


INTRODUCTION
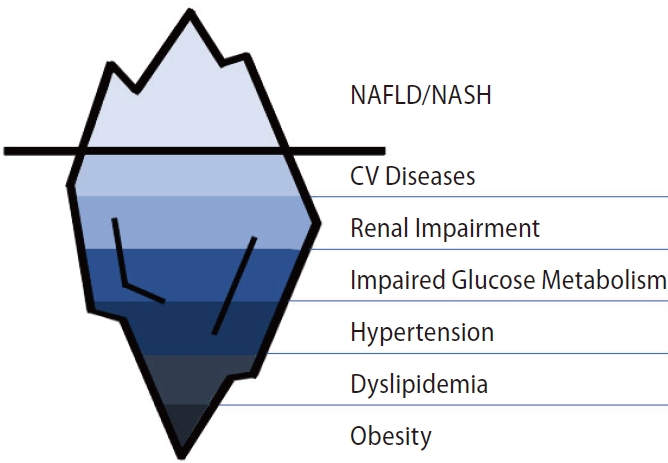
Non-alcoholic fatty liver disease (NAFLD) is currently the fastest growing indication to liver transplantation (LT) both in United States and Europe [1,2]. NAFLD is the hepatic expression of a systemic metabolic dysfunction. Indeed, NAFLD is commonly associated to cardiovascular (CV) disease, obesity, glucose impairment and dyslipidemia, which make more challenging the management of NAFLD patients in the transplant setting (Fig. 1). The term metabolic-associated fatty liver disease (MAFLD) was recently proposed to better characterize the metabolic dysfunction associated fatty liver disease [3], launching the debate on potential change in diagnosis, development of new therapies and improved clinical management.
MAFLD
MAFLD is defined by the evidence of hepatic steatosis (based on histologic, radiologic or blood test findings), associated with at least one of the following three criteria: overweight/obesity, type 2 diabetes mellitus (DM), and evidence of metabolic dysregulation [4]. Metabolic dysregulation is in turn defined by the presence of at least two of the following criteria: waist circumference Ōēź102/88 cm in Caucasian men/ women and Ōēź90/80 cm in Asian men/women; blood pressure Ōēź130/85 mmHg or the use of specific treatment, triglycerides Ōēź150 mg/dL or the use of specific treatment, high-density lipoprotein Ōēż40/50 mg/dL in men/women or the use of specific treatment, pre-diabetes, reactive C protein (RCP) Ōēź2 mg/dL and insulin resistance index (HOMA-IR) Ōēź2.5 [4]. The definition of MAFLD does not imply the absence of significant alcohol consumption or other causes of liver injury [4], but these patients should be defined as having dual etiology fatty liver disease [5]. The term MAFLD may improve patients characterization and help to identify individuals at higher risk for future adverse events and mortality. Indeed, Kim et al. [6] recently found a strong association between MAFLD and all-cause and cause-specific mortality, whereas NAFLD per se is not related to all-cause and cause-specific mortality. Specifically, patients who met the definition of MAFLD but not of NAFLD, had a 1.7-fold higher risk of all-cause mortality (hazard ratio [HR] 1.66; 95% confidence interval [CI] 1.19ŌĆō2.32; P=0.003) and a 24% higher CV mortality (HR 1.24; 95% CI 1.01ŌĆō1.51; P=0.041). Changing the nomenclature from NAFLD to MAFLD could focus on the metabolic underpinning and adjust the management of these patients, including in a transplant setting.
INDICATIONS TO LIVER TRANSPLANTATION IN PATIENT WITH NAFLD/NASH
Currently, approximately 25% of the global population is affected by NAFLD and up to 25% of these individuals have non-alcoholic steatohepatitis (NASH) [7], with an alarming growth of incidence in young population [8]. The estimated incidence of NAFLD and NASH in 2030 are 101 million and 27 million, respectively. A recent analysis reported an increment trend of 168% for decompensated cirrhosis, 178% for liver-related death and 137% for hepatocellular carcinoma (HCC), between 2015 and 2030 [9]. Similarly, a modelling study predicted an increased rate of HCC cases of 117% in France and 88% in UK [9]. LT is the only lifesaving approach for NASH-related end stage liver disease (ESLD) and non-resectable HCC [10]. It is therefore not surprising that NAFLD is rapidly growing as indication for LT and is currently the second leading cause for LT in USA, accounting for 21.5% of performed transplants in adults during 2018 [1]. An exponential growth has also been seen in Europe, going from 1.2% in 2002 to 8.4% in 2016 [2]. Patients transplanted for NASH have more frequently HCC than non-NASH patients, 39.1% vs. 28.9% respectively (P<0.001), are older (median: 60 vs. 55 years, P<0.001) and with higher body mass index (BMI) (mean: 32.6 vs. 25.8 kg/m2, P<0.001) [11]. The reason why HCC seems to be more prevalent as indication to LT in NASH than in non-NASH patients has not yet been thoroughly understood. Proposed mechanisms include the presence of a chronic systemic inflammatory environment, genetic polymorphisms as PNPLA3 and TM6SF2, greater iron absorption, gut dysbiosis, increased lipid storage with lipotoxicity, insulin resistance and higher insulin-like growth factor (IGF) levels [12,13]. In addition, NASH patients are often obese, thus making more difficult to perform ultrasound screening of HCC.
Notably, a significant proportion of HCC in patients with NAFLD/NASH may arise in a non-cirrhotic liver. In an Italian multicenter study on 756 patients with HCC, Piscaglia et al. [14] showed that 46.2% of NAFLD-HCC occurred in a pre-cirrhotic liver. Similar results have been reported by independent cohort in Germany and Japan (41.7% and 49%, respectively) [15,16].
ACUTE ON CHRONIC LIVER FAILURE
Acute on chronic liver failure (ACLF) is defined as an ŌĆ£Acute decompensation of cirrhosis (ascites, hepatic encefalopathy [HE], gastrointestinal [GI] bleed and/or infection) associated with organ failure (OF) and high 28-day mortality (>15%)ŌĆØ [17,18]. In a recent study based on National Inpatient Sample (NIS) database, Axley et al. [19] showed that NASH cirrhosis is the most rapidly growing etiology causing hospital admission for ACLF, with an increase of 63%, from 3.5% in 2006ŌĆō2008 to 5.7% in 2012ŌĆō2014 (P<0.001). In this series, infection was the most common precipitating event in ACLF (80%). Compared with non-NASH ACLF, these patients required a longer hospitalization though inpatient mortality was lower. A retrospective study based on the Veteran Health estimated an incidence of ACLF (based on European Association for the Study of the Liver - chronic liver failure criteria [EASL-CLIF] criteria) among NASH cirrhosis patients of 3.4/1,000 (95% CI, 2.9ŌĆō4.0), confirming bacterial infections as the most common precipitant factor. Among individuals with ACLF grade 3, in NASH patients, kidney failure was the most common organ failure, although NASH and hepatitis C etiology shared the highest rates of circulatory failure [20]. Growing evidence suggests that patients with ACLF grade 3 should be evaluated for LT and may achieve an excellent outcome after transplant [21], provided that they are appropriately selected [22]. Pre-transplant evaluation is important in NAFLD/NASH patients due to their increased CV and systemic risk. Importantly, NASH was not associated to an increased risk of post-transplant mortality in patients undergoing transplantation for ACLF [21,22].
PRE-TRANSPLANT EVALUATION
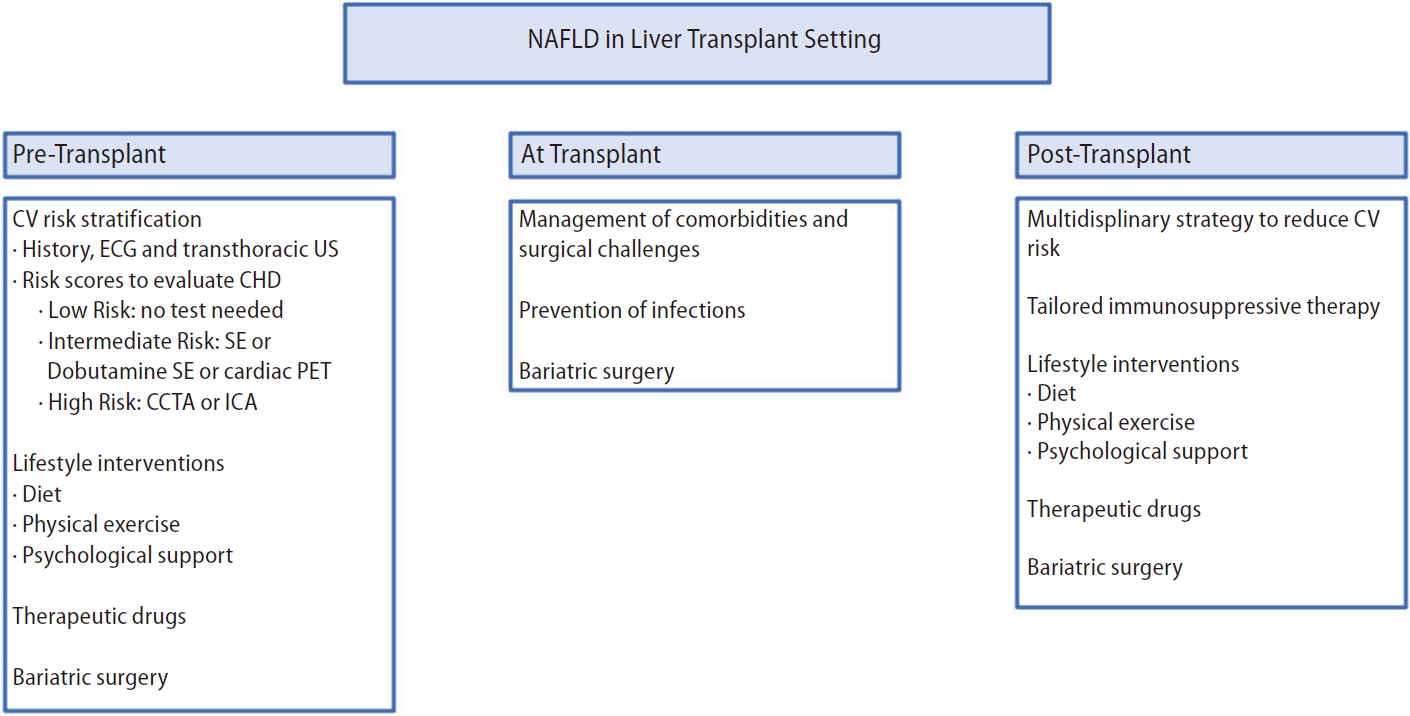
Metabolic syndrome, DM, and CV diseases that are often present in patients with NASH should be considered at time of LT evaluation, as they are important causes of death after LT and may be an absolute or relative contraindication to transplantation (Fig. 2) [23]. The CV issues in patients with NASH may act synergistically with the cardiac alterations associated with cirrhosis (e.g., cirrhotic cardiomyopathy, prolonged QTc) [24]. Adequate risk stratification of coronary artery disease (CAD) is essential to improve post-transplant survival. CAD is present in approximately 25% [25] of LT candidates, and patients with NASH or renal dysfunction are more likely to have a higher burden of CAD and critical coronary artery stenosis [26,27]. Worldwide, there is considerable variability in how LT programs assess cardiac risk, as models used to predict cardiovascular risk in the general population have not been validated in patients with liver disease. Regardless of the risk stratification approach used, a dedicated cardiology and anesthesia team must be involved in selecting candidates for LT [28]. As a first approach, it is necessary to obtain a medical history and search for the presence of CAD risk factors to determine the need for screening and the choice of the type of investigations. Traditional CV risk factors: male sex, hypertension, hyperlipidemia, smoking, age >60 years, left ventricular hypertrophy, previous CV disease or diabetes have been identified as the main risk factors associated with significant coronary artery stenosis in LT candidates [29,30]. So far, only three clinical risk scores have been proposed to stratify cardiac risk in LT candidates:
┬Ę CArdiovascular Risk in Orthotopic Liver Transplantation (CAR-OLT) [31]: a prognostic model designed to predict the overall 1-year risk of death or hospitalization for a significant CV event; however, it has not yet received external validation and does not estimate long-term CV risk.
┬Ę Cardiac arrest risk index [32]: a point-based model to predict cardiac arrest and ventricular arrhythmias within 30 days after transplantation.
┬Ę CAD-LT (coronary artery disease in liver transplantation) [33]: effectively stratifies pre-LT risk for significant CAD and thus can guide more targeted evaluation of candidates with less number of tests and faster waiting list inclusion.
Troponin-I and RCP, appear to have high sensitivity in predicting cardiac risk in liver transplant candidates, but more studies are needed before they can be used in clinical practice [34,35]. Current studies have revealed that coronary artery calcium scoring has a negative predictive value of 95ŌĆō100% for significant coronary heart disease (CHD) [36,37]. Therefore, the most recent American Society of Transplantation guidelines proposed its use in the risk stratification of LT candidates [23]. Non-invasive stress testing (e.g., dobutamine stress echocardiography, myocardial perfusion imaging and CV magnetic resonance) have been validated to detect CAD in general but are suboptimal for patients with ESLD [28]. According to the current European Society of Cardiology [38] guidelines, non-invasive testing should be offered to patients with more than two risk factors for CAD and poor functional status. Invasive coronary angiography is the gold-standard test to identify significant CHD in the general population, but currently, in LT candidates, studies are inconclusive and not able to predict the impact of asymptomatic pre-LT CV abnormalities on long-term outcomes [39,40]. Coronary computed tomography angiography (CCTA) is a non-invasive test valid for assessing the risk of CHD in LT candidates, although no studies are comparing it with invasive coronary angiography (ICA) in this population [41]. CCTA alone does not provide a functional assessment of coronary stenosis, which can be obtained by integrating this examination with fractional flow reserve obtained from computed tomography in this population [42].
The most recent guidelines, published in October 2022 by the American Transplant Society [28], recommend the following algorithm:
┬Ę Cardiac physical examination, electrocardiogram (ECG), and resting trans-thoracic echocardiography (TTE) (with measurement of myocardial strain and bubble study to assess pulmonary hypertension and intracardiac and extracardiac leads) for all LT candidates without CHD.
┬Ę In LT candidates at low risk of significant CHD (age <40 years, able to achieve Ōēź4 metabolic equivalents (METs), no NASH or diabetes, no CHD risk factors), if initial ECG and resting TTE are normal, additional cardiac stress testing may not be necessary.
┬Ę In intermediate-risk liver transplant candidates, non-invasive exercise testing may be considered (stress echocardiography [SE] is preferred; dobutamine SE if patient cannot exercise. Positron emission tomography as an alternative if available).
In LT candidates at high risk of significant CHD (diabetes, NASH, or Ōēź2 other CHD risk factors), coronary anatomic imaging (CCTA or ICA) is mandatory.
┬Ę ICA should be the last procedure performed in the evaluation before listing for liver transplantation after the patient has already been considered an acceptable transplant candidate.
Lifestyle modifications are recommended to improve clinical outcomes after transplantation. Obese patients should lose weight through a low-calorie diet and adequate physical activity [23]. Weight loss in this patient population must be carefully controlled and managed by experts to avoid loss of muscle mass and subsequent sarcopenia, which is a known risk factor that increases post-transplant mortality and worsens patient prognosis (Table 1) [43,44].
WAITING-LIST MANAGEMENT
A recent analysis on patients from OPTN (Organ Procurement and Transplantation Network)/UNOS (United Network for Organ Sharing) registry showed that, in comparison to patients with alcoholic liver disease (ALD), the risk of 90-day and 1-year waitlist mortality was significantly higher in NASH patients (P=0.042 and P=0.008) [45]. Model for End-Stage Liver Disease-Na (MELD-Na) score, Chronic Kidney Disease (CKD) stage >3 and hyponatremia were significantly associated to mortality. Nagai and colleagues also demonstrated that 90- day Delta MELD-Na was lower in Alcoholic Liver Disease (ALD) patients than in NASH patients, suggesting that NASH patients may have a faster disease progression. When considering patients with HCC as indication to LT, NASH patients showed a higher risk of 1-year waitlist mortality compared to HCC-ALD; however, an explanation could be that NASH patient were older [45]. Another study based on UNOS registry data from 2002 to 2016 found a higher unadjusted cumulative incidence of exclusion from wait list (WL) for mortality and deterioration in NAFLD patients compared to patients with other indications to LT, but when adjusted for confounder factors, waitlist mortality was similar between NASH and non-NASH patients [46]. In fact, by analyzing data from the Scientific Registry of Transplant Recipients (SRTR) from 2002 to 2016, Younossi et al. [47] found no significative difference in terms of outcome during the waiting-list (transplant vs. drop out) between different etiologies. Young et al. [48] demonstrated that patients with NASH-HCC are less likely to have exception to MELD on WL and, as a result, they are less likely to receive LT than patients waitlisted for other etiologies. Another factor that may contribute to disparities in HCC exception is the better hepatic function in NASH-HCC patients at diagnosis and the slower progression of cirrhosis compared with Hepatitis C Virus (HCV)-HCC patients [48], which results in lower MELD score. As a consequence, NASH-HCC patients have significantly higher rates of primary surgical resection and lower rates of LT when compared with HCV-HCC patients [49], leading to lower likelihoods to receive LT and longer WL times. Furthermore, NASH patientsŌĆöincluding those with a low MELD score, were more frequently delisted or died due to CV complications. It thus seems that the MELD score does not fully represent the clinical condition of NASH patients. New prognostic scores to better stratify the risk of short-term deterioration and mortality of patients with NASH are expected.
POST-TRANSPLANT MANAGEMENT
Early complications
It is estimated that about 40% of all deaths occurring in the first 30 days post-transplant are due to CV complications. Transplant operation is technically more challenging in obese patients; this is reflected by increased operative time, major operative transfusion requirements, increased surgical complications, such us hepatic arterial injury or malposition, inferior vena cava injury and uncontrolled bleeding, and higher rate of operative revision [50]. Consequently, obesity and diabetes mellitus together increased the 30-day risk of post-surgery complications, such as wound infections, sepsis, renal failure, and prolonged mechanical ventilation with extent of hospital stay [51-53]. NASH patients have more short-term mild complications, such as persisting ascites, pleural effusion, dyspnea, fever, electrolyte disturbance, abnormal liver enzymes or wound infections, while moderate severe complications were not significantly different between NASH and non-NASH patients. Mortality and graft survival at 90-days after LT were similar with patients transplanted for non-NASH cirrhosis [54]. Therefore, although the higher percentage of early complications, short-term graft and patient outcomes between NASH and non-NASH patients are comparable.
Late complications
Diabetes, hypertension, dyslipidemia, renal impairment and NASH have a key role as risk factors for the development of CV events after LT (Table 1) [55]. In particular, NASH patients have a higher mortality rate for cardio- and cerebro-vascular complications than non-NASH patients and such difference is particularly significant during the first year after LT [45]. Recently, a Spanish Group showed that the introduction of a post-transplant multidisciplinary approach achieved by a multiprofessional team, including the figures of hepatologist, endocrinologist and advanced practice nurses, decreased the incidence of CV events from 14% to 6%, acting on prevention and early detection of CV risk factors [56].
Diabetes mellitus
Prevalence of diabetes mellitus in NAFLD prior to LT is between 33% and 66% [57]. Male gender, ethnicity, family history, older age, BMI >30 kg/m2, HCV infection, and the use of immunosuppressive (IS) drugs, tacrolimus and corticosteroids, are risk factors for the development of post-transplant diabetes [58,59]. The gold standard for the diagnosis of diabetes after LT is the oral glucose tolerance test, whereas glycated haemoglobin might be used for monitoring, keeping in mind that in liver disease patients it could be falsely low due to anemia and splenomegaly. Diabetes Mellitus (DM) severely influences the prognosis of transplanted patients leading to higher 10-years mortality, increased CV events and greater infections rate [60,61].
At present there is no specific therapeutical indications for DM in LT recipients. A first step in the management of post-LT diabetes is modification of immunosuppression treatment [62]. Metformin is the most used treatment in general population with DM and could be safely prescribed as first line treatment in transplanted recipients with Estimated Glomerular Filtration Rate (eGFR) >30 mL/min, with no drug interaction with calcineurin inhibitors (CNIs) [63]. Promising results are expecting from the new antidiabetic drugs, such as agonist of GLP-1 receptor and SGLT2 inhibitors, which both have not only cardioprotective and nephroprotective benefits, but also effects on weight loss [64,65]. However specific interactions with immunosuppressive drugs need to be further investigated.
Dyslipidemia
Lipid metabolism impairment has a post-LT prevalence between 45% and 71%. Risk factors for the development of dyslipidemia are IS therapy, diabetes, high BMI, and individual predisposition [66]. Dyslipidemia after LT seems not to respond to life-style changing and is associated with a higher need of pharmacological therapy than in the pre-transplant setting [24]. Among statins, the hydrophilic ones should be preferred as they are not metabolized by cytochrome P 450-3A4 [67], thus not interfering with IS drugs. Pravastatin has not interaction with CNIs and it is the most used in the setting of LT. Ezetimibe in monotherapy is not useful but it could have a potential role in association with statins [68]. Fish oil are preferred to fibrates for the treatment of isolated hypertriglyceridemia [69].
Obesity
There is an increased prevalence of obesity both in transplant candidates and recipients. Patients, especially NASH ones, should be counseled before and after LT regarding consequences of obesity. Low diet, lifestyle modifications, and physical activity are mandatory especially after LT [70,71]. However, they are not always successful to prevent further increase in body weight as reported by Diwan et al. [72] who showed superiority of sleeve gastrectomy vs. dietary intervention in total body weight loss after LT. Among techniques, sleeve gastrectomy is always preferred over the Roux-en-Y gastric bypass for multiple reasons, firstly because it guarantees endoscopic access to the biliary system for the treatment of eventual post-transplant biliary strictures and secondly for malabsorption concern [24,73]. However, there is not consensus about which is the best time for bariatric surgery (BS), if before, simultaneously or after LT. The Mayo Clinic experience found that BS in contemporary with LT is a safe option, however restricted selection criteria of patients are mandatory [72,73]. Small case series are reported about BS after LT, some with complications due to peritoneal adhesions [74,75]. Further studies should be focused on new endoscopic bariatric techniques that are undoubtedly less invasive and are showing promising results in patients with NAFLD [76].
Cardiovascular events
CV disease is the most common extrahepatic cause of death in transplant recipients, independently from the underlying etiology, with a cumulative incidence of up to 30.3% within 8 years from LT [34]. Over the past decade, the increasing transplant indication for NASH and the older age of LT candidates, combined with the known metabolic effects of IS drugs, have contributed to the increased risk of CV disease in LT recipients. Patients transplanted for NASH have higher risk of dying from CV complications than patients transplanted for other reasons [77]. A recent study reported that the CV event rate 5 years after LT was approximately 40% in NASH patients and only 5ŌĆō10% in non-NASH recipients [78]. This finding was not confirmed by a meta-analysis of 119,327 patients, that, surprisingly, showed no difference in complications rates between NASH and non-NASH patients [79]. Interestingly, no differences in overall survival and graft survival were observed between the two groups in either study [78,79]. In clinical practice, the Prospective Cardiovascular M├╝nster Score (PROCAM) [80] and the Systematic Coronary Risk Evaluation Project (SCORE) [81] may be useful for rapid risk stratification of CHD after LT, but validated scores for predicting heart failure are not available. The first step in reducing the rate of cardiac events is to prevent and treat the CV risk factors, namely: diabetes, dyslipidemia, arterial hypertension, obesity, tobacco use and renal impairment. In patients with known cardiac disease prior to transplantation, monthly cardiac physical evaluation and B-Type Natriuretic Peptide (BNP) testing may be considered. Studies on the exact timing for echocardiography screening after LT are lacking; annual and semiannual screening in low- and high-risk patients, respectively, might be appropriate. In patients with severe CHD before LT, the use of statins may result in a survival benefit (HR 0.25; 95% CI 0.12ŌĆō0.49; P<0.001) [39]. Aspirin should be considered for secondary prophylaxis, whereas there is no evidence for its use in primary prevention [77]. In LT recipients with systolic dysfunction, as in the general population, anti-remodeling therapy, such as ACE inhibitors (ACEi), angiotensin receptor blockers (ARB), aldosterone antagonists, angiotensin receptor-neprilysin inhibitors (ARNI) and b-adrenergic receptor blockers (BB), may improve ejection fraction and relieve heart failure symptoms. However, they have no effect on diastolic dysfunction [82]. A case by case multidisciplinary team discussion, which includes hepatologist, surgeon, cardiologist, interventional cardiologist and anesthesiologist, is required to properly assess the individual CV risk after liver transplantation and to successfully prevent and treat CV events. A strict collaboration with primary care physician, dietician, psychologist and transplant hepatologist is advisable after liver transplantation to prevent weight gain, improve physical function and ameliorate adherence to lifestyle changes, thus reducing modifiable CV risk factors.
Arterial hypertension
Seventy per cent of patients after LT are affected by arterial hypertension [83]. As previously mentioned for diabetes, CNIs sparing strategy should be always adopted to prevent and further reduce blood pressure when hypertension occurs. Calcium channel blockers (AST to Platelet Ratio Index [APRI], Fibrosis-4 [FIB-4]), are the first line treatment due their effect on arterial renal vasodilatation opposed to the mechanism of CNIs and reducing systemic vascular resistance [63]. Beta-blockers could be used as a second line option [63]. ACE-inhibitors should be not used in the first period after LT due to the risk of hyperkalemia and metabolic acidosis, but they should be considered in patients with concomitant chronic kidney disease and diabetes mellitus [63].
Renal impairment
NAFLD/NASH transplanted patients are particularly at risk of developing renal impairment because of their frequent comorbidities (hypertension, diabetes, and obesity) associated to the well-known risk due to the use of CNI-based immunosuppression regimen. There are not precise guidelines for the treatment of renal disease after liver transplantation, however the efforts should be directed to the prevention and treatment of metabolic dysfunction and tailoring of IS therapy.
Recurrent NASH
In patients transplanted for NASH, post-transplant features of hepatic steatosis are present in up to 78ŌĆō88% of cases [78,84], while NASH is less common, ranging from 4% to 41% [84]. Risk factors for the development of post-transplant NAFLD are similar to the pre-transplant setting, which include obesity, hypertension, and diabetes [85]. Patients usually develop recurrent NAFLD/NASH in the first 5 years after liver transplantation [86]. Once NASH occurs, 11ŌĆō14% patients may develop cirrhosis within 5 years after LT [87]. Liver biopsy is the gold standard for the diagnosis of NAFLD/NASH. Less invasive techniques, such as magnetic resonance imaging (MRI), controlled attenuation parameter (CAP), magnetic resonance proton density fat fraction, serologic methods (AST to Platelet Ratio Index [APRI], Fibrosis-4 [FIB-4]), transient elastography, and magnetic resonance elastography, have been proposed but require validation [88]. Current guidelines are not specific for the management of recurrent NAFLD/NASH after liver transplantation. The first therapeutic approach should include weight loss and dietician counselling. Regarding medical therapy, there are no drugs that can be recommended in post-LT setting, since clinical trials did not include transplanted patients. In pre-transplant population, obeticholic acid, a FXR agonist, has been associated to histological improvement [89,90]; the same effect has been proved with Pioglitazone, that also reduces the chronic inflammatory environment [91]. Aramchol, a lipogenesis inhibitor, and liraglutide, a GLP1-receptor agonist, have been associated to a reduction in liver fat and steatohepatitis [92,93]. GLP1-receptor agonists and orlistat may also have a role in reducing NAFLD/NASH fibrosis [94]. Further data in recurrent NASH are awaited.
MANAGEMENT OF IMMUNOSUPPRESSION AND RISK OF REJECTION
IS treatment constitutes one of the most critical factors impacting outcomes after liver transplantation. The introduction of CNIsŌĆöcyclosporine (CsA) and tacrolimus (TAC)ŌĆöreported a reduction in acute rejection rates and improvements in short-term patient and graft survival [95]. Long-term survival, in contrast, is most impacted by renal, CV, and metabolic toxicity secondary to medication use, especially CNIs and glucocorticoids [96-98], in particular in predisposed patients such as those undergoing LT for NASH. The goal of the worldŌĆÖs LT experts is to reduce the toxicity of immunosuppression by tailoring therapy basing on individual patient characteristics. Steroids are obesogenic drugs that induce glucose intolerance, hypertension and hyperlipidemia. Their clinical use is short-lived in clinical practice, which limits their potential collectivizing effects. CNIs are associated with developing all components of the metabolic syndrome as a consequence of the inhibition of insulin secretion and increased insulin resistance. They, therefore, present a pro-diabetogenic action, more associated with TAC than with CsA, which, on the other hand, presents a more significant pro-lipidemic effect. The nephrotoxic effect of CNIs is also known to occur due to renal and systemic vasoconstriction mediated by this family of drugs, which is responsible for the onset of arterial hypertension. In patients transplanted for NASH, the strategy should be to early reduce or withdraw the steroids [24], introducing alternative immunosuppressive drugs with a lower impact on the metabolic profile. From OPTN/SRTR 2019 Annual Data Report, it was found that 75% of patients were treated with the dual regimen consisting of CsA and mycophenolate mofetil (MMF), and the MMF was reported to be used in 45% as maintenance therapy at 1- and 2-years after LT [95]. Patients treated with MMF combined with reduceddoses of CNIs had lower CV risk and reduced renal function impairment than those treated with a regimen containing only standard-dose of tacrolimus plus corticosteroids [99]. However, there still needs to be a consensus on the ideal minimization regimen. Newer mammalian target of rapamycin (mTOR) inhibitors [100] are associated with an increased risk of post-LT dyslipidemia, whereas they are neutral concerning diabetes mellitus and hypertension. Moreover they are associated with a reduction in body weight, a lower frequency of cardiac events and, compared with CNIs, are associated with a more favorable renal profile [24]. mTOR inhibitors, combined with CNIs, are associated to a prolonged long-term survival in patients transplanted for HCC [101]. In NASH patients, the use of drugs with less impact on the metabolic-cardiovascular profile, being the only modifiable factor, is the best strategy to reduce post-LT complications and improve outcomes.
SARCOPENIA
Up to 20% of NASH patients are estimated to be affected by sarcopenia [102]. A synergic overlap between pathophysiology of these two conditions resulted in an increased risk of NAFLD development when sarcopenia is present and vice versa [103,104]. Pre-LT sarcopenia has been associated with increased risk of adverse outcomes after liver transplantation, such as higher risk of bacterial infection and mortality [105]. Specific data regarding sarcopenia and NASH are still needed, however patients affected by sarcopenia and NASH are found to have an increased risk of insulin resistance, atherosclerosis and CV disease [103,106]. Metabolic alterations associated with cirrhosis may reverse after liver transplantation; however, few data on the assessment of body composition after LT are available. In 2013, Tsien et al. [107] investigated the potential role of post-transplant sarcopenia evaluating changes in body mass composition in prospective cohort of transplanted patients. Among 53 Patients (7.5% affected by NASH disease), 41 (77%) experienced a decreased in abdominal wall muscles and 43% an increase in fat area in a medium follow-up of 19.3┬▒9 months. However only patients who experienced post-transplant sarcopenia had 3.1-fold increased risk of developing DM (P=0.05, 95% CI 1.01ŌĆō9.38), with no evidence in decreased overall survival [107]. A review published in 2013 showed that, despite conflicting and few data with different methods of muscle mass assessment, further reduction of skeletal muscle mass has been observed up to one year after liver transplantation [108]. Possible explanations have been proposed including persistence of hypermetabolism soon after LT, IS drugs, mostly mammalian target of rapamycin (mTOR) inhibitors and corticosteroids, length of hospitalization and occurrence of post-transplant infections that tend to be more frequent in patients with pre-LT sarcopenia resulting in an increased risk of muscle mass depletion [105,109,110]. Subsequently, Jeon et al. [111] in retrospective cohort of 145 patients who underwent LT reported that all patients with pretransplant sarcopenia remain sarcopenic soon after LT and 15% of patients with normal muscle mass pre-transplant developed sarcopenia de novo post-LT. Although there was an increased trend of mortality soon after LT in newly developed sarcopenia, these finding were not confirmed at 6 months from LT, when sarcopenia resulted not to be a predictor of death [111]. Similar findings have been reported by Bhanji et al. [112] who assessed the skeletal muscle mass in two hundred and ninety-three patients 7 month after LT (interquartile range 4.8ŌĆō12 months). Ninety-eight patients (61%) resulted to be affected by post-LT sarcopenia, both with newly developed sarcopenia (25/98) and persistent sarcopenia (73/98). There was no difference in survival between post-LT sarcopenic patients (both de novo and persistent) and non-sarcopenic patients. It has been postulated that patients with post-LT sarcopenia resulted to be less affected by metabolic liver disease before LT (2.7% vs. 12.2% P=0.002). However, in contrast with these findings, Carias et al. [113], which retrospectively evaluated changing on body composition after LT in a cohort of 207 adult patients (21.7% with NASH), found that, at multivariate logistic regression analysis, NASH etiology is an independent predictor of sarcopenic obesity development (P=0.014; 95% CI: 1.44ŌĆō25.26, OR 6.03). Sarcopenic obesity (SO) is defined as the contemporary presence of sarcopenia in the contest of obesity [114]. The prevalence of SO in the context of cirrhosis ranges between 20% and 35% [115]. At present, studies on SO are limited and mostly focused on pre-transplant period, but a meta-analysis on the role of SO in liver transplantation reported an increased risk of death at least two times higher in SO vs. not SO patients both at short-and long-term follow-up [116]. Indeed the original aim of the meta-analysis was to assess the role of SO in patients with NASH after LT, but Hegyi et al. [116] were not able to perform the analysis due to lack of data. Data about the impact of post-LT sarcopenia continues to be scarce as recently highlighted by a review of Ooi et al. [105] who showed that upon 35 studies on sarcopenia in the setting of liver transplantation only 6 focused on the potential role of sarcopenia and SO after LT. Further data are needed on body compositionŌĆÖs changes in post-transplant period to ensure better management of these patients in order to guarantee better outcomes.
SURVIVAL AFTER TRANSPLANTATION
Liver transplantation represents the only life-saving therapy in patients with ESLD. In an analysis by Haldar et al. [11] on data from the European Liver Transplant Registry (ELTR) of patients transplanted between January 2002 and December 2016, NASH was not an independent predictor of patient or graft survival. However, older recipient age (61ŌĆō65 years: HR 2.07; 95% CI 1.39ŌĆō3.08; >65 years: HR 1.72; 95% CI 1.10ŌĆō2.71; relative to Ōēż45 years), MELD score >23 (HR 1.48; 95% CI 1.04ŌĆō 2.30; relative to Ōēż11) and BMI either Ōēż18.5 kg/m2 (HR 4.29; 95% CI 1.01ŌĆō18.21; 18.5ŌĆō25 kg/m2 : HR 2.24; 95% CI 1.27ŌĆō3.96) or >40 kg/m2 (HR 1.96; 95% CI 1.16ŌĆō3.32; relative to 25ŌĆō30 kg/m2) were independent predictors of post-LT mortality. A systematic review with meta-analysis [117] evaluated the variables associated with patient and graft survival in individuals with NASH-related liver disease, showing that recipient age >65 years, pre-transplant DM, MELD >23, functional status, HCC, dialysis prior to LT, hepatic encephalopathy and time/year of LT were predictors of mortality after transplantation. As previously described in patients transplanted for other etiologies of ESLD, increased patient mortality was associated with older age of the recipient (HR=2.07, 95% CI: 1.71ŌĆō2.50, I2=0, Žä2=0, P=0.40) and pre-transplant DM (HR=1.18, CI 95%: 1.08ŌĆō1.28, I2=0, Žä2=0, P=0.76). No difference in term of patient and graft survival rates were found between NAFLD/NASH and non-NAFLD/NASH patients transplanted for HCC [11]. Likewise, post-transplant HCC recurrence rates have been shown to be similar between NASH and non-NASH aetiologies, 13.3% vs. 14%, respectively (P=0.879). Median time to HCC recurrence did not change between the two groups, 22.6 vs. 13.3 months (P=0.274) [118]. NASH and obesity may be associated with a reduced quality of life [119], however no specific studies investigating quality of life (QoL) in NASH transplanted patients are yet available.
CONCLUSION
NAFLD/NASH has now become one of the most common indication for liver transplantation worldwide. Multidisciplinary management of NASH and NASH-associated comorbidities may mitigate morbidity and mortality in patients with NASH both before and after liver transplantation. Patients selection is crucial to achieve post-transplant survival comparable to other etiologies of liver disease. In transplant recipients, diet, physical activity, and adjustment of IS therapy are key for prevention of NASH recurrence. In the future, an improved risk stratification in NASH candidates for transplantation and new drugs for the treatment of NASH recurrence are expected.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





