

INTRODUCTION
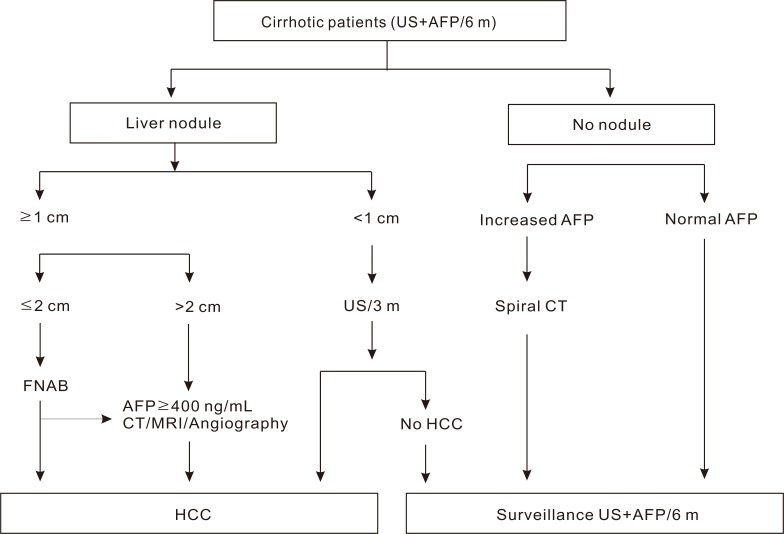
European Association for the Study of the Liver (EASL) guideline in 2000 and Korean Liver Cancer Study Group (KLCSG) guideline in 2003
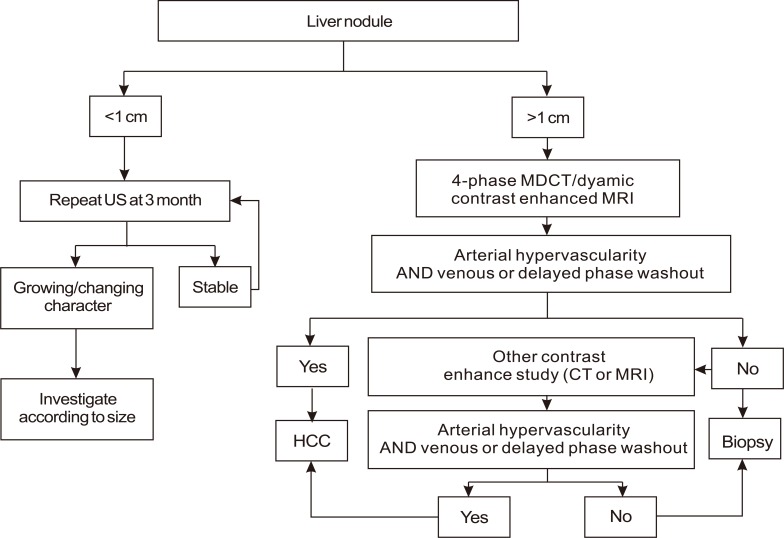
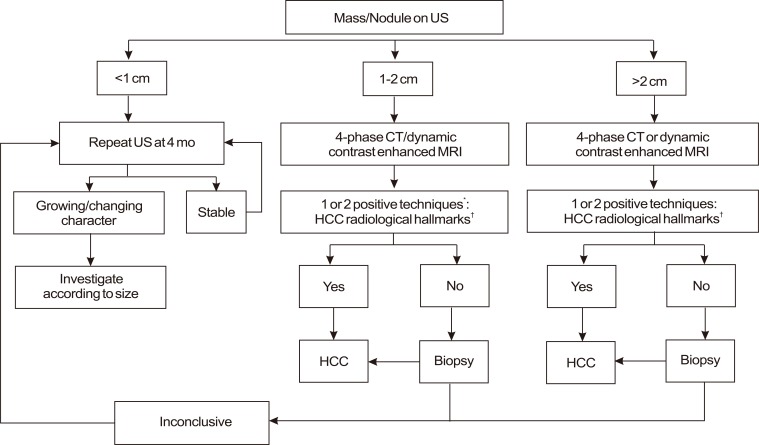
American Association for the Study of Liver Diseases (AASLD) guideline on the management of HCC in 2005 (Fig. 3).11
Nodules found on ultrasound surveillance that are smaller than 1 cm should be followed with ultrasound at intervals from 3-6 months.
Nodules of 1-2 cm found on ultrasound screening of a cirrhotic liver should be investigated further with two dynamic studies, either CT scan, contrast ultrasound or MRI with contrast. If the appearances are typical of HCC (i.e., hypervascular with washout in the portal/venous phase) in two techniques, the lesion should be treated as HCC.
If the nodule is larger than 2 cm at initial diagnosis and has the typical features of HCC on one dynamic imaging technique, biopsy is not necessary for the diagnosis of HCC. Alternatively, if the AFP is >200 ng/mL, biopsy is also not required.
If the vascular profile on imaging is not characteristic or if the nodule is detected in a non-cirrhotic liver, biopsy should be performed.
If the biopsy is negative for HCC, patients should be followed by ultrasound or CT scanning at 3-6 monthly intervals, until the nodule either disappears, enlarges, or displays diagnostic characteristics of HCC.
New guidelines for hepatocellular carcinoma diagnosis
-
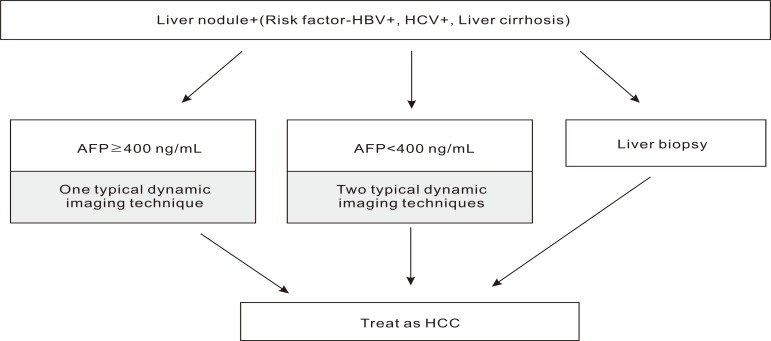
When nodules are detected in ultrasound surveillance in a high risk group for HCC (positive for hepatitis B or C virus, or liver cirrhosis), dynamic contrast enhancement CT or MRI should be performed for the diagnosis.
If the serum AFP level is ≥200 ng/mL in high-risk patients, typical characteristic of HCC in either dynamic contrast enhancement CT or dynamic contrast enhancement MRI lead to the diagnosis of HCC.
If the serum AFP level is <200 ng/mL, two or more positive findings of 1) dynamic contrast enhancement CT, 2) dynamic contrast enhancement MRI or 3) hepatic arterial angiography would lead to the diagnosis of HCC.
When a tumor of 2 cm or larger in patients with liver cirrhosis has typical characteristic of HCC in dynamic contrast enhancement CT or MRI, one could diagnose it as HCC regardless of the serum AFP levels.
The lesion does not satisfy the above criteria or shows atypical findings of HCC, biopsy should be performed for the diagnosis.
-
If nodules of high risk patients are smaller than 1 cm, which diagnosis may not be verified by a radiologic or histologic examination, a tumor marker test and ultrasonography should be performed several times, repeatedly, in an interval of three to six months, monitoring for any increase in the size and the level of tumor marker.
-
Nodules larger than 1 cm found on ultrasound screening of a cirrhotic liver should be investigated further with either 4-phase multidetector CT scan or dynamic contrast enhanced MRI.
Nodules found on ultrasound surveillance that are smaller than 1 cm should be followed with ultrasound at intervals from 3-6 months.
-
If the biopsy is negative for patients with HCC, the lesion should be followed by imaging at 3-6 monthly intervals, until the nodule either disappears, enlarges, or displays diagnostic characteristics of HCC. If the lesion enlarges but remains atypical for HCC a repeat biopsy is recommended.
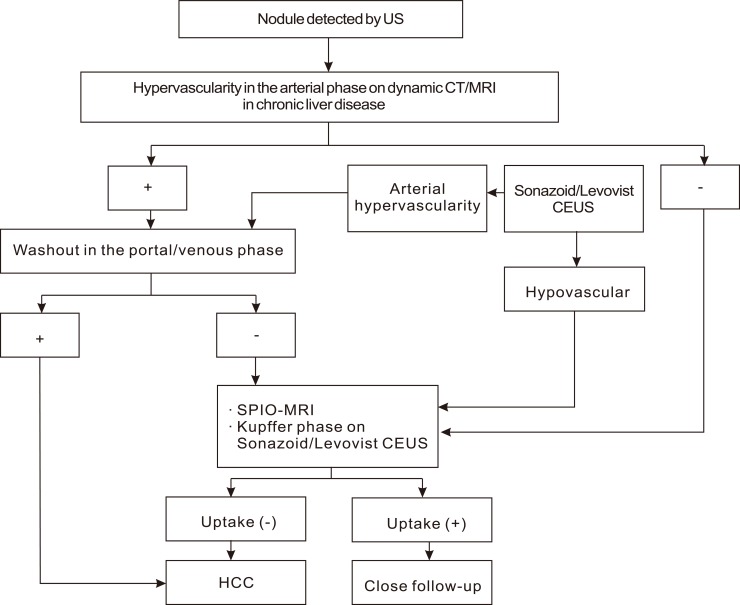
Typical HCC can be diagnosed by imaging regardless of the size if a typical vascular pattern, i.e., arterial enhancement with portal-venous washout, is obtained on dynamic CT, dynamic MRI, or contrast enhanced ultrasonography (CEUS).
Nodular lesions show an atypical imaging pattern, such as iso- or hypo-vascular in the arterial phase or arterial hypervascularity alone without portal-venous washout, should undergo further examinations such as SPIO MRI or CEUS.
In cirrhotic patients, nodules less than 1 cm in diameter detected by ultrasound should be followed every 4 months the first year and with regular checking every 6 months thereafter.
In cirrhotic patients, diagnosis of HCC for nodules of 1-2 cm in diameter should be based on non-invasive criteria or biopsy-proven pathological confirmation. A second biopsy is recommended in case of inconclusive findings, or growth or change in enhancement pattern identified during follow-up
In cirrhotic patients, nodules more than 2 cm in diameter can be diagnosed for HCC based on typical features on one imaging technique. In case of uncertainty or atypical radiological findings, diagnosis should be confirmed by biopsy.
-
Non-invasive criteria can only be applied to cirrhotic patients and are based on imaging techniques obtained by 4-phase MDCT scan or dynamic contrast-enhanced MRI. Diagnosis should be based on the identification of the typical hallmark of HCC. While one imaging technique is required for nodules beyond 1 cm in diameter, a more conservative approach with 2 techniques is recommended in suboptimal settings.
Cut-off value of AFP was lowered from 400 ng/mL to 200 ng/mL.
Tumor which is 2 cm or larger and with typical characteristics of HCC in dynamic contrast enhancement CT or MRI could be diagnosed as HCC regardless of the serum AFP level in the patients with liver cirrhosis on the basis that a few reports6,7,19 suggested that the diagnostic accuracy of HCC on imaging was 100% with tumors 2 cm or larger.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




