

INTRODUCTION
Hepatocellular carcinoma (HCC) is a leading cause of cancer-related mortality together with lung and stomach cancers.1 Despite the development of a number of modalities for treatment of HCC, the mortality associated with HCC is still high. The reason may be associated with difficulty of detection of early HCC due to the rapidly-infiltrating growth pattern of HCC, simultaneous presence of multiple tumors, and ambiguity of HCC-related symptoms.2,3 Thus, the number of cases of HCC with operability is very small. A recent study reported that only 30% of patients with HCC are indicated to potentially curative treatments, even fewer in Asia.4 Prognosis of patients with early stage HCC or operability is relatively good due to availability of curative therapies such as surgical resection or liver transplantation, radiofrequency ablation (RFA), and percutaneous ethanol injection therapy (PEIT). However, although there are many palliative therapies, such as transarterial chemoembolization (TACE), systemic chemotherapy, and radiation therapy, the prognosis of patients with advanced HCC or inoperability remains poor.
Among the palliative therapeutic modalities, TACE is the current standard treatment for patients who are not candidates for curative therapies. On the other hand, TACE is contraindicated in advanced HCC with main portal vein tumor thrombus, massive or diffuse infiltration type, poor liver function, and severe hepatic arterioportal shunt.5 Because of economic burden, sorafenib, a multikinase inhibitor with antiangiogenic, proapoptotic, and Raf kinase inhibitory effects, which is recommended for advanced HCC, is limited to use in Korea.6-8 Actually, in clinical practice of Korea, sorafenib cannot be easily applicable to Child-Pugh class B or C patients with advanced HCC, because they were not covered by Korean medical insurance. In addition, sorafenib is associated with significant complications, especially in the Asian population, and the efficacy of sorafenib in patients with portal vein invasion or extrahepatic metastasis is significantly diminished.9,10 Therefore, hepatic arterial infusion chemotherapy (HAIC) can be an alternative option in this situation. In addition, as an alternative therapy for intractable advanced HCC, some studies have suggested that HAIC with 5-fluorouracil (5-FU) and cisplatin might have survival benefits.5,9,11,12 In particular, HAIC has been recommended for advanced HCC with portal vein tumor thrombosis, venous tumor thrombosis, extrahepatic metastasis, and refractory to TACE. However, there is no specific information on efficacy and safety, such as overall survival (OS), progression-free survival (PFS), and adverse events of patients with advanced HCC after HAIC in clinical practice. Thus, our aim was to determine the clinical efficacy and safety of HAIC as first-line therapy for advanced HCC in consideration of Child-Pugh class.
PATIENTS AND METHODS
Patients
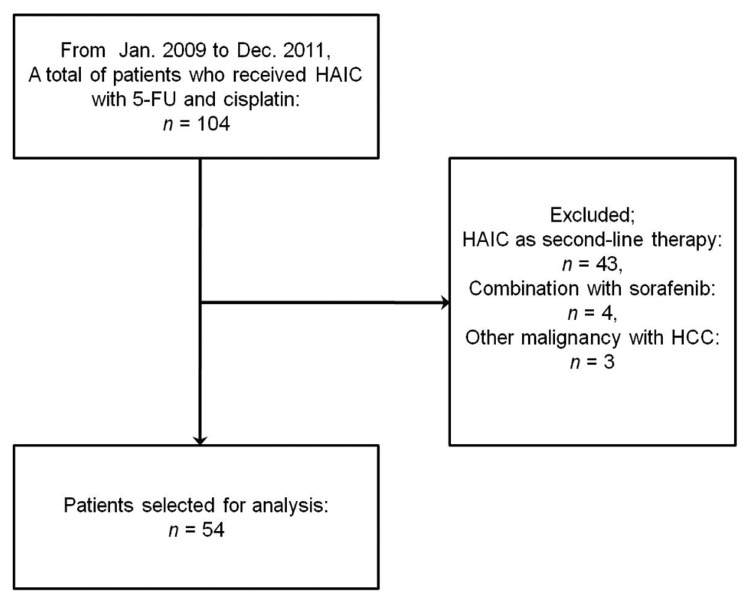
This study was conducted as a retrospective cohort study. Between January 2009 and December 2011, a total of 104 patients received HAIC with 5-FU (750 mg/m2) and cisplatin (25 mg/m2) on days 1-4 every four weeks via an implantable port system for advanced HCC at Yeungnam University Hospital. Of these 104 patients, a total of 54 patients who received HAIC exclusively as a palliative therapy were selected for this study (Fig. 1). All of the selected subjects had advanced HCC at the time of diagnosis (Barcelona Clinic Liver Cancer (BCLC) stage C: n=54), and were older than 18 years of age.13,14 The diagnosis of HCC was made either by histopathologic confirmation or typical radiologic appearance on two dynamic imaging modalities, or via one dynamic imaging examination with elevated serum alpha-fetoprotein (>400 ng/mL). We performed a retrospective review of all medical records, investigated the clinical efficacy of HAIC for advanced HCC divided into Child-Pugh class A and Child-Pugh class B/C, and evaluated safety through the toxicities or adverse events of HAIC.
This study was conducted in accordance with the 1975 Declaration of Helsinki. All subjects submitted written informed consent prior to enrollment in the study. Details of this study were approved by the Institutional Review Board of Yeungnam University Hospital (YUH-13-0341-O19).
Implantation of the drug port system
Under local anesthesia, the Seldinger method was used to gain access to the right femoral artery. Arteriography of the celiac trunk and superior mesenteric artery was performed in order to confirm portal vein patency, and arterial vascularization of the liver. After detection of tumor location and the main supplying hepatic artery, a 5.8-F indwelling intraarterial catheter was inserted, and the tip of the catheter was positioned at the common hepatic or proper hepatic artery under fluoroscopic guidance. The gastroduodenal artery was embolized using a coil to avoid formation of an ulcer as a result of efflux of the chemocytotoxic agents into the stomach or duodenum. The proximal end of the catheter was placed at the injection port and the device was subcutaneously implanted in the right thigh. To prevent occlusion of the catheter, 10 mL (10,000 units) of a heparin solution was infused via the port system for every cycle of chemotherapy.
Definition
Liver cirrhosis was defined by histologic, clinical, or radiological evidence. Clinical signs of liver cirrhosis included lower platelet count (<1.4├Ś105 cells/┬ĄL), the existence of varix or ascites, and the occurrence of encephalopathy. The gross type of tumor was classified by enhanced abdominal CT and angiography as diffuse, massive, and nodular type according to Eggel's classification. Responder was defined as a patient who achieved complete or partial response by HAIC according to radiologic examination, and non-responder was defined as a patient who achieved stable disease, progressive disease or no evaluation after HAIC.
Treatment protocol
The patients received treatment with 5-FU and cisplatin. 5-FU (750 mg/m2) was diluted with 5% dextrose in water and 200 mL was administered over two hours through a portable infusion pump from days 1 to 4. Cisplatin (25 mg/m2) was diluted with normal saline and 200 mL was infused over one hour using an intra-arterial catheter from days 1 to 4. The cycle of chemotherapy was every four weeks. To prevent cisplatin-associated nephrotoxicity, 1,000 mL of half-saline solution mixed with 20 mEq KCl and 8 mEq MgSO4 was given over three hours before and after administration of cisplatin, respectively. This treatment was continued until radiologic and clinical disease progression or development of intolerable adverse events.
Assessment of treatment for HCC was performed after every two cycles of HAIC through dynamic contrast-enhanced abdominal CT scan or gadolinium-enhanced magnetic resonance imaging using the modified Response Evaluation Criteria in Solid Tumors (mRECIST) for HCC. Concomitant antiviral therapy was allowed. If the adverse events by HAIC were grade 3 or 4, the dosage of sequential chemotherapeutic agents was reduced to 75% of the original dosage. In addition, after reduction of the dose, in the case of additional development of grade 3 or 4 toxicities, the patients were regarded as having intolerance to HAIC and were withdrawn from this therapy.
Outcomes and assessments
The primary outcomes of this study were to evaluated OS and PFS after HAIC for advanced HCC according to Child-Pugh class. OS was measured as the time interval from the initiation of treatment of HAIC to death or the last follow-up visit. PFS was measured as the time interval between the date of the first cycle of HAIC and the date that disease progression or any cause of death was first observed. Secondary outcomes included the response rate, and safety or adverse events developed by HAIC. Response rate was defined as the proportion of patients who had a best response rating of complete or partial responses over total responses after HAIC according to mRECIST. Safety was assessed in all patients using the National Cancer Institute's Common Terminology Criteria for Adverse Events (NCI-CTC AE) version 4.0. All of the selected patients were followed up at least every four weeks, and the evaluation for adverse events was performed prior to initiation of a new cycle. The evaluation included checking bone marrow reserve through complete blood count and differential cell count, liver function test, and renal function test, as well as physical examination, vital signs, and clinical manifestations.
Statistical analysis
Categorical data or frequency data were presented as absolute values and percentages, whereas continuous data were presented as mean┬▒standard deviation. Categorical data were analyzed by Pearson Žć2 test or Fisher's exact test, and continuous data were analyzed using Student t-test; if it was parametric, or not, the Mann-Whitney U test was used. Univariate and multivariate analyses of independent factors of the response to HAIC were assessed using binary logistic regression analysis. The Kaplan-Meier method was used for univariate analysis of OS and PFS and differences among groups were analyzed using the log-rank test. Multivariate analysis of the factors that influenced survival was performed using the Cox proportional hazards model. All P-values were two-sided, and a P-value <0.05 was considered statistically significant. Microsoft Excel 2007 (Microsoft Corp., Redmond, Washington, USA) was used for organization of all data, and PAWS statistics version 18.0 for Windows (SPSS Inc., Chicago, Illinois, USA) was used for analysis of data.
RESULTS
Patients characteristics
Median age of selected patients was 59.0 years (range: 39-78 years). Male was predominant (85.2%). Hepatitis B virus infection was the most common cause of HCC (70.4%). Other parameters of baseline characteristics are shown in Table 1. At the time of diagnosis of HCC, BCLC stage of enrolled patients was all stage C. However, after implantation of the drug port system, the liver function of some patients showed deterioration. As a result, BCLC stage of selected patients was changed into stage C (94.4%), and stage D (5.6%). In addition, Child-Pugh class was changed as shown in Table 1. All the analyses were performed according to staging and classification changed after implantation of the port system or at the time of initiation of HAIC. Mean interval between the time of diagnosis of HCC and the time of initiation of HAIC was 7.3┬▒5.2 days.
Treatment outcomes
Mean cycles of HAIC was 4.0┬▒2.8 times. Mean dose of 5-FU and cisplatin for each cycle was 3,683.9┬▒1,306.3 mg and 126.5┬▒43.1 mg, respectively. The cumulative total dose of anticancer agents was 14,895.6┬▒12,855.7 mg (range: 457-54,838 mg) for 5-FU, and 512.2┬▒440.1 mg (range: 18-1,824 mg) for cisplatin, respectively. Mean follow-up duration of the selected subjects was 8.1┬▒6.7 months. Median OS and PFS of enrolled patients were 5.1 months (95% confidence interval [CI]: 2.4-7.8) and 4.4 months (95% CI: 3.5-5.3), respectively.
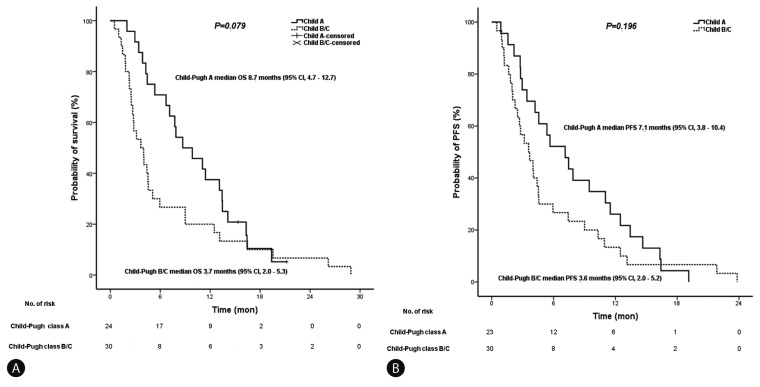
The selected patients were divided into two groups according to Child-Pugh classification; Child-Pugh A group (n=24) and Child-Pugh B/C group (n=30). A summary of baseline characteristics of each group is shown in Table 2. The median OS was 8.7 months in the Child-Pugh A group (95% CI: 4.7-12.7), and 3.7 months in the Child-Pugh B/C group (95% CI: 2.0-5.3; Fig. 2A). The median PFS was 7.1 months in the Child-Pugh A group (95% CI: 3.8-10.4), and 3.6 months in the Child-Pugh B/C group (95% CI: 2.0-5.2; Fig 2B), respectively. All median OS and PFS in both groups were not statistically significant (P=0.079, P=0.196 by log-rank test, Table 3). In addition, other parameters such as portal vein invasion and the existence of ascites were not significantly related to the OS and PFS after HAIC (P>0.05 by log-rank test).
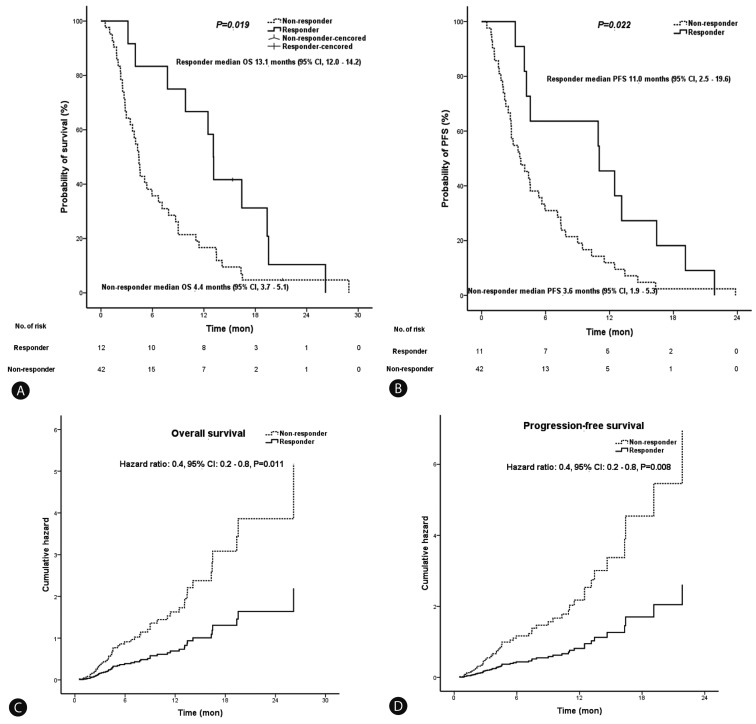
In total, although 12 patients (22.2%) showed partial responses, no complete response after HAIC for advanced HCC was observed. The best objective therapeutic responses according to mRECIST were not significantly different between the Child-Pugh A group and Child-Pugh B/C group (P=0.979). According to other parameters as well as Child-Pugh class, the best therapeutic responses by HAIC were analyzed in comparison (Table 4). Although other parameters including BCLC stage were not statistically different from the response rates, significant difference was exclusively observed in modified Union for International Cancer Control (UICC) stage (P=0.025). In addition, median OS was not statistically longer in patients who achieved complete response or partial response (responders), compared with other patients (non-responders) in the Child-Pugh A group (13.1 vs. 7.1 months, P=0.120) and the Child-Pugh B/C group (12.5 vs. 2.8 months, P=0.075). Median PFS was not significantly different between responders and non-responders in the Child-Pugh A group (11.0 vs. 5.7 months, P=0.089). However, statistical difference was observed between patients in the Child-Pugh B/C group (10.9 vs. 2.7 months, P=0.042). Considering all of the selected subjects, median OS and PFS were statistically different between responders and non-responders (13.1 vs. 4.4 months, P=0.019; 11.0 vs. 3.6 months, P=0.022). In addition, according to the Cox proportional hazards model, achievement of complete or partial response after HAIC was an independent prognostic factor of OS and PFS (hazard ratio [HR]: 0.4, 95% CI: 0.2-0.8, P=0.011, HR: 0.4, 95% CI: 0.2-0.8, P=0.008) (Fig. 3). Subgroup analyses were performed by dividing the selected subjects into responders and non-responders in order to investigate independent factors related to achievement of a complete or partial response after HAIC. Results of comparative analyses between each group are shown in Table 5. Dose of 5-FU and cisplatin per cycle showed significant difference between the two groups, respectively (P=0.007, P=0.001). According to results of binary logistic regression analysis, dose of cisplatin per cycle was an exclusively independent factor for achievement of a complete or partial response after HAIC (odds ratio: 1.039, 95% CI: 1.0-1.1, P=0.008).
Adverse events
HAIC-related adverse events such as neutropenia (79.2 vs. 83.3%), anemia (95.8 vs. 100%), thrombocytopenia (91.7 vs. 90.0%), elevated aminotransferase (100 vs. 100%), hyperbilirubinemia (91.7 vs. 96.7%), elevated creatinine (33.3 vs. 60.0%), nausea/vomiting (54.2 vs. 63.3%), diarrhea (25.0 vs. 33.3%), and fever (58.3 vs. 63.3%) occurred between the Child-Pugh A group and the Child-Pugh B/C group, irrespective of NCI-CTC AE grading (Table 6). The incidence rate of common adverse events was not significantly different between the two groups (P>0.05). In addition, the incidence rate of serious adverse events over grade 3 for each category of the toxicities did not statistically differ between the two groups (P>0.05). Serious adverse events Ōēźgrade 3 occurred frequently in both groups (83.3 vs. 96.7%, P=0.159). Although dose reduction rates by adverse events were not statistically significant between the two groups (33.3 vs. 26.7%, P=0.765), withdrawal rate significantly differed between the each group (16.7 vs. 43.3%, P=0.044). In total, seventeen patients withdrew from HAIC because of general weakness (64.7%), catheter-related complications (17.6%), and other causes (17.6%). Mean cycles of the patients who withdrew from HAIC was 2.5┬▒2.0 times. Median OS of these patients was only 3.2 months (95% CI: 1.3-5.0).
In this study, 28 patients (51.9%) experienced catheter-related complications. Of these, 22 patients (78.6%) experienced bleeding or hematoma after implantation of the drug delivery system, which did not require a transfusion; and catheter occlusion occurred in three patients (10.7%), which was resolved by thrombolytics or catheter exchange. The remaining two patients and one patient developed catheter-related infection, and extravasation, respectively. Catheter-related infection or cellulitis around the infusion port was cured completely with administration of antibiotics, wound dressing, and removal of the drug port system.
DISCUSSION
In this study, the median OS and PFS of patients with Child-Pugh class A were only 8.7 months and 7.1 months. According to findings of the SHARP trial (Sorafenib HCC Assessment Randomized Protocol), the median OS and PFS were 10.7 months and 5.5 months in patients who received treatment with sorafenib (Their liver functions were all Child-Pugh class A).15 In addition, a multinational phase III, randomized, double-blind, placebo-controlled trial to assess the efficacy and safety of sorafenib in patients from the Asian-Pacific region with advanced HCC (ClinicalTrials.gov, number NCT00492752) showed median OS (6.5 months), and PFS (2.8 months) for advanced HCC after sorafenib therapy, respectively.16 Basically, there was some difference between our study and the SHARP trial. In the current study, of enrolled patients, most patients (94.4%) were stage C of BCLC including three patients (5.6%) with stage D of BCLC. However, in the SHARP trial, most patients (82%) were stage C of BCLC, and patients (18%) with stage B of BCLC were also included. In the SHARP trial, hepatitis C infection (29%) and alcohol intake (26%) were the common causes of HCC. In contrast, in our study, hepatitis B infection (70.4%) was the most common cause. Compared to the Asian-Pacific trial, some similarities were revealed: BCLC stages of the enrolled patients were almost stage C, the most common cause of HCC was HBV infection (70.4 vs. 70.7%), and both studies were conducted as a first-line therapy for advanced HCC. However, regardless of these difference and similarities, it is difficult to make a direct comparison for survival benefits among our study and the two trials, because our study was not a large-scaled, randomized controlled trial, but a retrospective study with small subjects. The exclusively definite fact was that the OS and PFS of patients treated with HAIC as a first-line therapy were comparable to those of patients treated with sorafenib in the two trials. Thus, HAIC may be useful as an alternative option for treatment of advanced HCC.
HAIC for advanced HCC has been widely used in many Asian countries, including Korea and Japan. Several previous studies have reported on the survival benefit of HAIC using 5-FU and cisplatin, with a response rate ranging from 12.2 to 52%.17-22 The response rate (22.2%) of patients enrolled in our study was comparable to those of other previous studies for HAIC in patients with advanced HCC. As mentioned above, in this study, the median OS of responders was significantly longer than that of non-responders (13.1 vs. 4.4 months, P=0.019). Furthermore, the median PFS of responders was statistically different from that of non-responders (11.0 vs. 3.6 months, P=0.022). Achievement of complete or partial response after HAIC was an independent prognostic factor of OS and PFS (HR: 0.4, 95% CI: 0.2-0.8, P=0.011, HR: 0.4, 95% CI: 0.2-0.8, P=0.008). Therefore, better prognoses may be predicted for patients with more than partial response after HAIC for advanced HCC. In addition, in order to achieve results of complete response or partial response after HAIC, increase or maintenance of dose of cisplatin per cycle may be critical in practice.
In present study, although median OS and PFS of patients with Child-Pugh class A after HAIC for advanced HCC were longer than those of patients with Child-Pugh class B/C (8.7 vs. 3.7 months, 7.1 vs. 3.6 months), no statistical significance was observed. Our data may support the ability to treat patients with HAIC for advanced HCC irrespective of Child-Pugh classification. However, regardless of statistical significance, there was a definite difference of duration. Thus, in clinical practice, HAIC should be administered with caution in patients with advanced HCC of Child-Pugh class B/C.
All patients in our cohort study experienced at least one or more adverse events. Toxicity profile as well as severe adverse events above grade 3 appeared to be at least comparable in all of the patients independent of Child-Pugh status. In general, patients with Child-Pugh class B/C seemed to experience more adverse events and serious complications due to poorer hepatic reserve. However, the occurrence of adverse events between Child-Pugh A group and B/C group was not significantly different in real world. The reason may be associated with direct administration of 5-FU via the hepatic artery. 5-FU, which is a mainstay of HAIC therapy, is a cytotoxic agent known to inhibit deoxyribonucleic acid synthases. 5-FU is also known to exacerbate liver damage by causing liver fibrosis.23 In addition, 17 patients (31.5%) were withdrawn during the course of HAIC therapy. Most patients (64.7%) gave up the treatment by themselves due to general weakness or malaise. This is a critical problem for continuity of care. Psychological or emotional status of patients as well as therapy-related complications or adverse events may in some way influence the withdrawal of HAIC. The definite cause of this problem is still unclear. In order to improve the clinical efficacy of HAIC, we should try to determine a solution for withdrawal from HAIC.
Insertion of a drug port system for HAIC can cause certain problems. Implantation of the drug port system may have potential risk of causing damage to the vascular endothelium with the catheter. In some cases, administration of cytotoxic agents may be impossible due to dislocation of the catheter or damage to the artery. One study reported that 2.6% of patients who received treatment with HAIC experienced mild cerebral infarction.11 However, in this study, 28 patients (51.9%) developed catheter-related complications. Bleeding or hematoma occurred most often after implantation of the drug delivery systems (78.6%). The hemorrhages were minor, requiring only compression, not transfusion. In addition, all the catheter-related occlusion and infection were resolved through medical treatments as well as interventions.
There are a few limitations in our study. First, this study was conducted with a small number of patients in a single center, and had a retrospective study design. In addition, this study did not include a control group. Thus, the current study might have a selection bias. In some patients, the assessment of treatment response after HAIC was not performed, which might influence the results of our study. Thus, we could not definitely confirm the survival benefits of HAIC for advanced HCC. Some adverse events based on clinical symptoms or complaints except laboratory results such as liver function tests might be inaccurate or subjective because the investigation for adverse events only depended on reviewing the medical records.
In conclusion, our study showed that HAIC-related median OS and PFS of patients with Child-Pugh class A were longer than those of patients with Child-Pugh class B/C, in spite of no statistical significance (8.7 vs. 3.7 months, 7.1 vs. 3.6 months). In brief, Child-Pugh class B/C might be marginally associated with poor OS after HAIC for advanced HCC (P=0.078). All subjects developed HAIC-related adverse events including serious adverse events Ōēźgrade 3, however, no significant difference was observed with regard to Child-Pugh classification. Thus, HAIC should be administered cautiously in patients with Child-Pugh class B/C, because of a relatively low survival and high incidence of serious adverse events. In addition, our data demonstrated that achievement of complete or partial response after HAIC could be associated with better OS and PFS of patients with advanced HCC. HAIC is not yet a standardized therapeutic modality for advanced HCC. Large randomized trials for HAIC are still lacking, compared with the SHARP trial and the Asian-Pacific trial for sorafenib. Conduct of further large-scaled and prospective studies will be needed in order to investigate clinical efficacy and safety of HAIC for intractable advanced HCC.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




