


Graphical Abstract
INTRODUCTION
Coronavirus disease 2019 (COVID-19) has affected over 400 million people and caused near nearly 6 million deaths globally as of March 2022 [1]. Vaccination has high efficacy profile against COVID-19 infection using different vaccine platforms, such as mRNA (e.g., BNT162b2 [2], mRNA-1273 [3]), adenoviral vector (e.g., ChAdOx1 nCov-19/AZD1222 [4]), and inactivated vaccines (e.g., CoronaVac [5], BBIBP-CorV [6]). However, these trials had limited data on patients with chronic liver disease (CLD).
CLD is associated with higher risk of adverse outcomes following COVID-19 infection, especially those with liver cirrhosis [7,8]. Immunogenicity and safety of COVID-19 vaccine is a concern in this group of patients, as cirrhosis affects innate and adaptive immune response [9]. A study of 581 subjects receiving inactivated vaccines revealed that the seroconversion rates of neutralizing antibody (Nab) were 76.8%, 78.9%, and 76.7% among non-cirrhosis, compensated and decompensated cirrhosis groups respectively, in comparison with healthy subjects (90.3%) [10]. However, other studies reported a higher seroconversion rate of at least 90% among CLD patients [11,12].
Due to use of immunosuppressants, liver transplant (LT) recipients are at higher risk of severe infection [13], and have attenuated response to vaccinations against other diseases [14]. Lower immunogenicity was reported in LT recipients (73.9%) comparing with cirrhotic patients (100%) and controls (100%) [15]. An even lower seroconversion rate of <50% was reported in some studies [16-21].
The conflicting data of COVID-19 vaccine immunogenicity among CLD patients and LT recipients could be related to significant heterogeneity among studies in terms of CLD etiology, cirrhosis status, vaccine platform and type of antibody measured (including Nab, anti-spike receptor binding domain [RBD] antibody and anti-spike antibody). Currently, Nab level is a surrogate marker of vaccine effectiveness [22] and is predictive of protection from symptomatic COVID-19 infection [23,24]. Although levels of anti-spike antibody correlate with Nab, seropositivity is lower upon measurement of Nab than anti-spike antibody [11,25,26].
We therefore performed a systematic review and meta-analysis to summarize data on vaccine immunogenicity and reactogenicity among patients with liver diseases with stratification according to etiology, cirrhosis status, vaccine platform and type of antibody measured.
MATERIALS AND METHODS
Data sources and searches
We searched electronic databases MEDLINE (OVID), EMBASE, and Cochrane Library from inception to February 16, 2022. Keywords include liver disease, LT, organ transplant, COVID-19, vaccination. The search details can be found in Appendix 1. This review was conducted and reported in consonance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Study selection
Two reviewers (KSC, CHM) screened the titles and abstracts independently for inclusion. Full texts were retrieved if they met the inclusion criteria and assessed independently, and dissonance was resolved by WKS and MFY. Inclusion criteria included (1) study population: CLD patients and LT recipients; (2) intervention: COVID-19 vaccines (including CoronaVac, BBIBP-CorV, WIBP-CorV, BNT162b2, mRNA-1273, AZD1222); (3) study design: randomized controlled trials and observational studies; and (4) primary outcome: seroconversion rate of either Nab or anti-spike antibody. Secondary outcomes are T cell immune response and frequency of adverse events.
Exclusion criteria included (i) age <18 years; (ii) history of COVID-19 infection; and (iii) non-original studies, such as systematic reviews, meta-analysis, review articles, or guidelines. A summary of studies identified, included, and excluded is shown in PRISMA flow diagram (Supplementary Fig. 1).
Data extraction and quality assessment
For eligible studies, we recorded the first author, site of study, study duration, sample size, age, sex, causes of CLD and LT, COVID-19 vaccine type administered, antibody type measured, time interval of antibody measurement from second dose of vaccination, method of antibody test, and cut-off of antibody level regarded as seropositive (Table 1).
The quality of observational studies was assessed using Newcastle-Ottawa scale (NOS). Risk of bias was categorized into three groups: low risk (7ŌĆō9 points), moderate risk (4ŌĆō6 points), and high risk (<4 points) [27].
Data analysis
All statistical analyses were conducted in R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) statistical software. Continuous variables were expressed as median (interquartile range [IQR]) or mean┬▒standard deviation). The pooled rate of seroconversion and adverse events were expressed as proportion and 95% confidence interval (95% CI) using random effects model, and was presented as Forest plot. A P-value of <0.05 was used to define statistical significance. We used Cochran Q test to detect heterogeneity among studies, with a P-value <0.10 indicating significant heterogeneity. We calculated I2 statistic to measure proportion of total variation in study estimates attributed to heterogeneity. I2 values of Ōēź50% and Ōēź75% indicate substantial and considerable heterogeneity, respectively [28]. Meta-regression analysis was used to examine association between background characteristics of the included studies and pooled seroconversion rates [29].
We assessed publication bias by funnel plot and Egger regression. Publication bias was considered significant if P-value of Egger regression is <0.1 [30]. The trim-and-fill method was used to adjust for publication bias, if present, which re-estimated the effect size after imputing potentially missing studies.
Subgroup analysis was performed according to type of antibody tested, method of antibody test (electrochemiluminescence immunoassay analyzer [ECLIA], enzyme-linked immunosorbent assay [ELISA], and chemiluminescence immunoassays [CLIA]), age (with a cut-off of 60 years), etiology of CLD, cirrhosis status, vaccine platform, individual vaccine type, use of multiple immunosuppressants, and region, where applicable.
RESULTS
Study characteristics of meta-analysis
Supplementary Figure 1 depicts the study selection process. Of the 3,590 studies identified, 28 (CLD only: 5, LT only: 18, both CLD and LT: 2; LT with third dose vaccine: 3) are included in the meta-analysis with 3,945 subjects. The characteristics of included studies are shown in Table 1 (for CLD patients and LT recipients receiving two doses of vaccine) and Supplementary Table 1 (for LT recipients receiving third dose). For CLD patients, the median age was 53.8 years (IQR, 43.0ŌĆō64.4 years), and 62.1% were male. For LT recipients, the median age was 63.0 years (IQR, 59.0ŌĆō65.6 years), and 64.0% were male. All studies scored at least six stars in NOS, indicating low to moderate risk of bias with satisfactory quality (Supplementary Table 1).
Meta-analysis for CLD patients
Humoral immune response
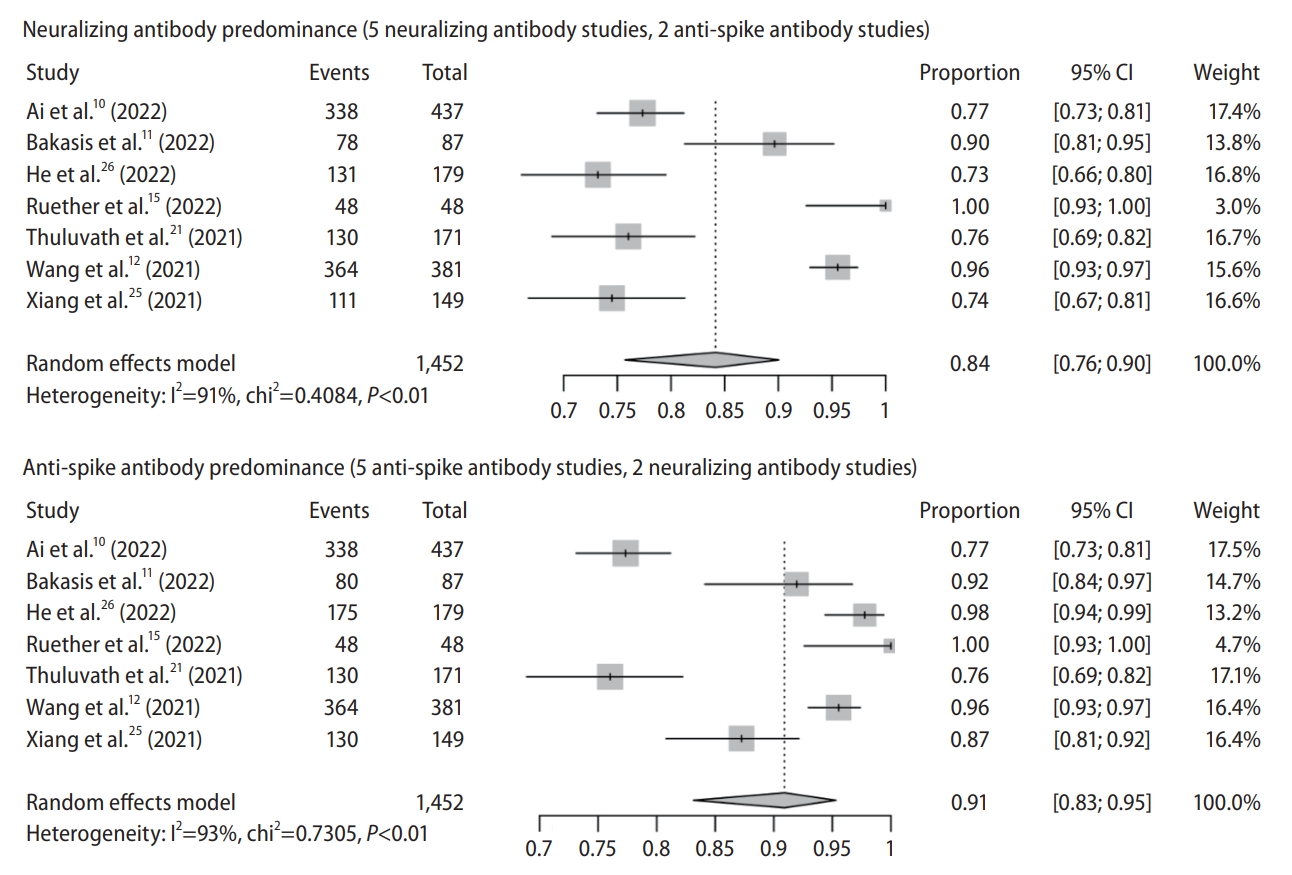
There are seven observational studies with 1,452 subjects (studies reporting both Nab and anti-spike antibody: 3; Nab only: 2; anti-spike antibody only: 2) (Table 1). In Nab predominance forest plot (Nab: 5; anti-spike antibody: 2), pooled seroconversion rate was 84% (95% CI, 76ŌĆō90%) with considerable heterogeneity among the studies (P<0.01; I2=91%) (Fig. 1). In anti-spike antibody predominance forest plot (anti-spike antibody: 5; Nab: 2), pooled seroconversion rate was 91% (95% CI, 83ŌĆō95%) with considerable hereogeneity (P<0.01; I2=93%) (Fig. 1).
The funnel plot appeared to be have some asymmetry for studies with either anti-spike antibody (P=0.038 by Egger test) or neutralizing antibody predominance (P=0.012 by Egger test), indicating publication bias (Supplementary Fig. 2). Trim and fill-method was used to adjust for publication bias, and the pooled seroconversion rate was 83% (95% CI, 71ŌĆō90%) for Nab predominance analysis and 82% (95% CI, 61ŌĆō93%) for anti-spike antibody predominance analysis.
Meta-regression analysis showed significant association between seroconversion of Nab and etiology of liver disease (P<0.001) and a trend for method of antibody test (P=0.053 for ECLIA vs. ELISA) but not other factors (Supplementary Fig. 3).
Antibody type
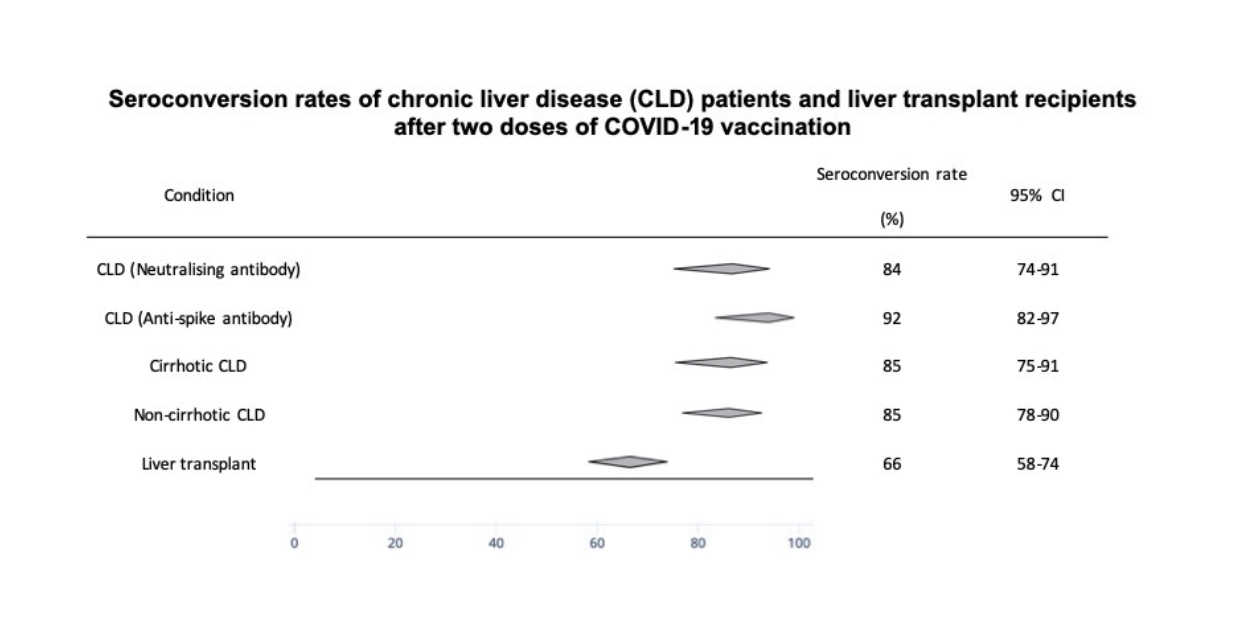
Pooled seroconversion rate of Nab and anti-spike antibody was 84% (95% CI, 74ŌĆō91%) and 92% (95% CI, 82ŌĆō97%), respectively (Fig. 2).
Method of antibody test
There were four studies on CLIA, two on ELISA and one on ECLIA. Seroconversion rate was 89% (95% CI, 77ŌĆō95%), 88% (95% CI, 82ŌĆō92%), 76% (95% CI, 69ŌĆō82%) in CLIA, ELISA and ECLIA, respectively (Supplementary Fig. 4).
Age
There were two studies with median age Ōēź60 years and five studies with median age <60 years. Seroconversion rate was 85% (95% CI, 64ŌĆō94%) and 88% (95% CI, 79ŌĆō93%) in the older and younger age group, respectively (Supplementary Fig. 5).
Etiology of liver disease and cirrhosis status
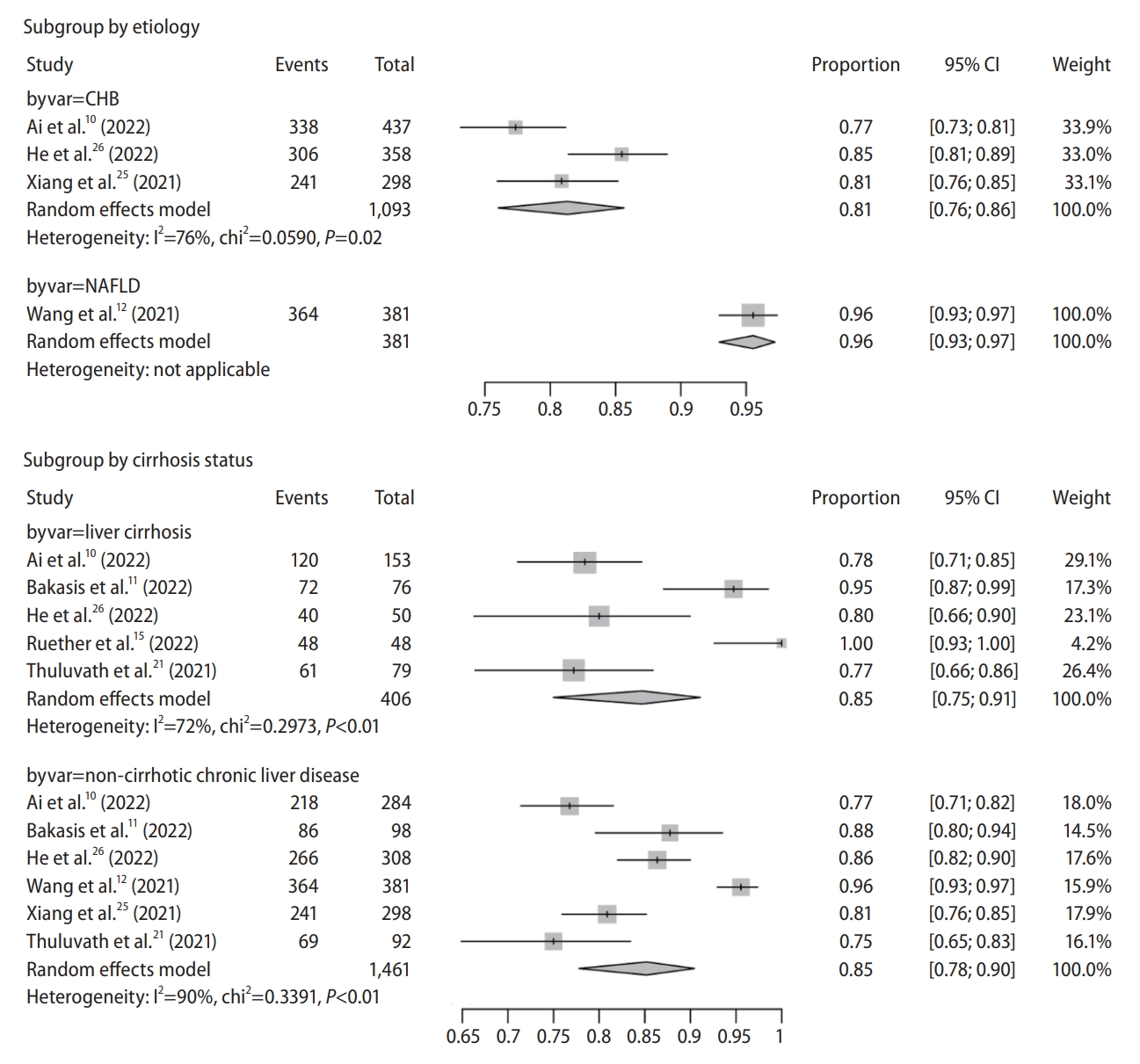
We used 80% as cut-off for classifying the major etiology of a study. There were three studies on chronic hepatitis B (CHB) infection (two studies with 100% CHB [25,26] and one with 87.9% [10]) and one study on non-alcoholic fatty liver disease (NAFLD) (Table 1) [12]. Other studies recruited a heterogeneous population of CLD patients of various etiologies without available individual data, and therefore were excluded from subgroup analysis. Seroconversion rate was 81% (95% CI, 76ŌĆō86%) and 96% (95% CI, 93ŌĆō97%) in CHB and NAFLD patients, respectively (Fig. 3).
There were five studies on cirrhosis and six studies on non-cirrhosis CLD, four of which reported both outcomes. Seroconversion rate was 85% (95% CI, 75ŌĆō91%) and 85% (95% CI, 78ŌĆō90%) in patients with cirrhosis and those without cirrhosis, respectively (Fig. 3). Only one study reported seroconversion rate regarding cirrhosis severity (compensated cirrhosis: 78.9%; decompensated cirrhosis: 76.7%) [10].
Vaccine platform
There were four studies on inactivated vaccine and three on mRNA vaccine. Seroconversion rate was 86% (95% CI, 78ŌĆō92%) and 89% (95% CI, 71ŌĆō96%) in inactivated and mRNA vaccine, respectively (Supplementary Fig. 6).
Individual vaccine type
We used 80% as cut-off for classifying vaccine type of a study. There were two studies using BNT162b2 [11,15] and one using BBIBP-CorV [12] with 516 subjects. Other studies recruited a heterogeneous population of patients with various vaccine types without available individual data, and therefore were excluded from subgroup analysis. Seroconversion rate was 95% (95% CI, 72ŌĆō99%) and 96% (95% CI, 93ŌĆō97%) in BNT162b2 and BBIBP-CorV subgroups, respectively (Supplementary Fig. 7).
Region
There were four studies from the East and three from the West. Seroconversion rate was 86% (95% CI, 78ŌĆō92%) and 89% (95% CI, 1ŌĆō96%) in the East and West subgroups, respectively (Supplementary Fig. 8).
Cell-mediated vaccine immunogenicity
Only one study reported T-cell immune response among cirrhosis patients [15]. A T cell response was observed in 65% of cirrhosis patients, 37% of LT recipients and 100% of control subjects, with a strong response being present in 46%, 32%, and 100% in the three groups, respectively.
Adverse events
There were five studies (inactivated vaccine: 4; mRNA vaccine: 1) reporting adverse events with 1,360 subjects. Prevalence of adverse events was 27% (95% CI, 18ŌĆō38%) with considerable heterogeneity (P<0.01; I2=88%) (Supplementary Fig. 9). Ai et al. [10] reported three subjects having grade 3 laboratory abnormalities with raised alanine transaminase five times above upper limit of normal, one of whom developed trend of acute liver failure requiring hospitalization (grade 4). Ruether et al. [15] reported two subjects with severe systemic side effects or requiring medications (grade 3) and one requiring hospitalization (grade 4). Supplementary Table 2 showed pooled prevalence of local and systemic adverse events among inactivated vaccine recipients. The most common local and systemic adverse event was pain (13%; 95% CI, 7ŌĆō23%) and fatigue (3%; 95% CI, 2ŌĆō5%), respectively. The study using mRNA vaccine did not report detailed data on individual adverse events.
Liver transplant recipients
Humoral immune response
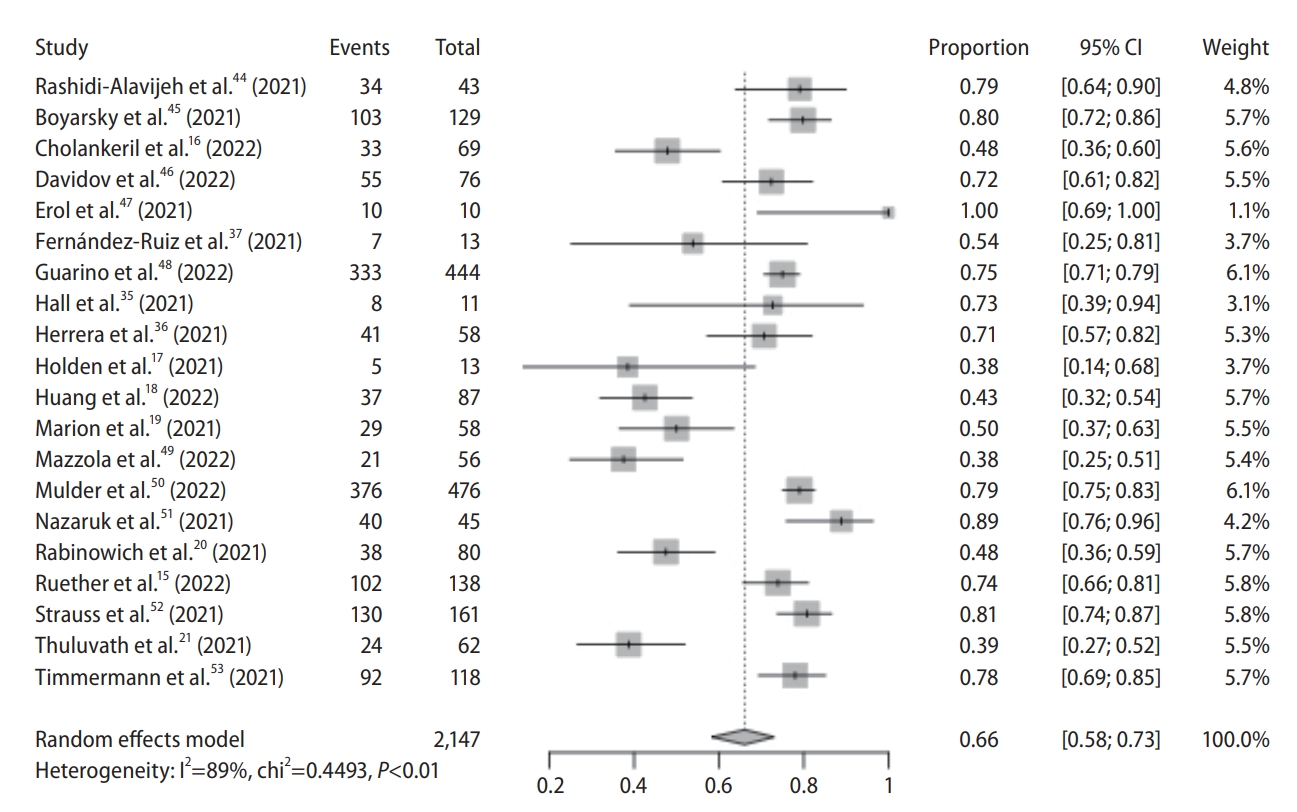
There were 20 observational studies with 2,147 subjects. All studies were conducted in the West. Pooled seroconversion rate was 66% (95% CI, 58ŌĆō73%) with considerable heterogeneity (P<0.01; I2=89%) (Fig. 4). The funnel plot appeared to be have some asymmetry (P=0.059 by Egger test), indicating publication bias (Supplementary Fig. 10). Trim and fill-method was used to adjust for publication bias, and the pooled seroconversion rate was 69% (95% CI, 61ŌĆō76%).
Meta-regression analysis showed a trend for association between seroconversion of Nab and age (P=0.085) and method of antibody test (P=0.066 for CLIA vs. ECLIA) but not other factors (Supplementary Fig. 11).
Subgroup analysis
Method of antibody test
There were nine studies on CLIA, seven on ELISA, and four on ECLIA. Seroconversion rate was 71% (95% CI, 61ŌĆō79%), 56% (95% CI, 43ŌĆō69%), 70% (95% CI, 47ŌĆō86%) in CLIA, ELISA and ECLIA, respectively (Supplementary Fig. 12).
Age
There were nine studies with median age Ōēź60 years and four studies with median age <60 years. A total of 1,826 subjects were included. Seroconversion rate was 64% (95% CI, 52ŌĆō74%) and 77% (95% CI, 70ŌĆō83%) in the older and younger age groups, respectively (Supplementary Fig. 13).
Individual vaccine type
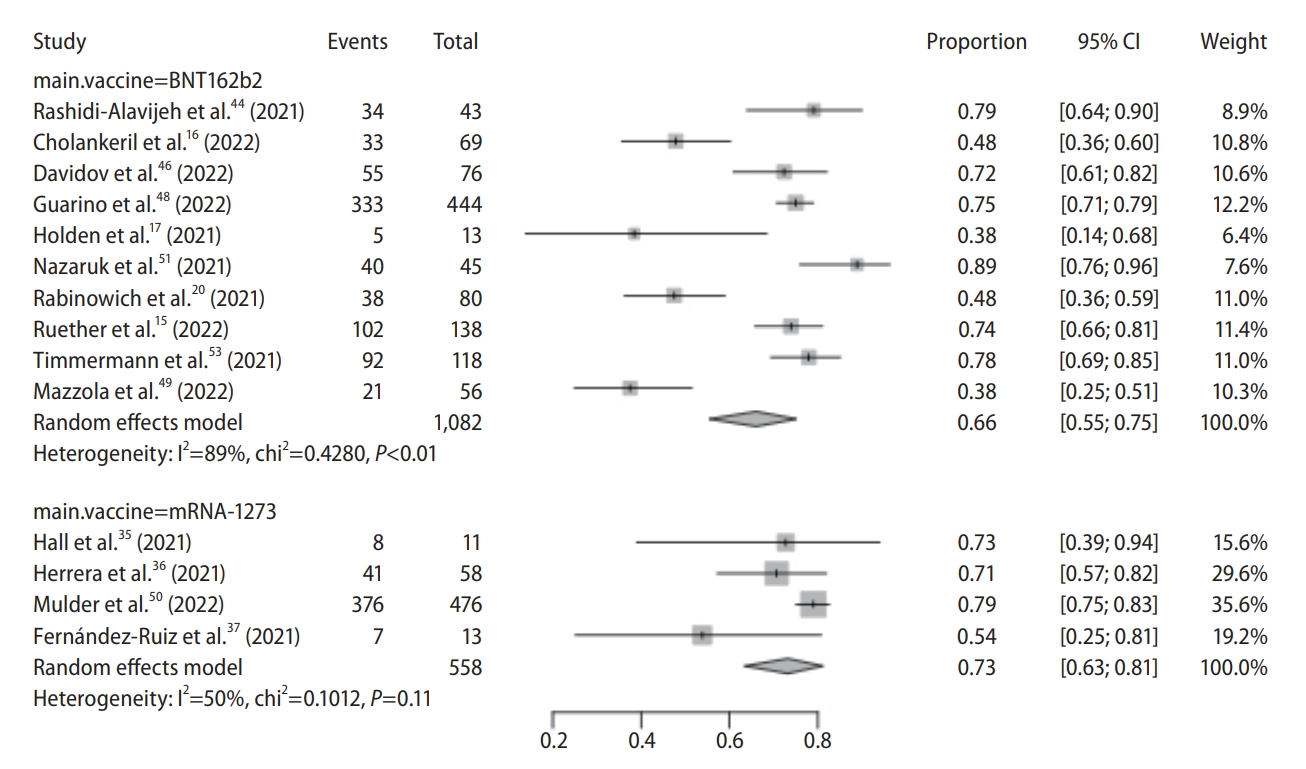
All studies used mRNA vaccines (BNT162b2: 10; mRNA-1273: 4) with 1,640 subjects. We used 80% as cut-off for classifying vaccine type of a study. Seroconversion rate was 66% (95% CI, 55ŌĆō75%) and 73% (95% CI, 63ŌĆō81%) in BNT162b2 and mRNA-1273 subgroups, respectively (Fig. 5).
Number of immunosuppressants
Four studies reported data on use of Ōēź2 immunosuppressants with 274 subjects. Seroconversion rate was 62% (95% CI, 43ŌĆō79%) (Supplementary Fig. 14).
Cell-mediated vaccine immunogenicity
Four studies reported cell-mediated immune response in 157 LT recipients. T cell response rate was 65% (95% CI, 30ŌĆō89%) with considerable heterogeneity (P<0.01; I2=90%) (Supplementary Fig. 15). Among those with negative humoral response in two studies, T cell response rate was 52% (95% CI, 12ŌĆō90%) (Supplementary Fig. 15).
Adverse events
Three studies reported adverse events with 251 subjects. Pooled prevalence of adverse events was 63% (95% CI, 39ŌĆō82%) with considerable heterogeneity (P<0.01; I2=92%) (Supplementary Fig. 16). Ruether et al. [15] reported 17 subjects with severe systemic side effects or requiring medications (grade 3) and one subject requiring hospitalization (grade 4). Data on individual adverse events were not reported in these studies.
Seroconversion rate among LT recipients receiving third dose
Three observational studies with 151 subjects were conducted in the West. Pooled seroconversion rate was 88% (95% CI, 58ŌĆō98%) with considerable heterogeneity (P<0.01; I2=83%) (Supplementary Fig. 17).
DISCUSSION
This is the first meta-analysis to report COVID-19 vaccine immunogenicity and reactogenicity among CLD patients and LT recipients. Overall seroconversion rate ranges between 84% (based predominantly on Nab) and 91% (based predominantly on anti-spike antibody) among CLD patients; similar immunogenicity is noted regardless of cirrhosis status. Seroconversion rate of anti-spike antibody is 68% after two doses and 88% after third dose among LT recipients.
CLD
CLD patients are at a higher risk of developing severe COVID-19 disease and acute decompensation [31] with mortality reaching 14% [31,32]. Owing to immune dysregulation, CLD patients had lower immunologic response rate to inactivated vaccines like influenza or hepatitis vaccines [33]. CLD and fibrosis hamper production of innate immunity proteins and pattern recognition receptors, and adversely influence B- and Tlymphocytes in terms of absolute counts and functions via various mechanisms. However, the pooled seroconversion rate is good, ranging from 84% to 91% in our meta-analysis. Notably, although seroconversion rate is similar among CLD patients compared with healthy controls, their titer is generally lower [11,15]. A lower seroconversion rate of Nab of 77% was noted in the study by Ai et al. [10] recruiting subjects (87.8% CHB) who received inactivated vaccines. Another study of CHB patients receiving inactivated vaccines also found a seroconversion rate of Nab at 64.0ŌĆō78.9%, dependent on HBV activity and cirrhosis status [26]. Our meta-analysis showed a numerical difference in seroconversion rate for CHB and NAFLD patients (81% vs. 96%). Nonetheless, a firm conclusion could not be drawn as there were only three studies on CHB (using three different inactivated vaccines) and one on NAFLD (using BBIBP-CorV only), and the difference could be due to different vaccine platforms used in each study. The seroconversion rate appears to be similar among younger and older subjects (85% vs. 88%).
There is also no difference in seroconversion rate between cirrhotic and non-cirrhotic groups (both 85%). There is only one study reporting no difference in vaccine immunogenicity as regards cirrhosis severity (compensated cirrhosis: 78.9%; decompensated cirrhosis: 76.7%) [10]. Subgroup analysis showed no difference in seroconversion rate between inactivated and mRNA vaccines.
Measuring anti-spike immunoglobulin G (IgG) or anti-RBD IgG results in a slightly higher seroconversion rate than Nab (91% vs. 84%). This difference is exemplified by one study showing seroconversion rate of 64.0ŌĆō78.9% for Nab (dependent on HBV replication and cirrhosis status) and 96ŌĆō100% for anti-spike IgG or anti-RBD IgG [26]. Nab level is a surrogate marker of vaccine effectiveness against symptomatic infection [22-24]. Anti-spike and anti-RBD IgG levels correlate with Nab [34] but not equate Nab. Using ECLIA to measure antibody level also results in slightly lower seroconversion rate compared with CLIA and ELISA (76% vs. 89% vs. 88%).
LT
Pooled seroconversion rate is less satisfactory (66%) among LT recipients, in particular for older than younger patients (64% vs. 77%). However, when compared with other organ transplant recipients (e.g., kidney, heart), LT recipients have higher seroconversion rate [19,35]. This may be related to stricter and higher levels of immunosuppression in other organ transplant recipients. However, all studies except one [35] reported seroconversion rate of anti-spike antibody but not Nab. Hall et al. [35] noted that 28.5% of organ transplant recipients with anti-RBD did not have Nab. Seroconversion rate of anti-spike IgG varied from 38% to 100%, likely related to variance in immunosuppression regimen. Known risk factors for seronegativity include high-dose steroid, triple immunosuppression, mycophenolate mofetil [20,36], low B-lymphocytes [15], hypogammaglobulinemia [36], vaccination during the first year post-transplantation [36], low estimated glomerular filtration rate [20], old age and alcohol-related liver disease [12]. Our meta-analysis showed that pooled seroconversion rate of patients receiving Ōēź2 immunosuppressants is slightly lower (62%) than that of whole cohort (66%). Subgroup analysis also shows the seroconversion rate of mRNA-1273 is slightly higher than that of BNT162b2 (73% vs. 66%). Importantly, pooled seroconversion rate increases to 88% after booster dose. Data on immunogenicity of inactivated vaccines in LT recipients are currently lacking. Notably, using ELISA to measure antibody level also results in slightly lower seroconversion rate compared with CLIA and ECLIA (56% vs. 71% vs. 70%).
There are four studies reporting T-cell immune response, with a pooled response rate of 65% [15,35-37]. Similar to the phenomenon observed in humoral response, level of T cell response is higher in LT recipients than other organ transplant recipients, e.g., heart transplant [36]. Our meta-analysis shows 52% have T-cell response despite seronegativity. Vaccine-induced T-cell response may offer protection via suppressing viral replication and supporting long-term memory of the immune system [38], hence protecting against severe infection despite seronegativity [23].
Concerning vaccine reactogenicity, pooled prevalence of adverse reactions is 27% among CLD patients receiving mainly inactivated vaccines, which is similar among healthy subjects (23% in a meta-analysis of randomized controlled trials) [39]. There is only one study reporting no significant difference in frequency of adverse events as regards cirrhosis status (non-cirrhosis: 15.5%; compensated cirrhosis: 16.3%; decompensated cirrhosis: 20.0%) [10]. As for LT recipients receiving mRNA vaccines, pooed prevalence of adverse reactions is 63%, compared with 48% among healthy subjects [39].
Our study findings support current international recommendation on COVID-19 vaccination in CLD patients and LT recipients [13,40]. LT recipients should receive vaccine platforms with more data (e.g., mRNA vaccine) and third-dose booster. Another strategy may be heterologous vaccination [41], in which seroconversion rate of 81.8% was reported for 8% of LT cohort who had heterologous vaccination in the study by Ruether et al. [15].
Limitations of the current study should be acknowledged. First, some studies did not measure Nab level, and the test kits differed among different studies. Second, the optimal antibody thresholds for protection is still unknown. Titers above the cut-off should protect against severe disease for the majority of vaccine recipients, but not against asymptomatic infection [23,42,43]. Third, only three studies reported vaccine immunogenicity among CHB patients and one on NAFLD; others recruited a heterogeneous population of CLD patients without available data for individual disease etiology (e.g., chronic viral hepatitis, NAFLD, autoimmune hepatitis) which may have different vaccine immunogenicity, in particular among autoimmune liver diseases which require immunosuppressants. Similarly, the LT recipients were comprised of a heterogeneous population of various disease etiology and different immunosuppressive regimen. Individual studies did not provide the seroconversion rate according to disease etiology and immunosuppressive regimen, and therefore subgroup analysis could not be performed according to these factors. Fourth, we did not include studies with general population that might enrol CLD recipients for comparison.
While an excellent safety profile is demonstrated in CLD and LT patients, the former group has good humoral response and the latter has lower response. Third-dose booster or heterologous vaccination may be considered in LT recipients, although more studies with larger sample size are warranted before this practice is widely recommended.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Supplement1
Supplement1 Print
Print





