

INTRODUCTION
Portal hypertension is one of the major complications of chronic liver disease (CLD), resulting in the development of portal vein-systemic collateral circulation that includes esophageal and gastric varices and portal hypertensive gastropathy (PHG).1
Approximately one-third of patients with varices develop acute bleeding,2 and each episode of variceal bleeding is associated with a 30 percent risk of mortality.3 The poor prognosis of bleeding from varices has led to an attempt to identify patients at high-risk for bleeding and attempts to prevent bleeding. The current consensus recommends that all patients with cirrhosis of the liver should be screened for varices by upper endoscopy,1 and if varices are detected, then either pharmacologic or endoscopic treatment are recommended to prevent bleeding.4 However, such practice eventually places a significant burden on medical and economical resources.
Accordingly, a number of studies have been recently attempted to find a more practical and non-invasive method for predicting the presence of varices.5-12 However, such efforts using non-invasive parameters including platelet count, spleen size, and albumin concentration have not been accepted as substitutes for endoscopy. Consequently, endoscopic screening is still the best method for the diagnosis of varices. Most of the subjects included in these studies had cirrhosis in relatively advanced stages. However, patients without evident stigmata of cirrhosis can also develop varices and the risk of bleeding should be identified in these patients. In addition, acute bleeding from PHG is less frequent than from varices, but it might be severe and fatal as well.13-15
Therefore, the aim of this study was to identify new non-invasive parameters for predicting the presence of varices and PHG in patients with CLD including patients with less advanced stages and to assess the accuracy of the parameters for diagnosing varices and PHG.
PATIENTS AND METHODS
Patients
The medical records of patients with CLD that underwent both first screening upper endoscopy and liver helical CT within an interval of three months were reviewed at Samsung Medical Center from January 1, 2006 to June 30, 2007. In this study, patients with CLD were determined as who were regularly followed-up for liver diseases including hepatitis B or C virus infection, alcoholic or non-alcoholic fatty liver disease, autoimmune hepatitis and primary biliary cirrhosis. Exclusion criteria for the study were: previously diagnosed varices or PHG; prophylactic ╬▓-blocker therapy; hepatocellular carcinoma; portal vein or splenic vein thrombosis; previous portosystemic shunt surgery or transjugular intrahepatic portosystemic shunt stent placement; hematologic disorders such as aplastic anemia and myelodysplastic syndrome.
The study protocol was performed according to the principles of the Declaration of Helsinki.
Clinical, laboratory, imaging and endoscopic data
The following clinical and laboratory information was collected from each patient: age, gender, etiology of liver disease, platelet count, prothrombin time (PT), serum albumin, serum total bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), presence and degree of ascites and encephalopathy assessed according to the Child-Pugh classification.
In order to reflect splenomegaly as a predictor for varices and PHG, we used the multidimensional index for spleen volume. From the images of the helical CT of the liver, the spleen length (L), width (W), and thickness (T) were measured in cm and the M-Index was calculated by multiplication of these measurements. CT examinations were performed with multidetector CT (Light-Speed 16, GE Healthcare, Milwaukee, WI; Brilliance 40, Philips Medical Systems, Best, The Netherlands). The CT parameters were 120 kVp, 200-300 mAs, 1.25 mm├Ś16 and 0.625 mm├Ś40 section collimation (pitch, 0.926-0.938), and a single-breath-hold helical acquisition of 5-8 s depending on the liver size. Using these raw data, a transverse image was obtained with a slice thickness of 5 mm and an interval of 2.5 mm (overlap 2.5 mm). Bezerra et al16 reported the M-Index correlated well with spleen volume (r=0.957). The L was obtained by multiplying the number of sections where the spleen was visualized by the thickness of the sections. The W and the T values were recorded at the point of maximal width and thickness of the spleen on any section.
All endoscopic images were reviewed in consensus by two endoscopists (YW Min and GY Gwak) who have 2 and 8 years' experience in digestive endoscopy, respectively. The severity of the esophageal varices (EV) was subdivided into three classes (Grade 1 to 3) according to the criteria proposed by the Japanese Research Society for Portal Hypertension.2,17,18 Grade 1 varices were defined as small straight varices, grade 2 as enlarged tortuous varices that occupied less than one-third of the lumen, and grade 3 as large coil-shaped varices that occupied more than one-third of the lumen. The severity of both gastric varices (GV) and PHG were evaluated according to the criteria proposed by the 1992 New Italian Endoscopic Club Consensus.19 GV were subdivided into three classes (Form 1 to 3): Form 1 was straight varices that protruded less than the radius into the lumen; Form 2 was straight varices that protruded more than the radius into the lumen; Form 3 was tortuous, cerebriform varices. The severity of PHG was subdivided into two classes, mild and severe. A mosaic-like pattern was classified as a mild PHG with a low bleeding risk, while red marks were classified as a severe PHG with a high tendency to bleed.14,19 Large varices more than grade 1 or severe PHG with red marks were regarded as high-risk lesions for bleeding.
Statistical analysis
Categorical variables were compared using Žć2-test or Fisher's exact test as appropriate. Continuous variables were compared using the Student's t-test for parametric method or Mann-Whitney's U test for nonparametric methods. Multivariate logistic regression analysis was performed on parameters which were significantly different in a univariate analysis between the two groups of patients with and without varices and PHG, in order to determine the variables independently associated with the presence of varices and PHG. The area under the receiver operating characteristic (AUROC) curves were used to select the parameters that showed good discriminative power for predicting the presence of EV, GV and PHG. In addition, receiver operating characteristic (ROC) curves were used to determine the VAP (varices and portal hypertensive gastropathy) score cut-off value with the best sensitivity and specificity. Data are shown as the mean┬▒standard deviation and each odds ratio (OR) and AUROC curves are presented together with its 95% confidence interval (95% CI). A two-sided P<0.05 was considered statistically significant for all analyses. Data were analyzed using SPSS 12.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Two hundred and thirty two patients were included in this study. Of these, 148 patients (63.8%) were male and the mean age was 52.3 years. One hundred and ninety-four patients (83.2%) were chronic liver disease or Child-Pugh class A liver cirrhosis, 31 patients (13.4%) were Child-Pugh class B, and 7 patients (3.4%) were class C. The etiologies of liver disease were hepatitis B virus infection in 144 patients (62.1%), hepatitis C virus infection in 21 patients (9.1%), and other causes such as alcoholic hepatitis, autoimmune hepatitis, primary biliary cirrhosis, and fatty liver in 67 patients (28.9%).
Overall, 102 patients (44.0%) had endoscopic evidence of EV, GV or PHG. Eighty-seven patients (37.5%) had EV; grade 1 in 44 (19.0%), grade 2 in 35 (15.1%), and grade 3 in 8 (3.4%) patients. GV was noted in 31 patients (13.4%); grade 1 in 17 (7.3%) and grade 2 in 13 (5.6%) patients. Forty-nine patients (21.1%) had PHG; mild PHG in 48 (20.7%) and severe PHG in 1 patient (0.4%). Fifty patients (21.6%) had high-risk lesions for bleeding.
Table 1 shows the main characteristics of the two groups of patients according to the presence of EV, GV and PHG. There were no significant differences between the two groups with regard to age, gender, and ALT levels. Patients with EV, GV or PHG had a significantly prolonged PT, elevated total bilirubin levels, elevated AST levels, higher Child-Pugh score, lower platelet count, and lower albumin levels compared to patients without EV, GV and PHG. The M-Index was greater in patients with EV, GV or PHG.
From the multivariate logistic regression analysis, platelet count, serum level of albumin, and M-Index were independently associated with the presence of varices and PHG (OR, 0.990; 95% CI, 0.984-0.997; P=0.003, OR, 0.328; 95% CI, 0.168-0.641; P=0.001, OR, 1.002; 95% CI 1.001-1.003; P=0.002, respectively).
For a more powerful predictor, we combined three independent parameters and a VAP scoring system was developed: (=[platelet count (/mm3)├Śalbumin (g/dL)]/[M-Index (cm3)]). The AUROC curve of the VAP score was 0.850 (95% CI, 0.801-0.899), which was larger than the values from each parameter (Table 2).
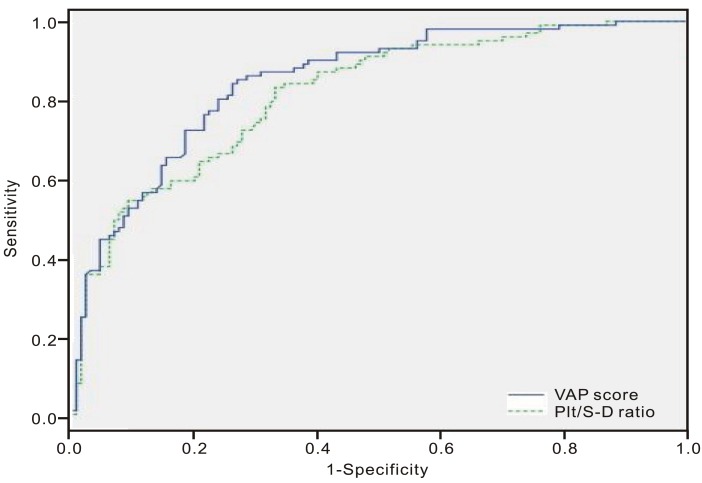
Next, the platelet count/spleen diameter ratio (Plt/S-D ratio) was adjusted in our study population: this has been reported to be the most accurate parameter for predicting EV in cirrhotic patients to date.20 The Plt/S-D ratio showed the AUROC curve of 0.818 (95% CI, 0.764-0.871) in our study population (Table 3), which was lower than the VAP score (0.850; 95% CI, 0.801-0.899; P=0.034; Fig. 1). In addition, the VAP score had better discriminative power for predicting the presence of high-risk lesions for bleeding compared to the Plt/S-D ratio in our study population (AUROC curves of 0.846; 95% CI, 0.793-0.900 vs. 0.785; 95% CI, 0.716-0.854; P=0.002; Table 3).
Finally, the ROC curves were used to assess the VAP score cut-off value with the best sensitivity and specificity for predicting the presence of EV, GV and PHG. The cut-off value of 861 had a sensitivity of 85.3%, a specificity of 73.1%, a positive likelihood ratio of 3.17, and a negative likelihood ratio of 0.20. The positive and negative predictive values for the presence of EV, GV and PHG with this cut-off value were 71.4% and 86.4%, respectively. For predicting high-risk lesions for bleeding, with a cut-off value of 861, the sensitivity was 92.0%, specificity 58.2%, positive likelihood ratio 2.20, negative likelihood ratio 0.14, positive predictive value 37.7% and negative predictive value 96.4% (Table 4). In addition, a subgroup analysis was performed according to the Child-Pugh class and etiology of liver disease. The sensitivity and specificity of VAP score were 79.4% and 75.4% and 94.1% and 100% in the Child-Pugh class A and B/C groups, respectively. In the patients with chronic viral hepatitis group, sensitivity and specificity were 87.2% and 67.8%, respectively. In the patients with non-viral liver disease, sensitivity and specificity were 79.2% and 83.7%, respectively.
DISCUSSION
A number of studies have recently addressed non-invasive methods for predicting the presence of varices in patients with liver cirrhosis.5-12,21 Even though upper endoscopy is the gold standard for identifying varices, non-invasive methods are needed for detecting varices to reduce the cost and discomfort to patients as the number of patients with CLD increases. However, there has been no method introduced that could substitute for endoscopy for the diagnosis of varices. In addition, previous attempts were limited by studying patients with cirrhosis in relatively advanced stages, where only EV was the focus of detection.5-12,21 Although EV is the most frequent focus of bleeding in patients with portal hypertension, GV and PHG can develop without EV and cause massive, life-threatening bleeding.13,22-24 Indeed, in the present study there were 15 patients (6.5%) that were confirmed as having GV or PHG without EV. Fontana et al15 reported that PHG was more prevalent in patients with more fibrosis on liver biopsy (26% in patients with Ishak score of 3 and 51% in patients with Ishak score of 6). These data suggest that PHG could be associated with more severe portal hypertension. Therefore, GV and PHG also need attention by clinicians. In order to overcome the limitations of previous studies, this study was designed to identify more accurate, non-invasive parameters for predicting the presence of EV, GV and PHG in patients with CLD including large numbers of non-cirrhotic patients. Most of patients included in the present study (194 patients, 83.2%) had chronic liver disease or were class A according to the Child-Pugh classification.
To date, a few single parameters, such as the platelet count, PT, serum albumin, AST, and splenomegaly have been reported to be correlated with the presence of varices and PHG.5-12 The result of the present study also demonstrated that total bilirubin, serum albumin, AST, platelet count, PT, Child-Pugh score, and spleen volume were associated with the presence of varices and PHG. In order to reflect splenomegaly more accurately, the multidimensional spleen volume measurement method was used rather than uni-dimensional spleen size measurement method, in addition, CT images were used to measure the sizes. As a result, the spleen volume was found to have the strongest discriminative power for the presence of EV, GV and PHG. Although CT images were used to measure spleen volume in the present study, it is also possible and even more practical to use ultrasonography in actual clinical practice. A validation study using ultrasonography is now being performed.
In addition to the single parameters, Giannini et al21 proposed the Plt/S-D ratio as a non-invasive tool to predict the presence of EV in patients with cirrhosis. They demonstrated that the AUROC curve of the Plt/S-D ratio was 0.981, and that a cut-off value of 909 of the Plt/S-D ratio had positive and negative predictive values for EV of 96% and 100%, respectively. Moreover, in a multi-center study performed to validate the formula, the accuracy (AUROC curve) of the Plt/S-D ratio was 0.860, which was significantly greater compared to either the platelet count alone or the spleen diameter alone. In addition, a cut-off value of 909 had positive and negative predictive values for EV of 76.6 and 87%, respectively.20 When the accuracy of the Plt/S-D ratio and the VAP score was assessed in the subjects of this study, the VAP score had superior results for predicting the presence of varices and PHG as well as high-risk lesions for bleeding compared to the Plt/S-D ratio (AUROC curves of 0.850; 95% CI, 0.801-0.899 vs. 0.818; 95% CI, 0.764-0.871; P=0.034 and AUROC curves of 0.846; 95% CI,0.793-0.900 vs. 0.785; 95% CI, 0.716-0.854; P=0.002, respectively).
The present study was limited in that it employed a retrospective design and that it had probable selection bias. Because chronic liver disease is not an indication of screening endoscopy for varices, many patients with CLD who underwent first screening endoscopy could be thought to be selected subjects. However, South Korea is a country with high prevalence of gastric cancer and screening endoscopy for gastrointestinal malignancy is recommended at least every two years. Therefore, the enrolled patients with CLD were not selected subjects who had other reasons for performing upper endoscopy. Since the study was retrospective, a prospective validation in a new cohort is needed. Therefore further study is ongoing for validating the VAP scoring system in a large scale and in a prospective manner. In addition, our assessments regarding the presence and severity of varices and PHG could be thought to be made inconsistently. However, our institution is reporting the results of upper endoscopy regarding varices and PHG using a structured form. Furthermore, to overcome this limitation, all endoscopic results and images were reviewed in consensus by two experienced endoscopists.
In conclusion, the results of this study showed that the VAP scoring system could be used to predict the presence of EV, GV and PHG in patients with CLD, including non-cirrhotic patients, more accurately than any other single or combined parameter previously proposed. Therefore, we expect using the VAP scoring system as a screening tool to detect patients that have a high probability to have EV, GV and PHG among the patients with CLD, although a validation is necessary in the future.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




