


Graphical Abstract
INTRODUCTION
Hepatitis C virus (HCV) infection affects approximately 58 million people worldwide. It is a major cause of liver cirrhosis and hepatocellular carcinoma (HCC) [1]. The goal of HCV treatment is to achieve a sustained virological response (SVR), defined as undetectable HCV RNA 12 weeks after treatment completion, because it reduces liver-related morbidity and mortality. Direct-acting antivirals (DAA), which target nonstructural (NS) proteins essential for HCV replication, have substantially changed the landscape of HCV treatment because they produce an SVR rate greater than 95% [2].
HCV is a positive-sense single-stranded (ss) RNA virus that reproduces 1010 to 1012 virions per day with an error rate of 10-3 to 10-5 mutations per nucleotide per genomic replication [3]. This process can lead to abundant variants, including in the genomic regions targeted by DAA. Resistance-associated substitutions (RASs) are changes in the amino acid sequence of DAA-targeted NS proteins, including NS3A, NS5A, and NS5B. They are commonly present before DAA treatment [4,5], but they can also emerge during DAA therapy and can be associated with treatment failure [6].
In South Korea, the prevalence of anti-HCV antibodies is 0.6–0.71% [7,8], and genotypes (GTs) 1b and 2 account for more than 90% of cases [9]. Since the first DAA protocol, daclatasvir+ asunaprevir (DCV+ASN), was approved for reimbursement in 2015 for patients with GT 1b in whom mandatory RAS testing showed an absence of NS5A RASs L31 and Y93, it has shown a real-life SVR rate of 94.8-96.3% [10,11]. Due to cost issues, sofosbuvir/ledipasvir (SOF/LDV) was reimbursed for GT 1 patients not indicated for DCV+ASN. SOF+ribavirin (RBV) was reimbursed for GT 2 treatment and had a reported SVR rate of 94.2% [12]. After the highly effective pan-genotypic DAA glecaprevir/pibrentasvir (GLE/PIB) was approved in 2018, DCV+ASN, SOF+RBV, and dasabuvir+ombitasvir/paritaprevir/ritonavir (DSV+OMV/PTV/r) were discontinued in practice, though elbasvir/grazoprevir (EBR/GZR) was continued for GT1 patients. SOF/velpatasvir (SOF/VEL) and SOF/VEL/voxilaprevir (SOF/VEL/VOX) were approved in November 2022.
The causes of DAA failure include advanced liver disease, poor compliance, GT3, and the presence of RASs [13]. Prior DAA exposure can select for RASs and attenuate the efficacy of DAA retreatment. Despite the increase of patients with DAA failure, no data are available on RASs or retreatment status in South Korea. Therefore, we used next-generation sequencing (NGS) to analyze the RAS profiles and retreatment outcomes of patients with chronic HCV infection who failed DAA treatment in South Korea.
MATERIALS AND METHODS
Study population
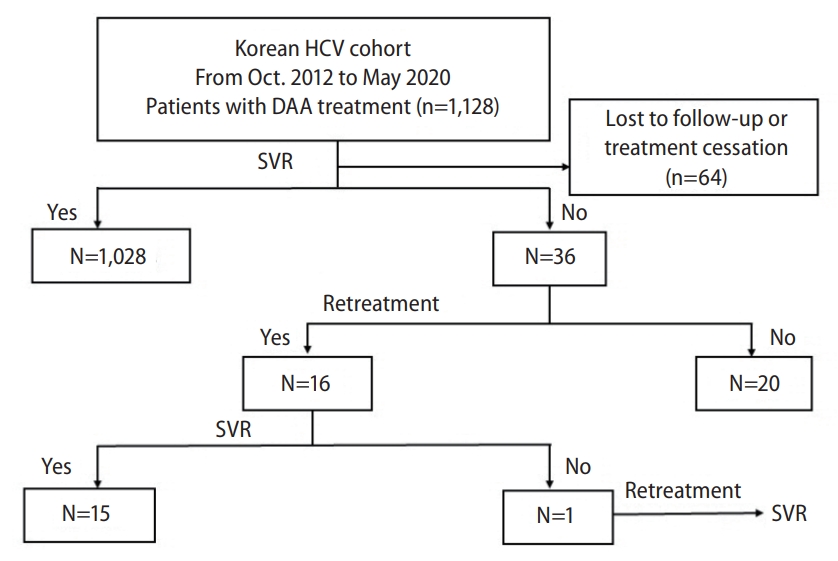
We analyzed data and blood samples from the South Korean HCV cohort, which prospectively enrolled patients older than 18 years with anti-HCV antibody positivity who voluntarily consented to participate in the study at 10 academic hospitals in South Korea between January 2007 and March 2020. From that population, patients with chronic HCV infection and DAA treatment were the source population for this study (n=1,128). After excluding patients who achieved an SVR after DAA therapy (n=1,028), we included 36 patients in whom DAA failed (Fig. 1). The study protocol was approved by the institutional review board of each hospital (IRB number: 2020-02-020, B-0706-046-002, 2010-01-072, 2012-02-014, 2008-03-009, 2020-02-060, 2020-02-041, 2017-080. 2007-0270. 20016-0345), and written informed consent was obtained from each enrolled patient before their inclusion in the cohort. This study was conducted according to the tenets of the Declaration of Helsinki.
Data and blood sample collection
Data on laboratory parameters (anti-HCV, serum HCV RNA, and HCV genotype), imaging studies, liver pathology, and transient elastography were collected from medical records upon patient enrollment. At initial enrollment, the participants were classified into three groups: chronic hepatitis, liver cirrhosis, and HCC, as described in previous studies. Patients who underwent successful curative treatment, such as resection or local ablation, and subsequently started DAA treatment were categorized as history of HCC group. The presence of a tumor was defined as a lesion on imaging delineated as HCC; this included individuals with lesions previously treated with chemoembolization who had evidence of radiographic tumor response with tumor necrosis. An active tumor was defined as the presence of arterial enhancement and venous washout on triphasic computed tomography or magnetic resonance imaging [14]. We obtained detailed information about antiviral treatments, which were prescribed at the discretion of the attending physicians.
Patients were prospectively followed every 3–12 months. If patients were lost to follow-up for >6–12 months, the research coordinator at the associated hospital contacted them via phone to confirm their clinical status and encourage a follow-up visit. Follow-up data were entered into the established electronic case report form on the homepage of the Korea Centers for Disease Control, Korean HCV cohort study website. An independent data management team regularly performed quality control.
Blood samples were collected at enrollment beginning in 2014, after obtaining separate consent for research purposes. However, follow-up sampling was not obligatory; therefore, the number of paired samples was small. Blood samples were centrifuged at 2,800 rpm within 2 hours of collection and transferred to a central laboratory within 24 hours under refrigerated conditions. The separated plasma was stored at -70°C.
Next-generation sequencing
HCV RNA was isolated from the plasma using a QIAamp MinElute virus spin kit (QIAGEN, Hilden, Germany). The concentration of ssRNA was calculated using Quant-IT RiboGreen (#R11490; Invitrogen, Waltham, MA, USA). Samples were run on a TapeStation RNA ScreenTape (Agilent, Santa Clara, CA, USA) to assess the integrity of the ssRNA. A library was prepared using 400 ng of ssRNA from each sample and an Illumina TruSeq mRNA sample prep kit (Illumina, Inc., San Diego, CA, USA). The samples were copied into first-strand cDNA using SuperScript II reverse transcriptase (Invitrogen) and random primers, which was followed by second-strand cDNA synthesis using DNA polymerase I and RNase H.
These cDNA fragments were subjected to an end repair process, the addition of a single ‘A’ base, and ligation of the indexing adapters. The products were purified and enriched using polymerase chain reaction (PCR). The libraries were quantified using quantitative PCR (qPCR) according to the qPCR Quantification Protocol Guide (KAPA Library Quantification kits for Illumina Sequencing platforms) and were qualified using a TapeStation D1000 ScreenTape (Agilent Technologies, Waldbronn, Germany). The indexed libraries were then sequenced by Macrogen Inc. (Seoul, Korea) using the HiSeqXten platform (Illumina).
After sequencing, FastQC (v0.11.5) was used to assess the read quality. Trimmomatic (v0.36) was used to remove adapter sequences and low-quality reads to reduce bias. DNA sequence data were aligned to the HCV genome reference using the Maximal Exact Match (MEM) algorithm in Burrows-Wheeler Alignment tool (BWA) [15]. We sorted the SAM/BAM files and duplication markings using SAMTOOLS v1.9 [16] and SAMBAMBA [17]. We detected single nucleotide variations and small insertions/deletions using mpileup from SAMTOOLS [16]. SNPEFF [18] was used to annotate the identified variants.
FASTQ was purified with VICUNA software to determine the HCV genotype [19]. and each sequencing read was competitively mapped to the HCV subtype reference genome. We counted the number of unique reads of good quality (mapping quality [MAPQ] >50) mapped to each reference and selected the genotype with the most numerous mapped reads.
Statistical analysis
Continuous variables are presented as median (interquartile range) and were compared with Student’s t-test. Categorical variables are presented as numbers (percentages) and were compared using the Chi-square test. An intention-to treat analysis was performed assuming that treatment failure occurred when DAA treatment was discontinued for any reason in patients who received at least one dose of a DAA. A per-protocol analysis was performed for patients who completed their treatment on schedule. All statistical analyses were performed using SPSS software version 25 (SPSS Inc., Armonk, NY, USA). All P-values were two-sided, and P<0.05 was considered statistically significant.
RESULTS
Characteristics of patients with first DAA failure and SVR rate after retreatment
From October 2012 to May 2020, 1,128 patients were treated with a DAA (Supplementary Table 1). An SVR was achieved in 1,028 of the 1,128 patients, and 64 patients discontinued treatment or were lost to follow-up (SVR rate: 91.1% by intention-to-treat analysis, 96.6% by per-protocol analysis) (Supplementary Table 2). We identified 36 patients (median age of 63 years, 18 males, 4 patients with liver cirrhosis, and 9 patients with HCC) with virologic failure of DAA treatment: DCV+ASN in 15, SOF+RBV in 13, LDV/SOF in 6, EBR/GZR in 1, and GLE/PIB in 2. Overall, GTs 1b, 2, and 3 were found in 20, 15, and 1 patient, respectively. Retreatment was performed in 16 patients, mostly with SOF/VOX/VEL or GP, and they had an SVR rate of 100% (Fig. 1). Among those 16 patients, 1 experienced 2 failures, with DCV+ASN and LED/SOF, but finally achieved an SVR with SOF/VOX/VEL (Table 1). SOF/VOX/VEL was not approved in Korea until November 2022, which was after our study period; therefore, it was used in these patients in clinical studies or as individual purchases from foreign pharmacies.
RAS profiles in patients with GT 1b infection and DAA failure
The NGS results showed that at least 1 baseline RAS was present in 9 of 10 patients with DCV+ASN or LED/SOF treatment failure; eight had an NS3A RAS, seven had an NS5A RAS, and seven had an NS5B RAS (Fig. 2). NS5A Y93 was the most prevalent RAS at baseline (5/10). Interestingly, the NS5A R30Q RAS was detected in two patients (Table 2).
Posttreatment RASs were analyzed in six patients using samples obtained between 13 and 166 weeks after treatment cessation. All six patients showed at least one posttreatment NS5A RAS: R30 (1/6), L31 (3/6), and Y93 (6/6). All four patients treated with NS3 protease inhibitor showed an NS3 RAS, whereas patients treated with NS5A or NS5B inhibitor did not have NS3 RASs (Table 3). In three patients with pre- and posttreatment samples, one with DCV+ASN treatment failure (#1) had treatment-emergent NS3 Q80R, NS5A L31M/V, and Y93H RASs at 157 weeks after DAA failure. In another patient with DCV+ASN failure (#2), NS3 168A and NS5A L31M RASs emerged, and the frequency of the Y93H RAS increased from 51% at baseline to 100% at 14 weeks after DAA failure. In the third patient, in whom LED/SOF failed (#11), baseline Y93H increased from 34.2% to 100%, but the NS3 RAS Y56F and NS5B RAS 316N were no longer observed by 166 weeks after DAA treatment (Table 4).
Furthermore, 8 of the 20 patients with GT 1b infection and DAA failure were successfully re-treated with DAAs: SOF/VOX/VEL after DCV+ASN failure (n=3), GLE/PIB after LED/SOF failure (n=2), DSV+OMV/PTV/r+RBV after LED/SOF failure (n=1), GLE/PIB after SOF+RBV failure (n=1, this patient was erroneously diagnosed with GT 2 infection), and SOF/VOX/VEL after failure with first DCV+ASN and then LED/SOF (n=1). Two of those patients with NS5A L31 or Y93 after their first DAA failure were successfully re-treated with SOF/VOX/VEL, and 1 patient with NS5A RASs R30 and Y93 was successfully retreated with GLE/PIB (Table 3).
RAS profiles in patients with GT 2 infection and DAA failure
The types of DAA failure in the 15 patients with GT 2 were as follows: SOF+RBV in 12, LED/SOF in one, GLE/PIB in one, and DCV+ASN in one. RASs were analyzed in 12 samples from 10 patients.
Six patients were tested for baseline RASs, including four with SOF+RBV failure, one with LED/SOF failure, and one with DCV+ASN failure. Only one of the six tested patients showed the NS3 Y56F RAS; however, neither an NS5A RAS nor NS5B RAS was found at baseline in these patients (Table 5). Posttreatment, the NS5B RAS was found in five patients who experienced SOF+RBV failure, and only one patient, who was misidentified as having a GT 1b infection, showed emergence of the NS5A F28C RAS after DCV+ASN failure (Table 6).
Among the 12 patients with GT 2 infection and SOF+RBV failure, 7 were successfully re-treated (6 with GLE/PIB and one with pegylated interferon+RBV). The patient erroneously given DCN+ASN was successfully re-treated with EBR/GZR+RBV.
RAS profile in the patient with GT 3 infection and DAA failure
The one patient with compensated cirrhosis and GT 3a infection was treated with GLE/PIB for 12 weeks but experienced virological failure. The baseline RAS was analyzed for this patient, and the NS5A RAS A30K was detected at a frequency of 100%. This patient has not yet been re-treated.
DISCUSSION
This study demonstrated the RAS features and retreatment outcomes of 36 patients with chronic HCV infection who experienced DAA failure in South Korea. Among the 10 patients with GT 1b, baseline RASs in NS3, NS5A, and NS5B were detected in eight, seven, and seven, respectively. After DAA failure, RASs in NS3, NS5A, and NS5B were detected in four, six, and two of six patients, respectively. However, among patients with GT 2, the only RAS detected at baseline was NS3 Y56F in one patient; after DAA failure, the NS5A F28C RAS was found in one patient who was erroneously treated with DCV+ASN. Among all 36 patients in our sample, 16 were retreated, with an SVR rate of 100%; therefore, active retreatment following a first DAA failure is recommended.
In the initial phase of DAA introduction in Korea, most patients with GT 1b infection were treated with DCV+ASN or LED/SOF, whereas those with GT 2 infection were treated with SOF+RBV. Although the SVR rates of genotype-specific DAAs are as high as 94.2–96.2% [11,12], 36 patients with virological failure on DAA were identified in this study. Baseline NS5A RASs significantly lowered the SVR rate in patients treated with DCV+ASN (65.4% vs. 94.3%) [20] in a previous clinical trial. Therefore, before 2017, a negative Sanger sequencing test for the NS5A RASs L31 and Y93 was mandatory for reimbursement of the DCV+ASN regimen in South Korea [21]. Among the 13 patients without a baseline RAS, as shown by Sanger sequencing, who were treated with DCV+ASV, NGS showed the presence of the Y93H RAS in 2. One patient had the Y93C/N RAS (56%/6%), and the other had the Y93H RAS (51.5%). Although the detection limit of Sanger sequencing is known to be 15–20%, a variant at a relatively low frequency (51.5%) could be missed by Sanger sequencing but detected with NGS.
Among the patients with GT 1b infection, the Y93 RAS was detected in 50% and 100% at baseline and after virological failure, respectively, whereas the L31 RAS was detected in 50% of patients after virological failure. Both the L31M and Y93H RASs significantly increased the 50% effective concentration (EC50) of DCV in GT 1b in vitro and exhibited synergism, showing >1,000-fold changes in EC50 [22]. Considering that the baseline prevalence of the NS5A RASs L31 and Y93 in Korean patients with GT 1b infection was reported to be 5.6% and 15.5%, respectively [23], they were likely to be associated with virological failure in Korean patients with GT 1b infection. Moreover, an international cohort study reported that NS5A RASs, including L31 and Y93, increased from 11% at baseline to up to 73% after failure with NS5A inhibitors [24]. The R30Q RAS by itself was not reported to be associated with DCV resistance, but it did increase the EC50 of DCV by 31,000– 37,000-fold when it co-presented with L31M and Y93 [22]. In our study, treatment-emergent NS5A RASs persisted at a high frequency (99%) for up to 157 weeks, which is compatible with previous results indicating that NS5A RASs persisted for 48 weeks posttreatment, whereas NS3 RASs returned to the wild type within 16 weeks after cessation, according to a direct sequencing analysis [25].
NS3 RASs Q80K/R and D168A/C/E/G/H/Y/Y were associated with resistance to asunaprevir in vitro and in vivo, but the role of the S122G RAS in asunaprevir failure was unclear [22]. Y56F was associated with resistance to grazoprevir [22]. The prevalence of natural NS3 RASs Q80, D168, S122G, and Y56F was reported to be 3.9%, 0.7%, 9.34%, and 26%, respectively [26]. In the present study, treatment-emergent Q80R and D168A RASs were associated with DCV+ASN failure and were detected at frequencies of 0.28% and 17% at 157 and 14 weeks after treatment cessation, respectively. Considering that almost all NS3 RASs returned to wild type after DAA cessation [25], these NS3 RASs might be present at higher frequencies immediately after DAA cessation.
NS5B RASs C316N and S556G in the GT 1b patients in our study population might be naturally occurring for non-nucleotide inhibitors. The prevalence of naturally occurring NS5B RASs in GT 1b was reported to be 12–25%, and the C316N RAS was the most prevalent [26,27]. Therefore, our result is consistent with those in previous reports.
When patients experience failure with NS5A or NS3 inhibitors, treatment with SOF/VOX/VEL is recommended [28]. However, DCV+ASN has mainly been used in East Asians, and few data are available on retreatment of patients with SOF/VOX/VEL. Although our patient population was small, we showed that treatment with SOF/VOX/VEL was highly effective for GT 1b HCV after DCV+ASN failure. In a Japanese study that evaluated the efficacy of LED/SOF treatment in patients who failed DCV+ASN treatment, the SVR rate was 86.7%, and the presence of cirrhosis and both NS5A L31 and Y93 RASs were poor response factors. In this study, a patient with a baseline Y93H RAS and DCV+ASN treatment failure who also failed LED/SOF+RBV and had treatment-enriched Y93H and treatment-emergent L31M/V was successfully treated with SOF/VOX/VEL.
Although GLE/PIB is not recommended for patients who fail an NS5A inhibitor–containing regimen, two patients with LED/SOF failure and NS5A Y93H RASs were treated with GLE/PIB and achieved an SVR. In GT 1b patients, NS5A Y93 and L31 RASs did not influence the treatment outcome with pibrentasvir [22]. In a study conducted in Japan, the SVR rate with GLE/PIB in patients with GT 1b who experienced failure with DCV+ASN or LED/SOF was 87.5%, and multiple NS5A RASs were detected in patients with GLE/PIB failure [29]. Therefore, SOF/VOX/VEL should be the retreatment regimen in patients with DCV+ASN failure.
The NS5B S282T RAS in GT 2a was associated with decreased susceptibility to sofosbuvir in vitro [30]. Although the emergence of NS5B S282T [31] and L159F [32] was reported in patients with GT 2b infection who experienced virologic failure with SOF+RBV, selection of sofosbuvir-resistant HCV is very rare and is associated with a significant reduction in viral fitness [33]. Therefore, virologic failure of SOF+RBV in patients with GT 2 infection might be associated not with RASs, but with other factors such as innate inadequacy of this regimen for GT 2, liver disease severity, ribavirin dosage, or medication adherence [34].In this study, we found no baseline or treatment-emergent NS5B RASs in patients with GT 2 infection who experienced failure with SOF+RBV. The proportion of HCC was higher in patients with SOF+RBV failure than in those with an SVR (30.8% vs. 9.8%), but the proportion of active HCC did not differ, probably due to the small number of active HCC patients. A study reported that active HCC was associated with DAA failure [14], so HCC might be one of the reasons for SOF+RBV failure. However, the time from the end of treatment to RAS testing ranged from 9–95 weeks, so the possibility that treatment-emergent RASs reverted to wild type could not be excluded. Treatment with GLE/PIB was highly effective in patients with GT 2 infection who experienced failure with SOF+RBV, showing a 100% SVR rate, and is currently recommended for patients with sofosbuvir failure [35]. In our study, GLE/PIB was also highly effective in patients with GT 2 infection and failure with SOF+RBV therapy.
The prevalence of GT 3 is very low (<1% in Korea) [36], and it is the most difficult genotype to treat because of the high frequency of RASs. Current guidelines recommend 8–12 weeks of GLE/PIB treatment for treatment-naïve GT 3 infections with compensated cirrhosis because of its 95% SVR rate [28,37]. In this study, a treatment-naïve patient with GT 3a infection and compensated cirrhosis experienced failure after 12 weeks of GLE/PIB therapy, and the NS5A A30K RAS was detected at a 100% frequency in that patient at baseline. With GT 3a, the NS5A RAS A30K occurs naturally with a frequency of 6% and does not decrease pibrentasvir sensitivity by itself, but it does lower sensitivity when Y93H is also present [38]. Therefore, it is unclear whether the NS5A A30K RAS was associated with GLE/PIB failure in this patient.
Most laboratories currently use Sanger sequencing as the gold standard for RAS tests; however, NGS offers potential advantages in terms of throughput, accuracy, and detection of low-frequency variants. Recent studies have shown that the results of NGS are highly concordant with those of Sanger sqeuncing [39,40]. However, NGS requires higher viral loads (4.5 log10 IU/mL) than Sanger sequencing (1,000 IU/mL) for RAS detection [39]. In our study, NGS corrected genotyping errors in 2 patients. NGS has been reported to have 96.1% specificity in determining the HCV genotype, and it is useful for distinguishing mixed infections [39].
Our study has several limitations. First, the small number of patients with DAA failure is insufficient for the study results to be generalizable. Second, RASs were not analyzed both at baseline and after virological failure for all patients; therefore, it was difficult to interpret whether the RASs detected after DAA failure were present at baseline or emerged after treatment failure. Third, the time points for the RAS analyses after virologic failure were not uniform, and RASs can be gradually replaced by the wild type, especially NS3 RASs. Fourth, we did not analyze RASs for the SVR group and thus cannot evaluate how the RASs affected treatment outcomes by directly comparing the SVR group and DAA-failure group. However, in other studies, the prevalence of natural RAS in treatment-naïve patients was much lower than in the patients with virological failure in our study. Fifth, because fewer than 50% of the patients with DAA failure were re-treated with a DAA, the number of re-treated patients was too small for a suitable statistical analysis; therefore, the retreatment outcomes of patients with DAA failure could be biased. The low retreatment rate is partly because SOF/VEL/VOX is currently commercially unavailable, and Korea did not have an option for NS5A inhibitor failure during the study period. Since rescue therapy with SOF/VEL/VOX has been reimbursed in Korea since November 2022, the efficacy of rescue therapy can be further elucidated. However, the retreatment rate of patients with GT 2 is also unsatisfactory, probably because of the absence of reimbursement for retreatment or cost issues for second-line treatment. Therefore, efforts should be made to improve the retreatment rate and therapeutic regimens of patients with DAA failure.
In conclusion, our study revealed that DAA failure occurs mainly in patients treated with DCV+ASN for GT 1b infection and those treated with SOF+RBV for GT 2 infection; approximately half of DAA-failed patients underwent retreatment with SOF/VEL/VOX or GP, and they had a 100% SVR irrespective of the presence of baseline or posttreatment RASs. NS5A RASs at baseline and after virological failure were prevalent in patients with GT 1b infection and DAA failure. In contrast, RASs in patients with GT 2 and DAA failure were rare both at baseline and after DAA failure. NS5A RASs Y93 and L31 were associated with DAA failure in GT 1b. Further studies are required to assess treatment outcomes and the factors of treatment failure.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement1
Supplement1 Print
Print





