Harnessing hepatitis B core-related antigen measurement to optimize posttreatment monitoring
Article information

Dear Editor,
We thank Professor Liaw for taking the time to comment on our study [1,2]. His expertise in the field and insightful feedback allow us to clarify important aspects that may have been confusing or inadequately explained.
REGARDING THE ASSAY SENSITIVITY FOR HEPATITIS B CORE-RELATED ANTIGEN
We agree that the commercial assay used in this study was not sensitive enough to precisely quantify serum hepatitis B core-related antigen (HBcrAg) levels when the serum levels were lower than 1,000 U/mL. We were aware of this limitation and discussed it in our article. Additionally, our observation that serum HBcrAg levels only fluctuated mildly after nucleos(t)ide analogue (NA) cessation could be related to the insensitivity of the method of measurement. More sensitive assays, like the iTACT-HBcrAg [3], may uncover more subtle fluctuations in serum HBcrAg and thus reveal different patterns of posttreatment changes. Moving forward, utilizing or developing more sensitive HBcrAg assays will be crucial for fully leveraging this biomarker’s potential predictive utility across a wider range of values.
A TIME-VARYING VARIABLE IS DIFFERENT FROM DIFFERENCES BETWEEN TIME POINTS
While the assay might lack sensitivity at low HBcrAg levels for detecting subtle kinetic differences, this does not negate our major finding that the most recent HBcrAg measurement outperforms the end-of-treatment (EOT) value for predicting clinical relapse (CR). The similar CR incidence observed between patients with decreasing versus stable or increasing annual HBcrAg trajectories should not be misinterpreted as in conflict with the superiority of the most proximate HBcrAg level. As a matter of fact, modeling a time-varying explanatory variable is distinctly different from analyzing changes between repeated measurements over time, as time-varying variables preserve the exact data points with time indices [4]. In short, our analysis demonstrates that the most recent HBcrAg value relative to CR is most predictive of risk, regardless of prior values. We are confident that this novel finding broadens our current understanding of the application of HBcrAg in optimizing the care of patients discontinuing NA therapy [5].
COMPARISONS TO QUANTITATIVE HEPATITIS B SURFACE ANTIGEN
Professor Liaw astutely observed that the proportion of CR in patients with quantitative hepatitis B antigen (qHBsAg) <100 IU/mL was numerically lower compared to those with HBcrAg <1,000 U/mL during off-therapy monitoring [2]. Nonetheless, there was no significant difference in this comparison. In fact, our observation that the time-varying HBcrAg levels outperform the time-varying qHBsAg levels in predicting CR among relapse-naïve patients did not result from sporadic comparisons of this kind. Rather, our finding is supported by the results of a multivariable Cox proportional hazards model specifically examining the associations of these biomarkers with CR risk. Moreover, our study does not argue against the predictive value of EOT qHBsAg, which has been shown in prior studies, including our own [6,7]. As shown in Table 2 in our article, the present study actually showed that EOT HBsAg level was an independent CR risk predictor, in addition to time-varying HBcrAg and EOT anti-HBe positivity.
SEROCLEARANCE OF HEPATITIS B SURFACE ANTIEN AS A STUDY OUTCOME
We also agree that seroclearance of HBsAg may indicate a functional cure and is an acceptable endpoint for NA treatment. However, HBsAg loss occurs relatively infrequently compared to CR. Thus, larger samples are essential to exploring predictors of HBsAg seroclearance [8]. In our study population, HBsAg loss was observed in 21 patients during post treatment follow-up. Following Professor Liaw’s recommendation, we estimated a cumulative incidence of 19.9% (95% confidence interval: 12.8–25.6%) for HBsAg seroclearance at 8 years, with antiviral therapy resumption as a competing risk event to avoid overestimation [9]. Investigating dynamic HBcrAg levels for predicting HBsAg loss compared to other biomarkers was beyond this study’s scope. Further dedicated research in larger cohorts is warranted to examine associations between fluctuating HBcrAg trajectories and subsequent HBsAg clearance or seroconversion after NA cessation.
EARLY AND INTENSIVE HBV DNA MEASUREMENT IS ESSENTIAL AFTER TREATMENT CESSATION
We appreciate Professor Liaw underscoring the importance of frequently monitoring serum HBV DNA levels after NA cessation. The updated guidance from the Asian Pacific Association for the Study of the Liver (APASL) recommends monthly screening for the first 3 months, then bi-monthly or trimonthly in the year thereafter, should viremia remain undetected [10]. This intensive early monitoring intends to swiftly identify emerging viral breakthrough, as rapidly rebounding viremia predicts impending hepatitis flares or even severe acute exacerbations [11,12].
DISTINCT ROLES OF HBV DNA VERSUS ANTIGENEMIA IN POSTTREATMENT MONITORING
In our opinion, the role of HBcrAg or HBsAg levels versus HBV DNA is distinctly different for relapse prediction. First, HBV DNA levels are uniformly very low or practically undetectable when NA therapy ceases per eligibility guidelines. In contrast, antigen levels often remain detectable at variable levels despite meeting cessation criteria. Besides this, the rebound of viremia can rapidly spike from undetectable to extremely high levels within weeks, whereas HBcrAg and HBsAg fluctuate mildly after NA cessation in most patients. Therefore, we posit that serum HBV DNA provides a forecast for imminent active hepatitis and is especially useful right after treatment cessation [13]. On the other hand, the levels of antigenemia may better assess the relapse risks in the long term.
In response to the comment, we performed a comparative analysis examining all three biomarkers as time-dependent variables along with their interaction terms. The time-varying HBcrAg level emerged as the sole factor independently associated with CR risk (Table 1), as compared to the time-varying HBsAg and the time-varying HBV DNA levels, all of which were measured annually. However, this result should not be misinterpreted as indicating that HBcrAg could replace HBV DNA monitoring. Unlike HBsAg or HBcrAg, HBV DNA needs to be measured much more frequently than once a year, especially within the first year after NA cessation. What our findings suggest is that including serum HBcrAg measurement may complement HBV DNA testing for optimized posttreatment monitoring of patients stopping antiviral treatment. Further research should continue investigating how best to integrate both biomarkers clinically.
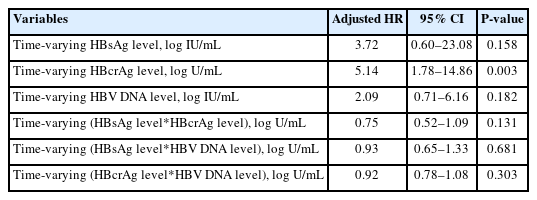
The regression model including all three time-varying biomarkers
SUMMARY
In summary, while the HBcrAg assay limitations restrict detecting subtle kinetic fluctuations posttreatment, this does not refute that the most recent level outperforms the EOT measurement for CR forecasting, irrespective of prior trajectories. Still, high-sensitivity assays may uncover finer fluctuations and patterns, so further optimization is indispensable. Besides this, our multivariate modeling demonstrated that time-varying HBcrAg is more predictive of CR than dynamic HBsAg, although isolated comparisons might show comparable capacities. While HBsAg seroclearance represents an important outcome, larger studies are needed to investigate posttreatment antigenemia kinetics for predicting its occurrence. Finally, uniformly suppressed viremia precludes the utility of EOT HBV DNA levels in risk stratification. However, rapid and fierce viral rebounds signal impeding hepatitis risk, mandating frequent DNA monitoring early after treatment cessation. Hence, HBV DNA and HBcrAg monitoring likely play complementary, rather than competing, roles in predicting and preventing posttreatment relapses.
Notes
Authors’ contribution
Manuscript drafting: Ying-Nan Tsai, Yao-Chun Hsu. Manuscript edition and final approval: all authors.
Conflicts of Interest
Ying-Nan Tsai reported no conflicts of interest. Jia-Ling Wu reported no conflicts of interest. Yao-Chun Hsu has received research grants from Gilead Sciences, lecture fees from Abbvie, Bristol-Myers Squibb, Gilead Sciences, and Novartis, and has served as an advisory committee member for Gilead Sciences and Sysmex.
Abbreviations
HBcrAg
hepatitis B core-related antigen
NA
nucleos(t)ide analogs
EOT
end of treatment
CR
clinical relapse
qHBsAg
quantitative hepatitis B antigen
HBsAg
hepatitis B surface antigen