in CEUS [55]. Therefore, diagnosing HCC solely by “APHE and washout” in CEUS can lead to the misdiagnosis of iCCA for HCC. However, several studies have shown different patterns of washout between HCC and iCCA in terms of timing and degree of washout; HCC usually shows late and mild washout (onset ≥60 seconds and less enhanced than liver but not devoid of enhancement), while iCCA shows early and marked washout (onset <60 seconds and virtually devoid of enhancement) (Fig. 2) [56-60]. Using the diagnostic criteria of “APHE with late and mild washout” for HCC by CEUS, many studies reported a good specificity (78.6–100%) but a lower sensitivity (38.6–92%) for HCC diagnosis, especially when compared to the conventional “APHE and washout” criteria or the subjective on-site diagnosis (Tables 2, 3) [17-20,61-68]. Several recent meta-analyses regarding CEUS LI-RADS reported a pooled sensitivity and specificity of 69–73% and 88–95% for LR-5, respectively [69-71].
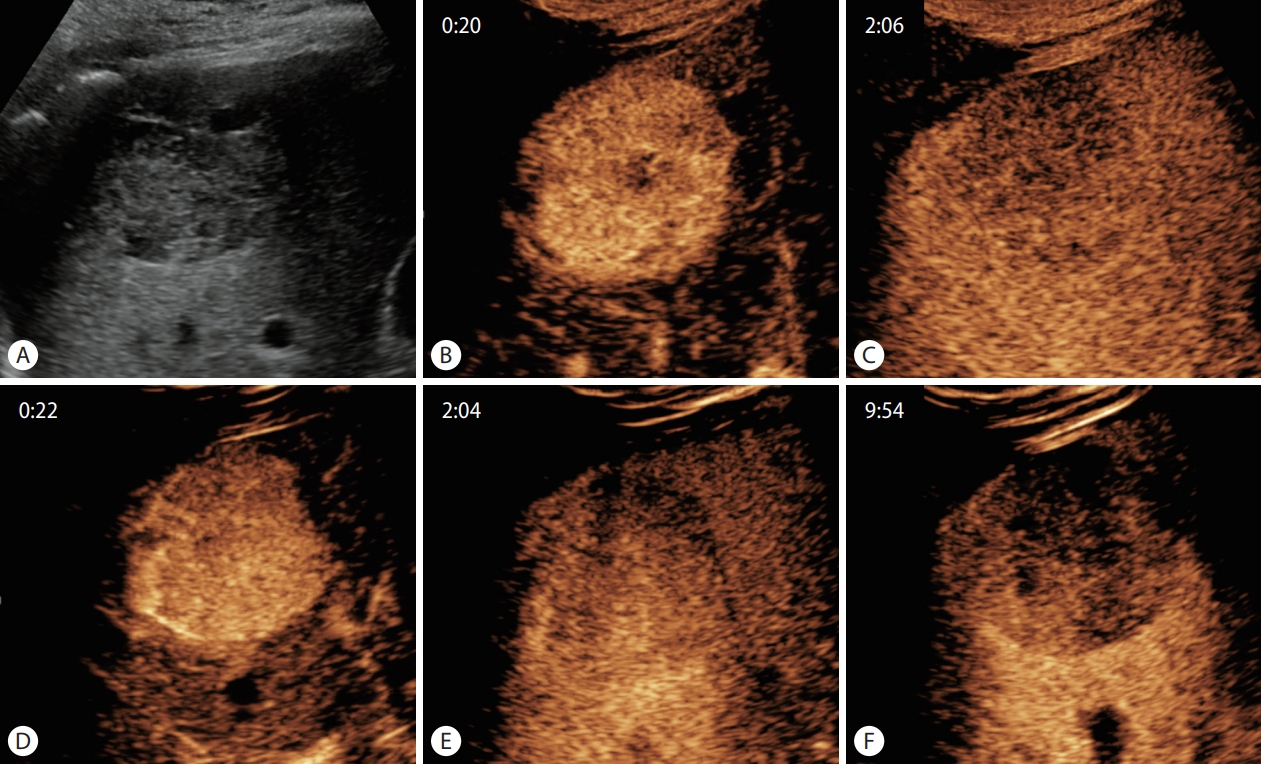
Typical contrast-enhanced ultrasound findings of hepatocellular carcinoma using SonoVue and Sonazoid. (A) Approximately 4.5-cm sized hypoechoic mass in liver segment 6 on B-mode ultrasound. After administration of SonoVue, the mass shows (B) hyperenhancement in the arterial phase (20 seconds) and (C) mild washout in the delayed phase, but not devoid of enhancement (126 seconds). The same lesion enhanced with Sonazoid also shows (D) arterial phase hyperenhancement (22 seconds) and (E) mild delayed washout (124 seconds), as well as (F) clear hypointensity in the Kupffer phase (approximately 10 minutes after contrast administration).
Diagnostic performance of CEUS LI-RADS for HCC

Comparison of diagnostic performance for HCC between CEUS LI-RADS and other diagnostic criteria
Advantages and limitations of CEUS
Despite the unsatisfactory sensitivity of CEUS due to the strict criteria for HCC diagnosis when used alone, CEUS has inherent advantages compared to CT/MRI. Unlike CT/MRI, which uses a predetermined scanning delay for the arterial phase, CEUS enables real-time arterial phase evaluation. Therefore, CEUS can be more sensitive when reevaluating APHE detection for lesions that lack APHE on CT/MRI due to mistiming [53,72,73]. Indeed, most major guidelines recommend using CEUS as a second-line modality when first-line examinations (i.e., CT or MRI) are inconclusive [7-9]. Several studies have shown that CEUS can depict more APHE and/or washout when used as a second-line modality for indeterminate lesions on CT/MRI (i.e., LR-3 or LR-4 lesions), and it can correctly upgrade the LI-RADS category from LR-3 or LR-4 to LR4, LR-5, or LR-M with few false positives [74-76]. In addition, arterioportal shunts or vascular pseudolesions are rarely visualized on CEUS, which are common pseudolesions mimicking true hepatic lesions and therefore inadequately categorized as LR-3 or LR-4 on CT/MRI [53,77,78]. Indeed, CEUS combined with grayscale ultrasound differentiated vascular pseudolesions such as arterioportal shunts from true nodules when MRI findings were inconclusive, with a small number of false negatives [75]. Another recent prospective study also showed the usefulness of CEUS as a second-line modality; although CEUS alone is less sensitive than HBA-MRI (60.8% vs. 72.2% and 86.1% according to EASL and KLCA-NCC guidelines, respectively), the additional use of CEUS for inconclusive lesions on HBA-MRI as a second-line modality can increase sensitivity (83.5% and 91.1% vs. 72.2% and 86.1% according to EASL and KLCA-NCC guidelines, respectively) with no additional false positives [79].
CEUS can also offer quantitative features of dynamic contrast enhancement by analyzing the time-intensity curve, and it may be used for differentiating HCCs from other hepatic tumors [80-84]. One study comparing quantitative CEUS parameters between HCC and focal nodular hyperplasia reported that maximum intensity and rise slope were higher in focal nodular hyperplasia, while rise time and time-to-peak were higher in HCC [82]. Two other studies reported differences in quantitative parameters, including washout time and maximum intensity between HCC and metastasis, and area under curves (AUCs) for washout time for differentiating HCC and metastasis are reported to be 0.780 and 0.922, respectively [83,84]. However, further studies are required to validate these results.
CEUS has several inherent limitations of ultrasound, such as operator dependency, limited sonic window, especially in patients with advanced cirrhosis, and limited capability for staging [54,85]. Several recent studies have shown mixed results for the inter-reader agreement of the CEUS LI-RADS criteria [18,62,63,67]. Inter-reader agreement of CEUS LI-RADS criteria has been reported to vary according to studies, ranging from moderate to excellent (κ=0.60–0.90) [18,62,63,67]. Among the imaging features of HCC on CEUS, inter-reader agreement was best in APHE (κ=0.65–0.83), followed by washout (κ=0.52–0.71), and ancillary features such as mosaic architecture (κ=0.124) or nodule-in-nodule appearance (κ=0.098) [18,62]. Another limitation is that CEUS permits the characterization of a limited number of targeted lesions on a single examination [60]. Thus, CEUS is not recommended for use in staging in LI-RADS, EASL, KLCA-NCC, and World Federation for Ultrasound in Medicine and Biology guidelines, and additional CT/MRI is required for staging even if HCC is diagnosed solely by CEUS [7,9,60,81].
Sonazoid-enhanced ultrasound
While LI-RADS, EASL, and KLCA-NCC allow only intravascular agents for HCC diagnosis, APASL accepts Sonazoid to diagnose HCC; nodules showing hypervascularity and/or Kupffer phase defects (discussed below) on Sonazoid-enhanced ultrasound can be diagnosed as HCC according to the APASL guideline [7-9,60]. Sonazoid is a liver-specific ultrasound contrast agent that is taken up by Kupffer cells after initial vascular distribution, enabling Kupffer phase (postvascular phase) imaging as well as vascular phase imaging [85]. Compared to intravascular agents, which use a low mechanical index (<0.1 MI), Sonazoid-enhanced ultrasound uses an intermediate mechanical index in the range of 0.2–0.3 due to its higher resistance to acoustic pressure [85]. With Sonazoid, imaging acquisition during the vascular phase, including the arterial phase and the PVP, is similar to that of intravascular agents, but following the vascular phase, an additional Kupffer phase, when microbubbles are accumulated in the Kupffer cells by phagocytosis, can be available [85]. Most malignant hepatic tumors, including HCCs, appear as non-enhancing or hypoenhancing defects in the Kupffer phase due to depletion of Kupffer cells, whereas most benign hepatocyte-origin tumors are iso- or hyperechoic at the Kupffer phase (Fig. 2). In addition, re-injection of Sonazoid in the Kupffer phase allows evaluation of arterial flow in Kupffer phase defect lesions; these properties may help increase the diagnostic performance of Sonazoid-enhanced ultrasound [85,86].
Sonazoid-enhanced ultrasound has several limitations related to the Kupffer phase. First, Kupffer phase defects may not be adequately evaluated in hyperechoic lesions when using low-mechanical index contrast imaging due to the influence of the background B-mode signal, which can result in false-negative nodules [87,88]. Second, a substantial portion of well-differentiated HCCs showed iso-enhancement in the Kupffer phase. One study using intraoperative CEUS showed that the proportion of hypoechogenicity in the Kupffer phase is significantly lower in well-differentiated HCCs than in moderately or poorly differentiated HCCs (54% vs. 92%), while another study reported that 83% of early HCCs were isoechoic at the Kupffer phase [89,90]. Lastly, similar to Gd-EOB-DTPA, theoretically, the additional enhancement via Kupffer cell uptake of bubbles during the TP of Sonazoid-enhanced ultrasound might cause the pseudo-washout effect (Table 4) [91].

Differences between SonoVue and Sonazoid for HCC diagnosis
Despite these limitations, a recent meta-analysis reported a good diagnostic performance for Sonazoid-enhanced ultrasound with pooled sensitivity and specificity of 90% and 97%, respectively, albeit with significant heterogeneity among studies [92]. There have been efforts to use Sonazoid using the CEUS LI-RADS criteria [91,93]. For instance, the modified CEUS LI-RADS LR-5 criteria, which included nodules ≥1 cm in size, non-rim and non-peripheral discontinuous globular APHE, late washout, and hypoenhancement in the Kupffer phase, showed sensitivity, specificity, and positive predictive value for modified LR-5 of 70.3%, 92.5%, and 93.8%, respectively, with miscategorization as LR-5 for two of 10 hemangiomas [93]. Even without the Kupffer phase, Sonazoid-enhanced ultrasound showed better sensitivity than SonoVue-enhanced CEUS (79% vs. 67%) with comparable specificity (both 100%) [91]. This difference possibly stemmed from the different washout profiles of the two contrast agents. Sonazoid-enhanced ultrasound showed a later washout time than SonoVue-enhanced CEUS (101 vs. 84 seconds), which may enable the detection of the late washout of HCCs more frequently. However, the reason for the different washout profiles between the two CEUS agents is not well known [91,94]. Until now, there has been no consensus regarding the diagnostic criteria for diagnosis of HCC on Sonazoid-enhanced ultrasound. Although the combination of APHE and Kupffer phase hypoenhancement of a hepatic lesion may provide high sensitivity, the downside would be a low specificity. Similar to HCC diagnostic criteria of KLCA-NCC guideline with HBA-MRI, it might be considered that the timing for determining late/mild washout criteria could be extended to Kupffer phase, only after excluding peripheral globular enhancement, rim APHE, rapid washout within 60 seconds, or marked washout (punchout appearance) within 2 minutes after contrast injection. In addition, contrast dosage and image acquisition methods vary between studies; either vendor-recommended dose or reduced dose can be used and late vascular phases or TP may or may not be obtained [85,91,93]. Based on the studies so far, Sonazoid-enhanced ultrasound is expected to be included as a diagnostic modality for HCC in 2022 KLCA-NCC guideline. Nevertheless, further studies are still warranted to validate these results, refine the diagnostic criteria, and standardize the protocol for Sonazoid-enhanced ultrasound.
FUTURE ASPECTS FOR HCC SURVEILLANCE AND DIAGNOSIS
Novel strategies for HCC surveillance: abbreviated MRI and CEUS
Current guidelines recommend surveillance in patients at risk of HCC with biannual ultrasound with or without serum alpha-fetoprotein measurement [5,7-9]. Previous studies, including randomized controlled trials, have shown that biannual surveillance of HCC using ultrasound significantly reduced overall or HCC-related mortality [95-97]. However, ultrasound has the limitation of low detection sensitivity for HCC, and a meta-analysis showed sensitivities for detecting early HCC in patients with cirrhosis of 63% and 45% using ultrasound with and without serum alpha-fetoprotein measurements, respectively [98,99]. Dynamic CT and MRI more sensitively detect HCC than ultrasound; however, the former has a risk of ionizing radiation exposure, while the latter has drawbacks in terms of cost and time effectiveness for HCC surveillance [98]. Therefore, novel strategies for HCC surveillance, abbreviated MRI and CEUS, have been studied to overcome the limitations of current surveillance modalities.
Abbreviated MRI is a simplified MRI protocol tailored to evaluate a specific disease. While complete liver MRI takes approximately 40 minutes to perform, abbreviated MRI involves only a few sequences necessary for HCC detection and is typically performed within 15 minutes, although it depends on the protocol [98]. Abbreviated MRI studies for HCC surveillance can be classified into three approaches: 1) non-contrast abbreviated MRI, typically consisting of T1-weighted in-phase/out-of-phase, T2-weighted, and diffusion-weighted imaging; 2) dynamic contrast-enhanced abbreviated MRI, typically consisting of pre-contrast, arterial, portal venous, and delayed phase imaging; and 3) HBP abbreviated MRI, typically consisting of HBP and T2-weighted imaging with or without diffusion-weighted imaging. Detailed information on the sequences, advantages, and disadvantages of each approach are beyond the scope of this paper and are available in another focused review [100].
To date, most studies regarding surveillance of HCC using abbreviated MRI have been performed retrospectively by simulating abbreviated MRI protocols from complete liver MRI. These retrospective, simulated studies have shown relatively good diagnostic performance (per-patient sensitivity, 61.5–92.1%; specificity, 76.4–100%) [101-110]. Recent meta-analyses reported pooled sensitivity and specificity of abbreviated MRI for detecting HCC of 86% and 94–96%, respectively, which were higher than those of ultrasound (sensitivity, 82% vs. 53%; specificity, 98% vs. 88%) [111,112]. However, few studies have focused on the performance of abbreviated MRI in a real surveillance setting [113]. Currently, prospective studies are ongoing, and they are expected to provide prospective data of abbreviated MRI that can validate the results of existing studies [114,115].
Sonazoid-enhanced ultrasound also has the potential to be used for the surveillance of HCC in high-risk patients. Sonazoid allows Kupffer phase imaging, which has a very stable time window of at least 60 minutes, and allows enough time to evaluate the entire liver for HCC surveillance [85,116]. A randomized controlled trial showed that Sonazoid-enhanced ultrasound can detect significantly smaller HCC nodules than B-mode ultrasound (13.0 vs. 16.7 mm) in patients with high risk for HCC development, even with shorter examination time (6.6 vs. 16.2 minutes) [117]. Although another prospective study did not find significant improvement in detecting early HCC by adding Sonazoid-enhanced ultrasound in routine ultrasound surveillance (detection rate, 1.1% vs. 0.8%), the false-referral rate was significantly reduced when CEUS was additionally used (1.1% vs. 4.4%) [116]. However, further studies regarding survival benefit and cost-effectiveness are warranted to clarify the benefits of CEUS in HCC surveillance. So far, the Asian Federation of Societies for Ultrasound in Medicine and Biology permits CEUS for HCC surveillance, especially in patients with very coarse liver parenchyma, while the World Federation for Ultrasound in Medicine and Biology does not recommend routine use of CEUS for HCC surveillance [81,85].
Deep learning in HCC diagnosis
Deep learning is a subset of machine learning that uses an architecture of artificial neural networks inspired by biological neural networks. Unlike classic machine learning methods, which depend on hand-engineered features, deep learning methods bypass feature engineering and learn features directly from data [118,119]. Deep learning has shown breakthrough performance improvements in various fields, including image analysis. A convolutional neural network is a deep learning architecture consisting of convolutional, pooling, and fully connected layers, which is the most commonly used architecture for processing images. Detailed information on deep learning and convolutional neural network is available in another focused review [118]. Regarding HCC imaging, deep learning has been studied not only for diagnosis but also for other fields such as segmentation, pathologic grading, and prediction of treatment response and prognosis [120]. In this article, we briefly introduce several studies on deep learning for the detection and diagnosis of HCC.
Deep learning algorithms for HCC diagnosis have been applied to multiple imaging modalities, including ultrasound, CT, and MRI. For ultrasound, Schmauch et al. [121] designed an ensemble model of ResNet50 and DenseNet to detect focal liver lesions from ultrasound and classified them as benign or malignant lesions, and reported AUCs of 0.935 and 0.916 in the test set for detection and classification, respectively. Yang et al. [122] developed another convolutional neural network model on ultrasound images combined with clinical information for the classification of focal liver lesions into benign or malignant lesions, which showed an AUC of 0.924 and higher sensitivity and specificity than expert radiologists on external datasets (86.5% vs. 76.1% and 85.5% vs. 76.9%, respectively). For CT, Yasaka et al. [123] trained a convolutional neural network model for the classification of liver masses into five categories (A, classic HCCs; B, malignant liver tumors other than classic and early HCCs; C, indeterminate masses or masslike lesions and rare benign liver masses other than hemangiomas and cysts; D, hemangiomas; and E, cysts), and the model showed an accuracy for the classification of liver masses of 84% and AUC differentiating A–B vs. C–E of 0.92. Another study on deep learning-based liver tumor classification on MRI showed 90.0% accuracy for differentiation between cysts, hemangiomas, focal nodular hyperplasias, HCCs, iCCAs, and colorectal cancer metastases and an AUC of 0.992 for HCC diagnosis, although only masses with typical imaging findings were included and the model was not externally validated [124]. More recent studies regarding deep learning algorithms showed comparable performance to radiologists for the classification of a liver mass on CT (accuracy for classification between HCC and non-HCC, 80.5% vs. 79.3%) or MRI (sensitivity and specificity for classification between benign and malignant, 91.9% vs. 89.1% and 94.1% vs. 90.4%, respectively) in external datasets [125,126]. In addition to classification, deep learning-based detection of HCCs on CT or MRI has been studied. One study developed a deep-learning algorithm for detecting HCCs on HBP images, which showed comparable performance to less-experienced radiologists on external datasets (sensitivity and specificity, 87% vs. 86% and 93% vs. 92%, respectively) [127]. Other studies also showed relatively good performance of deep-learning algorithms for detecting HCCs on CT (sensitivity, 92.0% and false-positive rate, 13.7%) or MRI (sensitivity, 89.7% and positive predictive value, 85.0% for lesions ≤2 cm) [128,129]. Regarding LI-RADS, one study reported that deep learning methods on MRI can distinguish between LR-3 and LR-4 or LR-5 lesions with an accuracy of 90% in the test set [130]. However, another study showed that the overall accuracy of the deep learning model for LI-RADS classification was only 41.2% and 47.7% in external CT and MRI datasets, respectively, although it had limitations in that only a small number of images were used for training [131]. Further investigations using larger multi-center data may be warranted to apply deep learning models in LI-RADS classification.
CONCLUSION
In recent years, several major guidelines for HCC have newly included HBA-MRI as the primary diagnostic test or CEUS as a second-line diagnostic test. Several studies have demonstrated that strongly enhanced hepatic parenchyma in HBP allows for better detection of HCC and staging of HCC. In addition, the usefulness of CEUS as a second-line modality has been reported to increase sensitivity without losing specificity. However, to date, there are significant discrepancies in the diagnostic criteria of HBA-MRI and preferred CEUS agents among major guidelines, which could be related to the prevalence of HCC and its treatment patterns in various regions. The application of novel surveillance strategies such as abbreviated MRI or CEUS and deep learning for HCC needs further validation in the near future. To resolve these issues, further large-scale prospective studies are required. Finally, the development and adoption of a universal lexicon for liver imaging would be necessary to decrease gaps between guidelines, enhance communication, and facilitate future scientific research.
Notes
Authors’ contributions
Study conception and design: Jeong Min Lee, Tae-Hyung Kim
Acquisition of data: Junghoan Park
Drafting of the manuscript: Junghoan Park
Critical revision of the manuscript: Jeong Min Lee, Tae-Hyung Kim, Jeong Hee Yoon
Conflicts of Interest
Jeong Min Lee received grants from Bayer Healthcare, Canon Healthcare, Philips Healthcare, GE Healthcare, CMS, Guerbet, Samsung Medison, Bracco, personal fees from Bayer Healthcare, Siemens Healthineer, Samsung Medison, Guerbet, outside the submitted work. Jeong Hee Yoon received personal fees from Bayer and Philips Healthcare. Other authors have no conflicts of interest.
Acknowledgements
We thank Sungeun Park and Hyo-Jin Kang for courtesy of the hepatobiliary MRI and CEUS images.
Abbreviations
AASLD
the American Association for the Study of Liver Diseases
APASL
the Asian Pacific Association for the Study of the Liver
APHE
arterial phase hyperenhancement
AUC
area under curve
CEUS
contrast-enhanced ultrasound
CT
computed tomography
EASL
the European Association for the Study of the Liver
ECA
extracellular contrast agent
Gd-BOPTA
gadobenate dimeglumine
Gd-EOB-DTPA
gadoxetic acid
HBA-MRI
hepatobiliary contrast agent magnetic resonance imaging
HBP
hepatobiliary phase
HCC
hepatocellular carcinoma
iCCA
intrahepatic cholangiocarcinoma
KLCA-NCC
the Korean Liver Cancer Association-National Cancer Center
LI-RADS
Liver Imaging Reporting and Data System
OATP8
organic anion transporting polypeptide 8
PVP
portal venous phase
TP
transitional phase