


PREAMBLE
Background and Aims
Clinical practice guidelines for the management of chronic hepatitis B (CHB) were originally published in 2004 by the Korean Association for the Study of the Liver (KASL) in order to provide specific medical information regarding CHB that would facilitate treatment of infected patients. Other than an update on treatment of antiviral resistance in 2014, which is a partial revision, the guidelines for the treatment of CHB have been revised entirely three times in 2007, 2011, and 2015. The Asian-Pacific Association for the Study of the Liver (APASL), the European Association for the Study of the Liver (EASL), and the American Association for the Study of Liver Diseases (AASLD) also presented and continued to revise their clinical practice guidelines, and the latest updates were in 2015, 2017, and 2018. However, since the medical environment in each country is somewhat different depending on race, region, institution, and economic conditions, it is necessary to revise the Korean guidelines to reflect our medical environment and research results.
The clinical practice guidelines committee has begun revising guidelines to reflect the results of Korean and international research published since the revision of the KASL clinical practice guidelines for management of CHB in 2015 and to develop new recommendations. In particular, recent information on newly available antiviral agents has been added, and the goals and the aims of treatment as well as starting and cessation of treatment have been clearly defined. The present guidelines also summarize updates for management of drug resistance, partial virological response, and side effects. In addition, additional data on the topics of epidemiology, prevention, natural history, diagnosis, monitoring, and management of CHB in specific situations are reflected in this update. Expert opinions were solicited in cases of insufficient data to make definitive conclusions. However, as the guidelines do not represent a standard treatment protocol, clinicians should keep in mind that the best management may vary depending on the individual patient.
Target population
Patients newly diagnosed with CHB and those previously diagnosed and treated are the primary target population for these guidelines. In addition, the guidelines have been designed to help manage patients with CHB and those with other special conditions such as hepatocellular carcinoma (HCC), renal dysfunction, metabolic bone disease, immunosuppression, anticancer chemotherapy, liver/non-liver organ transplantation, or co-infections with other viruses such as hepatitis C virus (HCV), human immunodeficiency virus (HIV), or hepatitis delta virus (HDV). Guidelines for pregnant women or those who are preparing for pregnancy, as well as children and adolescents are also presented separately.
Readership
These guidelines aim to provide useful information and medical guidelines for clinicians responsible for the diagnosis and treatment of patients with CHB in Korea. It is also intended to provide practical and educational information for residents, fellows, and their supervisors.
Information about the committee and funds
The Committee for the Revision of Clinical Practice Guidelines for CHB 2018, launched in accordance with the initiative of the Board of Directors of the KASL and approved by the council, was composed of ten hepatologists. In addition, specialists representing the Korean Pediatric Society, Korean Society of Infectious Diseases, and Korean Society for Transplantation were invited to participate as external consultants. The cost of revising the guidelines was covered by the KASL.
Collection of evidence
The committee searched newly published articles related to hepatitis B from PubMed, MEDLINE (up to 2018), and KoreaMed since publication of the 2015 guidelines and systematically reviewed these articles to recommend updated clinical guidelines based on the latest medical data. In addition, we searched abstracts and proceedings of academic conferences in Korea and abroad and collected necessary data. The language of the related literature was limited to articles published in English and Korean, and the search terms included “hepatitis B,” “hepatitis B virus (HBV),” “chronic hepatitis.” Other keywords covered clinically important topics related to epidemiology, natural history, prevention, diagnosis and initial evaluation, treatment goals and aims, treatment targets and strategies, drugs, monitoring, and antiviral resistance, as well as special situations.
Levels of evidence and grades of recommendation
The collected data were analyzed through a systematic review, and the levels of evidence were classified by the revised Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system. The levels of evidence were based on the possibility of change in the estimate of clinical effect by further research, and were described as high (A), moderate (B) or low (C). Classification of grades of recommendation were either strong (1) or weak (2), by the GRADE system, according to the level of evidence, generalizability, the clinical effect of the research result, and socioeconomic aspects. Each recommendation is combined with the level of relevant evidence (A-C) and corresponding recommendation grade (1, 2) as follows: A1, A2, B1, B2, C1, C2 (Table 1).
List of the clinical questions
The committee listed clinical questions related to CHB treatment that were addressed in the main text and the recommendations (Supplementary Material).
Review of the manuscript
Initial drafts of the revised guidelines were thoroughly reviewed and agreed upon over the course of several committee meetings. An updated manuscript was reviewed at a meeting of the advisory board and opened to a public hearing where KASL members, members of related organizations, and representatives from patient associations attended. After further modification prior to publication, the final manuscript was approved by the Board of Directors of the KASL.
Announcement of the revised guidelines
The revised CHB guidelines were released on November 24, 2018. The Korean version can be found on the KASL website (http://www.kasl.org).
EPIDEMIOLOGY
Of the 3.5 billion patients who suffer from CHB worldwide, 600,000 die from related diseases annually [1]. In Korea, the hepatitis B surface antigen (HBsAg)-positive rate was high — up to 10% — in the 1980s. After introduction of HBV vaccinations in 1983, HBsAg-positivity rates dropped significantly to 3% by 2008. However, the most common etiologies of liver cirrhosis and/or HCC are related to HBV, and CHB remains prevalent even in the late 2010s [2,3].
NATURAL HISTORY
CHB is defined as persistence of serum HBsAg for more than 6 months. The natural course consists of five phases: immune-tolerant, hepatitis B e antigen (HBeAg)-positive immune-active, immune-inactive, HBeAg-negative immune-active, and HBsAg loss (Table 2). Duration of these phases varies, sequences of phases are not continuous in patients, and there can be a gray zone in which the features are not compatible with any specific phase. Therefore, assigning phases of infection or making a decision regarding antiviral treatment based on a single alanine aminotransferase (ALT) and HBV DNA is insufficient (Fig. 1) [4].
Immunological features of CHB during five phases
CHB, immune-tolerant phase (Immune-tolerant CHB) In cases of perinatal infection, the immune-tolerant phase is characterized by HBeAg positivity, very high levels of serum HBV DNA (generally ≥107 IU/mL), persistently normal levels of ALT, and minimal or no liver necroinflammation [5,6]. In a follow-up of immune-tolerant CHB patients, serum ALT was elevated in 16% of cases, and the follow-up fibrosis stage was not different from the initial stage in those who remained in the immune-tolerant phase for five years [5]. In another study from Taiwan, 5% of 240 immunetolerant CHB patients progressed to liver cirrhosis and did not develop HCC in 10 years of follow-up [7]. However, there was a small in vitro study that suggested early hepatocarcinogenesis could be underway even during the immune-tolerant phase, as was evident by a high level of HBV DNA integration and clonal hepatocyte expansion [8]. Further studies are needed to confirm these issues.
The immune-tolerant phase can last for more than three decades in patients infected with HBV genotype C due to late HBeAg seroconversion. Therefore, many female patients infected with this genotype are in the immune-tolerant phase when they are of childbearing age, which can lead to vertical transmission of HBV to a child [9].
HBeAg-positive CHB, immune-active phase (Immuneactive HBeAg-positive CHB)
With increasing age, most patients in the immune-tolerant phase experience immune responses to HBV. Such changes are due to increased response of cytotoxic T lymphocytes to hepatitis B core antigen (HBcAg) and HBeAg [10], resulting in destruction of infected hepatocytes. This phase is characterized by HBeAg positivity and fluctuating courses of serum ALT and HBV DNA levels [11,12]. Histological findings reveal moderate-to-severe necroinflammation [13]. There can be various stages of liver fibrosis according to the severity of liver injury.
Once HBeAg seroconversion occurs, the natural course of the disease may have one of three clinical features: (1) repeated HBeAg reversion and seroconversion, (2) an immune-inactive phase of CHB, or (3) HBeAg-negative CHB [14,15]. Typically, 10–40% of patients who experience seroconversion revert to an HBeAgpositive state and then experience recurrence of seroconversion at least once with progression of hepatitis activity [16,17]. In particular, reversion frequently occurs in patients with HBV genotype C, and the rate decreases with age [9]. Hepatic decompensation, which occurs in 5% of patients with acute exacerbation, may be fatal [18].
CHB, immune-inactive phase (Immune-inactive CHB)
Most patients who seroconvert during the immune-active phase progress to the immune-inactive phase, which is characterized by HBeAg negativity, antibody to hepatitis B e antigen (anti-HBe) positivity, persistent normal ALT levels, and HBV DNA levels below 2,000 IU/mL [19-21]. Typical histological findings in the third phase are mild liver inflammation [19], and various stages of liver fibrosis can reflect previous liver injury [22].
This phase persists for an extended period in most patients, but with a relatively good prognosis. However, an estimated 20% of such patients will return to the HBeAg-negative or HBeAg-positive immune-active phase, and may experience recurring periods of reactivation and inactivation throughout their lives, which can lead to cirrhosis or HCC [23,24].
HBeAg-negative CHB, immune-active phase (Immuneactive HBeAg-negative CHB)
Approximately 20% of patients who experience HBeAg seroconversion during their immune-active HBeAg-positive phase progress to the immune-active HBeAg-negative phase, with HBV DNA levels ≥2,000 IU/mL, increased ALT levels, and active necroinflammation of liver [15]. These patients show HBeAg negativity because they harbor HBV variants in the precore (PC) or basal core promoter (BCP) regions of HBV DNA, resulting in failure to produce HBeAg [25-27]. The immune-active HBeAg-negative phase is associated with older age and low rates of prolonged spontaneous disease remission, and most patients in this phase will experience persistent hepatocellular inflammation and progress to hepatic fibrosis and cirrhosis [27-29]. Severe fluctuations of HBV DNA and ALT levels can make it difficult to differentiate these patients from those in the immune-inactive phase [30].
HBsAg loss phase (Resolved CHB)
Patients in the immune-inactive phase subsequently progress to the HBsAg loss or clearance phase at a rate of 1–2% annually [30-32]. According to Liaw’s prospective data, HBsAg loss occurs in 0.5% of CHB patients per year, and 0.8% of asymptomatic chronic HBV carriers per year [33]. Korean patients reportedly experience a relatively low rate of HBsAg loss (0.4% annually) [34]. In a few patients, serum HBV DNA can be detected at a very low titer during this phase. HBsAg loss is the state of functional cure, and it is associated with a reduced risk of cirrhosis. However, significant risk of HCC development remains even after HBsAg loss in male patients, and in settings where HBsAg loss has been achieved late (presence of cirrhosis or age ≥50 years) [35,36].
Risk factors that influence the natural history and progression of liver disease in CHB
In Korea, the reported annual and five-year accumulated incidences of cirrhosis are 5.1% and 23%, respectively, while those for HCC are 0.8% and 3% [37]. The risk factors for hepatitis B progressing to cirrhosis or HCC can be divided into host, viral, socialenvironmental factors (Table 3). For host factors, cirrhosis, persistent necroinflammation, old age, male gender, family history of HCC, co-infection of other hepatitis virus or HIV affects the risk [17]. High levels of serum HBV DNA and/or serum HBsAg, HBV genotype C, and specific genotypic mutations are included in viral factors [38-47]. Social-environmental factors for progression to cirrhosis or HCC include alcohol consumption, metabolic syndrome, diabetes, obesity, and smoking [17,46]. In contrast, coffee [48-50], metformin [51], aspirin [52,53] and statins [54-59] exert protective effects against the development of HCC.
Multiple prognostic prediction models have been developed to estimate the risk of HCC development in CHB patients. The Risk Estimation for Hepatocellular Carcinoma in Chronic Hepatitis B (REACH-B) model, which consists of gender, age, serum ALT, HBeAg, and serum HBV DNA levels, has been developed for HCC risk prediction in non-liver cirrhosis, treatment-naïve CHB patients. REACH-B model has been validated in Hong Kong and Korean cohort of CHB patients including liver cirrhosis. Areas under the receiver operating characteristic curve (AUROCs) for HCC prediction at 3 years, 5 years, and 10 years are 0.77–0.81 in those cohort [60]. A modified REACH-B model, which substituted serum HBV DNA for the liver stiffness value from the original REACH-B model, showed better outcomes in assessment of three-year and five-year HCC prediction in several prospective Korean studies [61,62]. Meanwhile, the PAGE-B (platelets, age, gender, and hepatitis B scores) model, which was developed from Western studies [63], has been validated by several Korean retrospective studies [64,65]. Modified PAGE-B (adding serum albumin) was superior to original PAGE-B in the prediction of five-year HCC risk in Korean CHB patients [65].
PREVENTION
The following section describes methods for avoiding new HBV infection in non-infected persons, and for minimizing the risk of disease progression and development of complications in CHB patients.
HBV non-infected persons
Because chronic HBV infection is endemic in Korea, any person at high risk for liver disease or with suspected liver disease is recommended to have their HBsAg and antibody to hepatitis B surface antigen (anti-HBs) statuses checked [66,67]. For individuals negative for HBsAg and anti-HBs (<10 mIU/mL), and who have not been vaccinated, hepatitis B vaccination is recommended. In particular, 1) patients with chronic liver diseases such as HCV infection, alcohol-related liver disease, fatty liver disease, autoimmune hepatitis, and cirrhosis, as well as those with elevated ALT or aspartate aminotransferase (AST) of unknown etiology [68], and 2) patients at increased risk of HBV infection, such as healthcare workers, inmates and staff at correctional facilities, residents and staff of facilities for the developmentally disabled, household members and sexual partners of HBsAg-positive persons, hemodialysis patients, persons who inject drugs, those at risk for sexually transmitted diseases, and HIV-coinfected patients should be vaccinated for hepatitis B [67].
The three doses constituting the hepatitis B vaccine series administered intramuscularly at birth and 1 and 6 months induce a protective antibody response (anti-HBs >10 mIU/mL) in >90% of recipients. Most non-responders (44–100%) subsequently respond to a further three-dose vaccination [69,70]. Although serological testing for anti-HBs is not necessary after routine vaccination in immunocompetent adults, post-vaccination testing of anti-HBs status is recommended in some subjects, such as newborns of HBV-infected mothers or nine- to 18-month-old infants with family members with CHB, healthcare workers, dialysis patients, workers in dialysis units and operation rooms, immunocompromised subjects (e.g., HIV infected individuals, hematopoietic stem cell transplant (HSCT) recipients, patients undergoing chemotherapy), and sexual partners of patients with chronic HBV infection should be tested 1–2 months after completion of the HBV immunization series [69,70]. While anti-HBs levels can decline or disappear over several decades, vaccinated subjects remain protected against HBV infection and there is no need for booster vaccinations in immunocompetent individuals. However, an anti-HBs level of <10 mIU/mL in dialysis patients indicates an increased risk of HBV infection, and a booster vaccination is needed if annual testing reveals an anti-HBs level of <10 mIU/mL [70]. This also applies to immunocompromised patients [69,70].
A person without protective anti-HBs exposed to HBV-contaminated blood or body fluids should receive hepatitis B immunoglobulin (HBIG, 0.06 mL/kg) and the hepatitis B vaccine as soon as possible; preferably within 24 hours, otherwise post-exposure prophylaxis should be initiated within seven days for percutaneous exposure or within 14 days for sexual exposure [71]. Sexual partners who have not been tested for HBV serological markers, have not completed the full immunization series, or who are negative for anti-HBs should use barrier protection methods, such as condoms.
As HBV is endemic in Korea, the most common etiology of isolated antibody to hepatitis B core antigen (anti-HBc)-positive patients who are negative for HBsAg and anti-HBs is past HBV infection. They rarely require immunization, but those who are at increased risk of HBV infection should be vaccinated for HBV [72,73]. Isolated anti-HBc positive patients with abnormal liver function results should be considered for the possibility of serum HBV DNA detection.
Patients with chronic HBV infection
Chronically HBV-infected patients are not the indication for HBV vaccination. Co-infection with hepatitis A in HBV carriers increases the risk of mortality 5.6- to 29-fold [74]. Therefore, hepatitis A vaccination is recommended for persons negative for the protective hepatitis A virus antibody immunoglobulin G (anti-HAV IgG) [75].
CHB patients can transmit the virus to others, and should be counseled regarding how to modify their lifestyle to prevent HBV transmission. Mother-to-child transmission (MTCT) is the most important route of HBV infection. Refer to “Pregnant women or women preparing for pregnancy” sections in the “Management in Special Conditions” chapter, for details on antiviral treatment during pregnancy to prevent MTCT. HBIG and vaccination after delivery can prevent 90–95% of transmission to newborns from HBsAg-positive mothers [76,77]. Such infants should receive 0.5 mL HBIG and start the HBV vaccination series within 12 hours of birth.
The rates of HBV infection among newborns from HBsAg-positive mothers were not different between breast- and formulafeeding (0–8% vs. 3–9%, respectively) [78,79].
Chronic alcohol consumption is an independent risk factor for cirrhosis and HCC, and even more harmful in patients with chronic liver diseases [80]. Abstinence from alcohol is recommended in patients with chronic HBV infection [81].
According to several retrospective studies, smoking is associated with HCC development [82,83], and the risk of HCC development is much higher in smoking CHB patients with metabolic syndrome [84].
No specific dietary measures have been shown to affect the natural course in CHB patients. However, one prospective study showed fatty liver disease is associated with fibrosis progression independent of viral factors [85]. In addition, patients with metabolic syndrome resulting from diabetes mellitus, hyperlipidemia, and obesity were associated with an increased risk of HCC development in several retrospective studies [86-88]. CHB patients should therefore be counseled on lifestyle modifications regarding metabolic syndromes.
[Recommendations]
1. If HBsAg and anti-HBs are negative, hepatitis B vaccination is recommended. (A1) However, vaccination is not necessary if anti-HBc is positive or anti-HBs was lost after past vaccination; nevertheless, vaccination may be recommended in the presence of high risk of HBV infection. (B1)
2. Newborns with HBV-infected mothers should receive HBIG and the hepatitis B vaccine at delivery and complete the recommended vaccination series. (A1)
3. The hepatitis A vaccine should be given to patients with chronic HBV infection who are negative for anti-HAV IgG. (A1)
4. Patients with chronic HBV infection should abstain from alcohol. (A1)
5. Patients with chronic HBV infection are recommended to stop smoking. (B1)
6. Patients with chronic HBV infection are recommended to maintain adequate body weight to prevent metabolic syndrome or fatty liver disease, and to manage metabolic complications including diabetes and hyperlipidemia. (B1)
DIAGNOSIS AND INITIAL EVALUATION
CHB is defined as the presence of HBsAg for longer than 6 months. The initial evaluation of CHB patients should include a thorough history and physical examination, with an emphasis on risk factors such as alcohol consumption or drug use, HAV or HCV co-infection, and a family history of chronic HBV infection and HCC. In high-risk groups, the possibility of HDV or HIV co-infection should also be considered. To establish the causal relationship between HBV infection and liver disease, comorbidities such as obesity, diabetes mellitus, and metabolic syndrome should be assessed. Appropriate longitudinal long-term follow-up is crucial for patients with CHB. Serological, virological, and biochemical tests, non-invasive liver stiffness measurement and/or liver biopsies are used to assess HBV replication and the degree of liver injury in patients with CHB.
Antigen/antibody test
HBsAg immunoassay is a necessary and accurate test for diagnosis of CHB. By definition, patients who remain positive for HBsAg for longer than 6 months are sufficient to diagnose CHB.
Serological tests, including those for anti-HBs and anti-HBc, can assist in screening populations for HBV infection and differentiating among acute, chronic, past infection and immunized individuals.
Persistently positive anti-HBc is shown when an anti-HBs titer from past HBV infection becomes undetectable over time or in cases with occult hepatitis B infection [89-92]. Patients who recover from HBV infection will be negative for HBsAg and positive for anti-HBs and anti-HBc. Patients who respond adequately to hepatitis B vaccines will be negative on anti-HBc and positive on antiHBs testing, as anti-HBc emerges only after HBV infection and persists for life.
Laboratory tests for patients with CHB should include those for HBeAg and anti-HBe. HBeAg positivity generally indicates a high level of viral replication, and anti-HBe positivity a low level. HBeAg-negative, anti-HBe-positive patients with a normal ALT level and an HBV DNA level of <2,000 IU/mL (<10,000 copies/mL) may be in the inactive phase. HBeAg-negative CHB patients have elevated ALT and an HBV DNA level of >2,000 IU/mL.
Acute hepatitis A co-infection in CHB patients can result in increased icteric manifestations, longer recovery time, and increased risk of fulminant hepatic failure. Indeed, underlying chronic liver disease is an important risk factor for fulminant hepatic failure and death in patients with acute HAV infection [93-95]. The seropositivity graph has shifted horizontally to the right for 20 years in age in the last 30 years, and there is a possibility of acute hepatitis A in all age groups [96]. Therefore, CHB patients should undergo testing for anti-HAV IgG, and all patients with a negative immune status for hepatitis A should receive the HAV vaccine. Laboratory tests should include tests for co-infection with HCV. Additionally anti-HDV, and/or anti-HIV should be tested in those who are at risk [97,98].
Biochemical tests
Assessments of the severity of liver disease should include biochemical markers such as AST, ALT, gamma glutamyltranspeptidase (GGT), alkaline phosphatase (ALP), bilirubin, albumin, and creatinine. A complete blood count (CBC), and prothrombin time should also be assessed. A progressive decline in serum albumin levels and prolongation of the prothrombin time (PT), often accompanied by a decrease in platelet count, are characteristically observed after cirrhosis develops. The serum ALT level has been commonly used in assessments of liver disease and is an important criterion for defining which patients are candidates for therapy [99]. The ALT level is usually higher than that of AST, but the ratio may be reversed when the disease progresses to cirrhosis. HBVinfected patients with normal or mildly elevated ALT levels have been thought to have no or mild necroinflammation on liver biopsy. However, there is no correlation between the degree of liver cell necrosis and ALT level [100].
Data from clinical studies have shown that the true normal level of ALT is significantly lower than the previously established limits: 40 IU/L for males and 30 IU/L for females. Moreover, data from cohort studies indicate that the upper limit of normal (ULN) ALT and AST levels should be decreased to 30 IU/L for males and 19 IU/L for females [100]. Meanwhile, according to a study in Korea involving 12,000 patients with chronic HBV infection, the best cut-off values for liver-related mortality prediction were >34 IU/L in men, and >30 IU/L in women [101]. Despite being a retrospective study, the research included various age groups (40–79 years), did not excluded the data of mild fatty liver-disease patients, and reflected realistic values of Korean patients with chronic HBV infection. Those levels were associated with liver-related mortality prediction, which is the most important issue in clinical settings. Therefore, it would be relevant to use cut-offs of ALT ≤34 IU/L in men, and ALT ≤30 IU/L in women until this issue can be clarified by further study.
Serum HBV DNA tests
Serum HBV DNA testing provides a direct measure of the level of viral replication. This quantification is essential for characterizing the status of infection, diagnosing the disease, making the decision to treat, and subsequent monitoring of patients. It is also important for predicting the risks of cirrhosis and HCC and should be applied to all patients diagnosed with CHB. The most frequently recommended method for serum HBV DNA quantification is real-time polymerase chain reaction (PCR). The introduction of the international unit (IU) as a recommended reporting unit for HBV DNA has facilitated standardized reporting and comparison of serum HBV DNA levels [103]; 1 IU/mL is equivalent to roughly 5 copies/mL, but it differs between test equipment types (Roche Diagnostics: 5.8 copies/mL, Abbott Diagnostics: 3.4 copies/mL). The same test should be utilized for each HBV DNA level test in a given patient in clinical practice to ensure consistency.
HBV genotypes
HBV genotypes appear to influence the progression of liver disease, risk of HCC, and response to therapy (including interferon therapy) [104-106]. Some studies in Asia have suggested that genotype C is associated more frequently with late HBeAg seroconversion, HBV reactivation or HBeAg seroreversion after achievement of seroconversion, severe liver disease, and HCC than is genotype B [107]. The specific genotype has also been shown to affect the response to interferon therapy, with the rate of an antiviral response to pegylated interferon (peginterferon) therapy being higher for genotypes A and B than for genotypes C and D [108].
HBV genotyping can be recommended to help identify patients who might be at greater risk of disease progression and to determine the most appropriate candidates for peginterferon therapy [109]. However, genotyping is considered unnecessary in Korea, where patients are almost exclusively infected with genotype C.
Serum HBsAg quantification
A quantitative HBsAg (qHBsAg) assay is used to indirectly assess the amount and transcriptional activity of covalently closed circular (ccc) DNA, which acts as a template for HBV transcription. HBsAg is not only generated by transcription and translation of cccDNA, but also can be generated from HBV DNA episomally integrated into the host genome. Therefore the role of qHBsAg as viral replication is more limited than serum HBV DNA [110]. However, qHBsAg can help differentiate among multiple phases of natural courses, combining HBV DNA levels in the assessment. Serum qHBsAg level is higher in HBeAg-positive patients than in HBeAgnegative patients. In HBeAg-positive patients, qHBsAg level is higher in the immune-tolerant phase than in the immune-active phase [111,112]. In HBeAg-negative patients, one-time measurement of serum HBV DNA <2,000 IU/mL and HBsAg <1,000 IU/mL is suggestive of future inactive carriers [113,114]. In contrast, among HBeAg-negative patients with lower viral loads (HBV DNA <2,000 IU/mL), HCC risk is higher in those with a high qHBsAg titer (>1,000 IU/mL) than in those with a low qHBsAg titer [115].
Additionally, the role of serum qHBsAg in prediction of ontreatment or off-treatment response has been widely studied. Serum qHBsAg was useful to predict treatment response during peginterferon therapy in HBeAg-positive patients, possibly providing a guide to stopping treatment ealier [116]. Serum qHBsAg levels were useful predictors of a sustained off-treatment response in CHB patients who were previously treated with nucleos(t)ide analogues (NA) [117,118].
Liver biopsy
Liver biopsy can be helpful in determining the degree of necroinflammation and stage of fibrosis. Although it is invasive, the rate of serious complications is very low (1/4,000–1/10,000). A liver biopsy is recommended even in CHB patients with normal ALT levels, to evaluate the need for antiviral treatment in the presence of the risk of significant liver fibrosis, such as increasing age and serum HBV DNA levels [119]. However, there are limitations in that only a small portion of the liver is sampled, leading to low intra/interobserver reliability [120]. Also, biopsy may be contraindicated in patients with bleeding tendency. Thus, it is not required when cirrhosis is clinically evident or when treatment is indicated irrespective of the grade of activity or the stage of fibrosis. The efficacy of non-invasive methods such as transient elastography (TE) or serum markers in assessing fibrosis in CHB has increased [120].
Non-invasive fibrosis tests
The severity of liver fibrosis and determination of ALT and HBV DNA levels have essential roles in treatment decisions. Non-invasive methods to estimate liver fibrosis have been developed. Commonly used serum markers are aspartate aminotransferase-platelet ratio index (APRI) and fibrosis-4 (FIB-4) index (platelets, ALT, AST, Age). FibroTest, Hepascore, FibroMeter, Enhanced Liver Fibrosis test using direct markers such as serum α-2 macroglobulin, hyaluronic acid, tissue inhibitor of metalloproteinases-1, type III procollagen aminopeptide, apolipoprotein A1, haptoglobin, L-glutamyl transpeptidase are also available [120,121].
APRI is calculated by the formula of
(AST/ULN for AST)×100/platelet count (×109/L) [122].
APRI was useful for exclusion of significant fibrosis at a low cut-off level and diagnosis of cirrhosis at a high cut-off level in several meta-analyses [123,124].
FIB-4 is calculated by the formula of age(yr)×AST (IU/L)/platelet count (×109/L)× ALT ( IU / L )
TE using Fibroscan® (Echosense, Paris, France) has a high degree of accuracy for assessment of advanced liver fibrosis. It is the most commonly used method for monitoring chronic liver disease because of its non-invasiveness and high-reproducibility [128]. TE can be performed rapidly (5 min) in outpatient clinics and yields immediate results [129,130]. However, only procedures involving ≥10 successful measurements are considered reliable. Moreover, a success rate of at least 60% and an interquartile range (IQR) of less than 30% of the median value are required (IQR/median) [131]. TE has limitations in subjects with ascites, obesity, or narrow intercostal spaces. Moreover, the system may yield false-positive results in subjects with acute hepatitis and extrahepatic biliary tract obstruction) [132-134]. In a meta-analysis from Korea, AUROCs for diagnosis of significant fibrosis (≥F2) and cirrhosis were 0.86 and 0.93, respectively, with diagnosis cut-offs for F2, F3, and F4 of 7.8 kPa, 8.8 kPa, 11.7 kPa, respectively [135]. TE (Fibroscan®; Echosense) had greater diagnostic accuracy than APRI or FIB-4 for liver cirrhosis in a study that compared liver biopsy, aspartate aminotransferase-to-alanine aminotransferase ratio, APRI, TE, and FIB-4 in patients with chronic hepatitis [136].
Newly developed non-invasive tools to assess fibrosis are acoustic radiation force impulse imaging, shear-wave elastography, real-time elastography, and magnetic resonance elastography (MRE), which needs to be further validated in large cohorts of CHB patients. MRE showed high diagnostic accuracy for biopsy-confirmed liver fibrosis in several retrospective studies [137,138] and is at least as accurate as TE for assessment of fibrosis [139-141]. MRE was more reliable in the obese patients [142].
Screening for HCC
The initial evaluation of patients with CHB should include screening tests for HCC. Periodic surveillance is also needed in these patients to ensure early detection of HCC during follow-up, irrespective of antiviral treatment. Standard tools for HCC surveillance include measuring the alfa-fetoprotein level and ultrasonography every 6 months [143]. Patients at a high risk of HCC include those older than 40 years and those with cirrhosis even when they are younger than 40. Periodic surveillance leads to a higher probability for applying curative treatment [144,145]. Magnetic resonance imaging and computed tomography may be preferred for some patients with severe cirrhosis or obesity, as ultrasonography has poor sensitivity in those conditions. The use of antiviral therapies may lower the risk or delay the progression of disease but cannot prevent all possible complications. Therefore, active surveillance for HCC is required at regular intervals for early diagnosis and treatment.
[Recommendations]
1. The initial evaluation of patients with CHB should include taking a detailed medical history and physical examination, with an emphasis on risk factors such as co-infection, alcohol consumption, and family history of HBV infection and HCC. (A1)
2. In the evaluation of CHB patients, CBC, AST, ALT, ALP, GGT, bilirubin, albumin, creatinine, prothrombin time are required. (A1)
3. HBeAg/anti-HBe and serum HBV DNA quantification should be assessed as HBV replication markers in CHB patients. The most frequently recommended method for serum HBV DNA quantification is real-time PCR. (A1)
4. IgG anti-HAV test is recommended in CHB patients. (B1)
5. In patients with CHB, an anti-HCV test is recommended to rule out HCV co-infection. (B1)
6. In patients with CHB, an anti-HDV and an anti-HIV test may be recommended to rule out HDV or HIV co-infection. (B2)
7. Liver biopsy can be performed to determine the degree of liver necroinflammation and fibrosis in CHB patients. (A2)
8. If a liver biopsy is difficult to perform in patients with CHB, non-invasive tests such as serum markers or liver elasticity measurement are recommended to assess liver fibrosis. (B1)
9. Patients with CHB should be tested for HCC regardless of hepatitis B treatment; abdominal ultrasonography and serum alfa-fetoprotein are the surveillance tools that should be performed every 6 months. (A1)
TREATMENT GOAL AND AIMS
The ultimate goals of hepatitis B treatment are to decrease mortality and increase survival by alleviating hepatic inflammation and preventing the development of fibrosis, which ultimately reduces the frequency of progression of hepatitis to liver cirrhosis or HCC [146-152]. The ultimate goals could only be achieved by eradication of HBV in the liver in the early stages of infection; however, cccDNA persists in the hepatocyte nucleus despite antiviral treatment until now, so it is difficult to expect complete elimination of HBV. Therefore, it is most important to consistently maintain complete viral suppression [153].
Since the goals of treatment can only be assessed after a substantially long-term follow-up period, alternative clinical biomarkers reflecting treatment goals may be considered when deciding to discontinue treatment. Currently, clinically available biomarkers that reflect achievement of treatment goals are ALT, HBV DNA, HBeAg, and HBsAg. Thus, ALT normalization, undetectable HBV DNA, HBeAg loss or seroconversion, and HBsAg loss or seroconversion can be used as clinical treatment aims or endpoints. Among these, serum HBsAg loss or seroconversion is the ideal endpoint of CHB treatment [154].
[Recommendations]
1. The ultimate goals of CHB treatment are to decrease mortality from liver disease and improve survival by preventing HBV replication and alleviating hepatic inflammation, and by preventing the progression of fibrosis, development of liver cirrhosis, and HCC. (A1)
2. Clinical endpoints (aims) of treatment are ALT normalization (male ≤34 IU/L, female ≤30 IU/L), undetectable serum HBV DNA, serum HBeAg loss or seroconversion, and serum HBsAg loss or seroconversion. Serum HBsAg loss or seroconversion is the ideal endpoint of hepatitis B treatment. (A1)
TREATMENT INDICATION
Active HBV replication is associated with increased risk of liver damage, progression of liver disease, and liver-related complications [22]. Nowadays, antiviral therapy has been developed that can effectively inhibit replication of the virus. Inhibition of HBV replication by antiviral therapy can improve hepatic inflammation, normalize serum ALT levels, improve liver fibrosis, reduce the incidence of HCC, and decrease liver-related death [155]. However, currently available antiviral therapies cannot eradicate or eliminate the virus. Furthermore, the efficacy and side effects of the same drug may vary depending on the clinical situation [156]. Therefore benefits and risks of antiviral therapy should be carefully evaluated on an individual basis in the context of the clinical situation. The following three factors are fundamental components that should be taken into consideration when deciding antiviral therapy: 1) The severity of liver disease, 2) the degree of HBV replication, and 3) the presence of liver injury (Fig. 2). The severity of liver disease can be categorized into chronic hepatitis, compensated cirrhosis, and decompensated cirrhosis. The degree of HBV replication can be assessed by measuring serum HBV DNA levels. The presence of liver injury can be estimated using serum ALT levels or can be assessed by a liver biopsy.
CHB, immune-tolerant phase
The immune-tolerant phase is characterized by HBeAg positivity, very high serum HBV DNA levels (usually ≥107 IU/mL), and persistently normal serum ALT levels. In this phase, long-term prognosis is excellent without antiviral therapy [67,157,158]. To verify the immune-tolerant phase, a liver biopsy is necessary and will show no or mild inflammation without fibrosis on liver biopsy. However, liver biopsy is an invasive procedure with potential complications that limit its widespread use and repetitive testing in clinical practice. Hence, in real-life clinical practice, a combination of clinical findings is typically used to define the immune-tolerant phase without liver biopsy. However, caution should be exercised considering the results of a recent study suggesting that when patients are defined as in the immune-tolerant phase by a combination of clinical findings without liver biopsy (HBeAg positive, high serum HBV DNA levels, normal ALT levels, and no evidence of cirrhosis), HCC and liver cirrhosis-related complications still occur in a considerable number of patients during long-term follow-up [159]. In several studies, older age, being male, relatively low serum HBV DNA levels, high liver stiffness value, and normal but high-normal ALT levels were factors associated with HCC development or liver-related complications among patients presumed to be in the immune-tolerant phase by combinations of clinical findings without a liver biopsy [159-161]. The immune-tolerant phase is usually observed in young adults, and is not common in elderly patients. Although other clinical findings suggest the immune-tolerant phase, liver biopsy may show significant fibrosis or necroinflammation in elderly patients [162], as age is associated with increased risk of HCC and death during follow-up [159,161]. Therefore, even when all the other clinical findings suggest the immune-tolerant phase, a liver biopsy can be considered to verify the immune-tolerant phase in older adults. An age cutoff for liver biopsy consideration was suggested to be 30–40 years [67,97]; however, evidence to support this approach is limited.
The immune-tolerant phase is also characterized by very high levels of HBV DNA, as there is little or minimal immune response to the virus [67,97]. In one study, among patients presumed to be in the immune-tolerant phase, relatively low serum HBV DNA level was associated with a higher risk of HCC and death compared to those with very high serum HBV DNA levels (≥107 IU/mL) [159,161]. Relatively low serum HBV DNA levels indicate that the immune response has already begun to suppress the virus. The immunetolerant phase is also characterized by little or no necroinflammation without liver fibrosis. Hence, significant fibrosis as seen using non-invasive serum fibrosis markers (e.g., APRI, FIB-4) or TE (Fibroscan®; Echosense) suggests that patients are not in the genuine immune-tolerant phase.
ALT is a good indicator of liver necroinflammation, so patients in the immune-tolerant phase show persistently normal ALT levels, as there is no or little liver necroinflammation. Hence, patients with slightly elevated ALT levels are more likely to have fibrosis and necroinflammation on a liver biopsy, and have a higher risk of developing complications during follow-up [161,162]. Therefore, if ALT is at the borderline of ULN or is slightly higher than ULN, this can be a sign that a patient is not genuinely in the immune-tolerant phase. However, careful interpretation is needed in defining normal or elevated ALT levels. There is controversy about what constitutes healthy, normal ALT levels. Elevation of ALT level can be caused by obesity and other conditions not related to HBV. Recently, the cutoff level for ALT associated with increased liver-related mortality among Korean chronic HBV infected patients was reported to be 34 IU/mL for men and 30 IU/mL for women.101 Therefore, the present guidelines recommend using these values to define normal ALT levels. For patients with the previously mentioned risk factors (older age, relatively low serum HBV DNA levels, non-invasive test suggesting significant fibrosis, or ALT at ULN or slight higher ULN), a liver biopsy can be considered to guide management decisions despite other clinical findings suggesting the patient is in the immune-tolerant phase.
The efficacy of currently available antiviral regimens is limited for patients in the immune-tolerant phase. Long-term treatment may be necessary and treatment discontinuation can be difficult. Antiviral treatment using NAs resulted in a poor antiviral response rate and a low HBeAg seroclearance rate [163]. Furthermore, when NA treatment was discontinued for those who started oral NA therapy at the immune-tolerant phase, all patients showed a rebound of serum HBV DNA levels above 2,000 IU/mL, 70% showed an elevation of ALT levels, and 55% had to re-start NA therapy [164]. However, in one study from Korea that compared 87 NA-treated immune-tolerant CHB patients to 397 monitored immune-tolerant patients as a control group, increased risk of HCC and cirrhosis was observed in the control group despite favorable baseline liver function [165]. This finding suggests that some patients who are presumed to be in the immune-tolerant phase may develop complications during follow-up, and that antiviral treatment may decrease the risk of developing complication. Further studies are needed to identify appropriate antiviral treatment indications in patients in the immune-tolerant phase.
[Recommendations]
1. Antiviral therapy is not indicated in CHB patients in the immune-tolerant phase, as defined by HBeAg positivity, very high serum HBV DNA level (≥107 IU/mL), persistently normal ALT level, and no inflammation or fibrosis on liver biopsy. (B1)
2. Liver biopsy can be considered for HBeAg-positive CHB patients with normal ALT levels to determine antiviral treatment if the patient’s age is ≥30–40 years old, serum HBV DNA levels are <107 IU/mL, non-invasive fibrosis tests suggest significant hepatic fibrosis, or ALT is approaching the borderline of ULN range. (B2)
HBeAg-positive and HBeAg-negative CHB, immune-active phase
The immune-active phase is characterized by active replication of HBV and moderate or severe necroinflammation with or without fibrosis. A systematic review and meta-analysis of 15 randomized controlled trials and 44 observational studies showed that antiviral treatment in the immune-active phase reduced the risk of cirrhosis, hepatic decompensation, and HCC [155]. Therefore, patients in the immune-active phase are indicated for antiviral treatment. Nevertheless, careful attention to HCC development is needed, as antiviral treatment cannot completely eliminate the risk of developing HCC [166]. A recent study from Korea reported a marked reduction in liver disease mortality by widespread use of antiviral treatments against HBV, but paradoxical increased burden of liver cancer [167].
Active replication of HBV can be confirmed by serum HBV DNA measurement using PCR. Detection of HBV DNA in the serum indicates active replication of the virus. However, the lower limit of detection is different among different HBV DNA measurement assays. Moreover, many patients with low-level viremia (serum HBV DNA level <2,000 IU/mL), shows normal ALT levels, and little or no necroinflammation or fibrosis on a liver biopsy, and show favorable outcomes without antiviral therapy [45]. Hence, not all patients with detectable serum HBV DNA, but patients with serum HBV DNA levels ≥2,000–20,000 IU/mL (10,000–100,000 copies/mL) for HBeAg-positive patients, and serum HBV DNA levels ≥2,000 IU/mL (10,000 copies/mL) for HBeAg-negative patients are considered for antiviral therapy [45,47,168].
Serum ALT is a convenient indicator of necroinflammation of the liver and can be easily used in clinical practice [169]. Elevation of ALT suggests hepatocellular injury and requires assessment and evaluation. However, the degree of ALT elevation does not always correlate with necroinflammation of the liver and can be affected by body mass index and gender [100,170]. ALT elevation can arise from alcohol use, drug use, fatty liver, and other causes unrelated to HBV [170,171], and a normal ALT level may not exclude significant liver disease [172]. Hence, the use of ALT as a criterion for treatment initiation requires consideration of what degree of ALT elevation should be regarded as a threshold to initiate treatment. If the ALT level is elevated more than ≥2 times the ULN, antiviral treatment for HBV is recommended unless the ALT is elevated by other causes [67,97]. When ALT is elevated above the ULN but <2 times the ULN, controversy exists as to whether these patients require antiviral treatment [67,97]. Patients with serum ALT elevated above the ULN but <2 times the ULN have an increased risk of liver cirrhosis and HCC compared to patients with serum ALT within the normal range [173,174]. Yet, “normal” ALT levels is defined at different cutoff between studies, and “normal” ALT levels also differs by ethnicity [170,175]. The specific ALT levels used in clinical trials to initiate antiviral therapy also differ [176-181]. Therefore, sufficient data are not available to judge whether it is necessary to start antiviral treatment in patients with serum ALT elevated above the ULN but <2 times the ULN. In this case, trends in serum ALT and HBV DNA levels should be closely monitored to identify possible causes and to verify whether treatment for such patients should be initiated. If a patient shows persistently elevated ALT levels, but those levels remain <2 times the ULN, the degree of fibrosis can be further investigated by non-invasive fibrosis tests or by liver biopsy to verify whether patients require antiviral treatment.
Histological assessment of the liver, liver biopsy, is a cornerstone in the evaluation of hepatic necroinflammation and fibrosis [182]. Findings of moderate to severe necroinflammation or significant fibrosis (≥F2) indicate that antiviral treatment for HBV is needed [156]. However, a liver biopsy is an invasive procedure requiring special resources that limit widespread clinical use. Serum fibrosis biomarkers or TE (Fibroscan®; Echosense) of liver are alternatives that can be used to estimate degree of fibrosis [183]. These non-invasive biomarkers for liver fibrosis are less accurate than liver biopsy. However, they can be used to rule in or rule out patients with significant fibrosis. Recently, treatment initiation based on liver disease severity as assessed by non-invasive tests (e.g., Fibroscan® [Echosense]), has been suggested [183]. However, evidence to support treatment initiation determined by non-invasive tests remains limited at present.
Among HBeAg-positive CHB patients, spontaneous HBeAg seroconversion has been reported for those experiencing increase of ALT level with HBV DNA elevation [184]. Hence, 3–6 months observation without antiviral treatment can be considered if spontaneous HBeAg seroconversion is expected [184]. However, biochemical deterioration leading to liver failure is of concern. A prospective cohort study of 90 patients from Korea with HBeAg-positive CHB who were monitored without antiviral therapy showed a very low rate of spontaneous HBeAg seroconversion (1.1%), while there was frequent biochemical deterioration and one case of liver transplantation due to liver failure [185]. Therefore, when expecting HBeAg seroconversion, the risk of acute decompensation leading to liver failure warrants careful attention. Another report from Korea showed that spontaneous HBeAg seroconversion can be expected for patients with non-vertical transmission and low serum HBV DNA levels [186].
CHB patients may present with severe acute exacerbation, characterized by elevated HBV DNA levels, serum ALT levels 5–10 times greater than ULN, jaundice, coagulopathy, ascites, and/or hepatic encephalopathy. They can also be classified as having acute-on-chronic liver failure (ACLF) when they present with symptoms and signs of liver failure [187]. Severe acute exacerbation can occur spontaneously [188], by drug resistant HBV during antiviral therapy [189], by stopping antiviral therapy [190], or by anticancer chemotherapy [191]. NA therapy reduces mortality in patients with severe reactivation of CHB presenting as ACLF [192]. Therefore, immediate antiviral treatment is recommended for CHB patients with severe acute exacerbation or ACLF. Some studies have reported a higher mortality rate among entecavir-treated patients than lamivudine-treated patients [193,194], but a meta-analysis of three prospective and eight retrospective studies showed similar effects on the mortality rate between entecavir and lamivudine treatment, with a more favorable long-term outcome in entecavir than lamivudine [187]. However, antiviral treatment cannot fully prevent progression to liver failure, which may lead to mortality in the case of high Model for End-stage Liver Disease (MELD) score, moderate to severe ascites, and/or aggravation of hepatic encephalopathy [195-197]. Emergent liver transplantation should be considered and prepared. Steroid or plasma exchange has been suggested in cases of severe acute exacerbation and ACLF, but data are currently limited to a small number of cases [198,199].
Some HBeAg-negative CHB patients show normal or mildly elevated ALT levels despite elevated HBV DNA levels (>2,000 IU/mL). Some patients move to the immune-inactive phase spontaneously —especially patients with low qHBsAg levels and low serum HBV DNA levels [200]. HBeAg-negative patients are those who have experienced the prior immune-active phase, and there is possibility that various degrees of fibrosis remain in these patients. For those with advanced fibrosis, antiviral treatment can be considered for those with elevated HBV DNA levels regardless of ALT levels [67,97]. Hence, HBeAg-negative CHB patients showing elevated HBV DNA levels (>2,000 IU/mL) but normal or mildly elevated ALT levels require careful evaluation of their degree of fibrosis to decide if they should undergo antiviral treatment or monitoring.
[Recommendations]
1. Antiviral therapy is recommended in HBeAg-positive CHB patients with HBV DNA ≥20,000 IU/mL, or HBeAg-negative CHB patients with HBV DNA ≥2,000 IU/mL if serum ALT level is ≥2 times the ULN. (A1)
In cases where ALT is 1–2 times the ULN, close ALT monitoring or liver biopsy can be considered. Antiviral therapy is recommended if liver biopsy reveals moderate to severe necroinflammation or significant fibrosis (≥F2). (A1)
Non-invasive fibrosis tests can be used to guide management decisions in cases where a liver biopsy is not feasible. (B1)
2. In patients with HBeAg-positive or HBeAg-negative CHB, prompt antiviral therapy should be initiated in the case of acute exacerbation, with elevation of ALT ≥5–10 times the ULN, signs of liver failure such as jaundice, PT prolongation, ascites, or hepatic encephalopathy. (A1)
3. In HBeAg-negative CHB patients with HBV DNA ≥2,000 IU/mL and normal ALT levels, follow-up can be considered. Otherwise, liver biopsy or non-invasive fibrosis tests can be considered for assessment of the degree of necroinflammation and/or fibrosis in order to determine whether treatment is needed. (B2)
CHB, immune-inactive phase
The immune-inactive phase is characterized by HBeAg-negative, anti-HBe-positive, persistently normal ALT levels, and undetectable or low (<2,000 IU/mL) serum HBV DNA levels. In this phase, long-term outcome without antiviral treatment is good for those without advanced fibrosis [45]. In contrast, risk of HCC is not low for patients with advanced fibrosis [201]. The immune-inactive phase is a dynamic phase that can reactivate to an immune-active phase [15]. Hence, patients in the immune-inactive phase require careful assessment of the degree of fibrosis and close monitoring of serum ALT and HBV DNA levels to verify whether they remain in the immune-inactive phase.
HBsAg loss or seroclearance is observed in 1–2% of patients per year in the immune-inactive phase [31,34]. HBsAg seroclearance is considered a surrogate endpoint for a functional cure of CHB. Hence, several studies investigated whether antiviral therapy in the immune-inactive phase can further induce HBsAg seroclearance [202].
Patients who remain in the immune-inactive phase are those with a low risk for HCC or liver-related complications during follow-up without antiviral treatment. The clinical benefit of inducing HBsAg loss by antiviral treatment in the immune-inactive phase, in terms of achieving treatment goals for CHB (improving overall survival or preventing the development of HCC), has not yet been demonstrated and requires further investigation.
Compensated cirrhosis
Antiviral treatment for compensated cirrhosis patients can decrease the risk of HCC and liver-related complications [155], and can improve liver fibrosis [149,203]. Serum ALT level may not be elevated in patients with cirrhosis, and the risk of developing a complication is high even for those with normal ALT levels [204]. Hence, cirrhotic patients with active HBV replication require antiviral treatment regardless of ALT levels. For cirrhotic patients, the risk of HCC decreases but remains even after achieving a virological response by antiviral therapy [205], requiring HCC surveillance.
For compensated cirrhosis patients, those with elevated HBV DNA levels (≥2,000 IU/mL) are indicated for antiviral therapy. For patients with detectable but low-level viremia (<2,000 IU/mL), recent EASL and AASLD guidelines recommend antiviral therapy [67,97]. An observational cohort study from Korea reported that 33% of compensated cirrhosis patients with low-level viremia experienced HBV DNA elevation ≥2,000 IU/mL during follow-up, and this was associated with an increased risk for developing HCC [206]. Furthermore, HCC risk was higher for patients who remained at low-level viremia compared to those with undetectable HBV DNA levels, and antiviral treatment was inversely associated with HCC risk in this group [206]. For compensated cirrhosis patients with low-level viremia, prompt antiviral treatment has the advantage of preventing HBV DNA elevation during follow-up, and may decrease the risk of developing complications in another observational study from Korea [207]. These data support prompt antiviral therapy for compensated cirrhosis with low-level viremia. However, until now, there have not been any randomized controlled trials that can assess the benefit and risks of prompt antiviral therapy for compensated cirrhosis patients showing low-level viremia.
[Recommendations]
1. In patients with compensated cirrhosis, antiviral therapy should be initiated regardless of ALT level if serum HBV DNA level is ≥2,000 IU/mL. (A1)
2. Antiviral therapy can be considered in compensated cirrhosis patients with detectable but low-level viremia (<2,000 IU/mL), regardless of ALT level. (B1)
Decompensated cirrhosis
Decompensated cirrhosis includes cases with ascites, variceal bleeding, hepatic encephalopathy, or jaundice [208]. Patients with decompensated cirrhosis might be managed in an institution that can respond appropriately to complications, and are candidates for liver transplantation. Antiviral therapy modifies the natural history of decompensated cirrhosis, improves liver function, decreases the need for liver transplantation, and improves survival [151,209]. However, even if antiviral therapy is administered, it takes time to acquire a virological response and recover clinically. Some patients with severely impaired liver function may not recover despite antiviral therapy, where liver transplantation should be considered for such cases [210]. Patients with decompensated cirrhosis are prone to liver failure when HBV reactivation occurs, which requires prompt antiviral therapy when serum HBV DNA is detectable, regardless of its serum levels. Administration of interferon is contraindicated because it may cause serious side effects including liver failure even with small doses [211].
MONITORING OF PATIENT WHO ARE NOT INDICATED FOR TREATMENT
Patients with CHB who are not on antiviral therapy need to be monitored on a regular basis to see if they become indicated for treatment. Patients in the immune-active phase are indicated for antiviral treatment, while those in the immune-tolerant phase and immune-inactive phase are not indicated for antiviral treatment. Serum HBeAg, anti-HBe, AST/ALT, HBV DNA levels, qHBsAg levels, and/or a liver biopsy can be considered to verify whether patients are indicated for antiviral treatment. qHBsAg tests are helpful in differentiating those in the immune-active phase from those in the immune-tolerant or immune-inactive phase [114,212-214]. Antiviral treatment is considered independent of the natural course of chronic HBV infection in patients with compensated or decompensated cirrhosis. Therefore, the severity of liver disease should be assessed by clinical findings, laboratory results, imaging studies, non-invasive liver fibrosis markers, and/or by performing a liver biopsy.
Chronic HBV infection is a dynamic process that requires regular monitoring. Serum ALT, HBV DNA, and HBeAg/anti-HBe should be monitored on a regular basis, and qHBsAg, non-invasive fibrosis tests, and/or a liver biopsy can be performed additionally during regular monitoring. For those who are not indicated for treatment, ALT and HBV DNA should be monitored at 3–6 months intervals, and HBeAg/anti-HBe monitoring should be performed at 6–12 months intervals. In real-life situations, sometimes it is difficult to categorize patients into those who are indicated for treatment or not (grey area). In such cases, more frequent monitoring of serum ALT and HBV DNA (every 1–3 months) and HBeAg/anti-HBe monitoring (every 2–6 months) can be performed to see if treatment criteria have developed. Despite close monitoring, some patients may remain in the grey area, and for them, non-invasive assessment of liver fibrosis or a liver biopsy should be considered to see whether patients require antiviral treatment and guide further management plans (Fig. 2).
[Recommendations]
1. In CHB patients not indicated for treatment, monitoring serum ALT and HBV DNA levels every 3–6 months and HBeAg/antiHBe every 6–12 months is recommended to assess if treatment criteria have developed. (B1)
2. If it is uncertain whether treatment is indicated, monitoring serum ALT and HBV DNA levels every 1–3 months and HBeAg/anti-HBe every 2–6 months are recommended. Otherwise, treatment decisions can be made by non-invasive fibrosis tests or a liver biopsy (B1).
TREATMENT STRATEGY
Currently approved antiviral treatments include peginterferon alfa and oral NAs. NAs can be classified into drugs with high genetic barriers and drugs with low genetic barriers (Table 4).215 When starting antiviral therapy for HBV, peginterferon monotherapy, oral NA monotherapy, or combination therapy with peginterferon plus NA can be considered [216-219]. Combination treatment with peginterferon plus NA aims to increase the serological response (e.g., HBsAg loss), which cannot be easily achieved by NA alone [216,217]. However, starting antiviral treatment with peginterferon plus NA offered no significant advantage over peginterferon or NA monotherapy [220,221]. Hence, in Korea where genotype C HBV infection is prevalent, combination treatment with peginterferon plus NA cannot be recommended as a better initial regimen than peginterferon alone or NA alone treatment.
Peginterferon treatment is recommended for a finite duration and has the advantage of providing immune-mediated control of the HBV and the possibility of achieving a sustained off-treatment response [219]. However, the major limitation of peginterferon is that it is a parenteral therapy with various side effects and limited efficacy. Peginterferon is also contraindicated in patients with decreased liver function (e.g., decompensated cirrhosis) [219]. Peginterferon treatment can be considered for compensated cirrhosis patients, but risks (possibility of treatment-related side effects and deterioration of liver function) and benefits (immune-mediated control, and sustained off-treatment response) should be carefully considered on an individual basis among highly selected patients. Once treatment with peginterferon has been started, early treatment discontinuation can be considered by monitoring side effects and the virological response during peginterferon treatment.
In contrast, NA treatment has no fixed treatment duration and requires indefinite treatment for most of the cases [156]. However, NA treatment has the advantage of being safe in most cases including patients with decompensated cirrhosis. There is a risk of drug resistance with NA treatment, and when drug-resistant HBV mutants develop, it can lead to treatment failure and progression of liver disease [222]. Newer agents with a high genetic barrier for antiviral resistance have significantly reduced the risk of drug resistance and can effectively suppress HBV replication with monotherapy alone. Hence, when starting antiviral treatment with NAs, monotherapy with a high genetic barrier to resistance is recommended. When choosing a specific NA, one should consider the efficacy and safety of the drug. Although the class effects of NAs remain unclear, each NA has a unique side effect profiles [223]. Hence, when the efficacy of one NA is expected to be similar to another NA, one should consider patient co-morbidities and the future risk of drug-related side effects when selecting an NA (Refer to “Management in Special Conditions” chapter).
[Recommendations]
1. For the treatment of patients with CHB, monotherapy using NAs with high genetic barriers to resistance or peginterferon alfa is recommended. (A1)
2. For the treatment of patients with compensated cirrhosis, monotherapy using NAs with high genetic barriers to resistance is recommended. (A1)
If underlying liver function is well preserved, treatment with peginterferon alfa may be considered with careful monitoring for deterioration of liver function and adverse drug reactions. (B2)
3. For the treatment of patients with decompensated cirrhosis, monotherapy using NAs with high genetic barriers to resistance is recommended. (A1)
Peginterferon alfa is contraindicated due to the risk of liver failure. (A1)
THERAPEUTIC AGENTS
In 2017, tenofovir alafenamide fumarate (tenofovir AF) and besifovir dipivoxil maleate (besifovir) were newly approved for treatment of CHB in adults. Currently, there are eight treatment options for CHB patients in Korea (Table 4).
Among the newly approved drugs, tenofovir AF is a nucleotide analogue with the same mechanism as the existing tenofovir disoproxil fumarate (tenofovir DF) and is maintained at a stable concentration in plasma, effectively metabolized in hepatocytes, and shows similar antiviral activity to tenofovir DF even at a smaller dose. As the amount of systemic exposure is small, tenofovir AF induces less renal and bone toxicity than tenofovir DF [224-227].
Besifovir is an acyclic nucleotide phosphonate that was developed in Korea as an oral antiviral agent and is similar to adefovir and tenofovir DF in structure [228,229]. Although clinical data are limited, besifovir has shown little effect on renal and bone toxicity and has similar effects to tenofovir DF in the Phase 3 trial [230]. Table 4 summarizes newly added drugs and existing treatments including peginterferon alfa 2a. NAs are classified into those associated with high genetic barrier to resistance (entecavir, tenofovir DF, tenofovir AF, besifovir) and those with low genetic barrier to resistance (lamivudine, telbivudine, clevudine, adefovir) (Table 4). In addition, although the efficacy of antiviral agents was not analyzed in head-to-head comparisons, the antiviral efficacy of individual drugs is described in Table 5.
NAs with high genetic barrier
Entecavir, tenofovir DF, tenofovir AF, and besifovir are recommended as first-line treatment for HBeAg-positive and -negative CHB patients. In particular, many clinical data of entecavir and tenofovir DF have been verified to show their long-term safety and efficacy [231-233]. Recently, clinical studies with up to 2 years of follow-up have suggested that tenofovir AF and besifovir exhibit better safety profiles than tenofovir DF, with similar antiviral efficacy [224-227,230]. Further clinical investigation focusing on long-term treatment outcomes should be performed to verify the antiviral efficacy and safety of these new antiviral agents.
NAs with low genetic barrier
Lamivudine, telbivudine, clevudine, and adefovir are not recommended as first-line treatment for patients with HBeAg-positive or -negative CHB because of viral resistance. However, these drugs have been used in clinical practice before introduction of antiviral agents with high genetic barriers, and they are still being prescribed in patients showing optimal virological responses.
Interferons
Interferon is a cytokine produced and secreted by immune cells in viral infection and has an antiviral effect and immunity-controlling activity. Although the precise mechanism is unclear, interferon alfa plays a role in destruction of cccDNA and viral mRNA, inhibition of the replication of viral DNA, and effective control of the immune response to virus-infected hepatocytes [234].
Peginterferon is a combination of interferon and polyethylene glycol molecules that has a long half-life, is easier to administer once per week, and has a stronger therapeutic effect compared to conventional interferon. The greatest advantage of peginterferon is the finite treatment period. The rate of HBsAg seroclearance was shown to be 2–7% at the first year after the end of treatment and increased to 12% at the fifth year [216,217,220,235-238].
DEFINITION AND PREDICTORS OF ANTIVIRAL TREATMENT RESPONSE
Definition of response
NAs
The virological response is defined as undetectable HBV DNA by a sensitive PCR assay (Table 6). A maintained virological response is defined by achieving a virological response and maintaining undetectable HBV DNA levels as assessed using a sensitive PCR assay. A partial virological response is defined as a decrease but detectable HBV DNA level after at least 24 weeks of therapy when using low genetic barrier drugs (e.g., lamivudine, telbivudine), and at least 48 weeks of therapy when using high genetic barrier drugs (e.g., entecavir or tenofovir) in compliant patients. A serological response is defined for HBeAg loss and HBeAg seroconversion for an HBeAg serological response in HBeAg-positive patients, and HBsAg loss or seroconversion for an HBsAg serological response. A viral breakthrough is defined as an increase in serum HBV DNA level of more than 1 log10 IU/mL compared with the lowest HBV DNA level on-therapy, or redetection of serum HBV DNA at levels of 10-fold the lower detection limit after achieving a virological response. A virological breakthrough usually precedes a biochemical breakthrough. A biochemical response is defined as a normalization of ALT levels, and a biochemical breakthrough is defined by an increase in ALT levels for patients who have achieved a biochemical response. Genotypic resistance is defined when HBV DNA mutations known to confer antiviral resistance during antiviral therapy have been detected. Phenotypic resistance is defined as decreased susceptibility (in vitro testing) to inhibition by antiviral drugs associated with genotypic resistance. Cross-resistance is defined as an HBV mutation selected by one antiviral agent that also confers resistance to other antiviral agents. HBV resistance to NAs is characterized by the presence of HBV variants with amino-acid substitutions that confer reduced susceptibility to the administered NA. Such resistance may result in primary treatment failure or virological breakthrough during therapy.
Peginterferon alfa
A primary non-response to peginterferon alfa is defined as a decrease of less than 1 log10 IU/mL in serum HBV DNA from baseline to after 3 months of therapy. A virological response is defined as an HBV DNA level of less than 2,000 IU/mL after 6 months or at the end of therapy. A sustained off-therapy virological response is defined as an HBV DNA level of less than 2,000 IU/mL at least 6 months after the end of therapy. A serological response is defined by HBeAg loss or HBeAg seroconversion for an HBeAg serological response in patients with HBeAg-positive CHB, and HBsAg loss or HBsAg seroconversion for HBsAg serological response.
Predictors of response
NAs
Pre-treatment serum ALT levels, HBV DNA levels, HBeAg levels, and qHBsAg levels are factors associated with the virological response [99,239]. Serum HBV DNA levels, ALT levels, severe necroinflammation as observed on a liver biopsy, and a maintained virological response are factors associated with the HBeAg serological response in HBeAg-positive CHB [240-243]. When using low genetic barrier drugs such as lamivudine, adefovir, or telbivudine, undetectable HBV DNA at 6–12 months of treatment was also associated with a virological response [244-247]. Caucasian patients, those infected with HBV genotype A or D, males (as opposed to females), and the virological response were factors associated with HBsAg serological response during entecavir therapy [248]. Caucasian race, less than 4 years of infection, HBV genotype A or D, and a reduction in HBsAg levels >1 log10 U/mL by week 24 were factors associated with HBsAg serological response during tenofovir therapy [249]. In Asian patients with CHB, achieving a viral suppression took longer for patients who had a high baseline viral load (≥9 log10 copies/mL) [250]. HBV genotype was not associated with the virological response to NA therapy.
Peginterferon alfa
The HBV genotype is associated with the treatment response to peginterferon alfa therapy. Those with HBV genotype A or B showed a more favorable HBeAg response, HBsAg response, and virological response than those with HBV genotype C or D [108,220,251,252].
In Korea, almost all patients are infected with HBV genotype C, which should be considered when treating patients with peginterferon. High serum ALT levels, low HBV DNA levels, severe necroinflammation, and HBV genotype are factors associated with HBeAg serological response in HBeAg-positive CHB [216,253]. High serum ALT levels, low HBV DNA levels, young age, and female sex are factors associated with the virological response in HBeAgnegative CHB [217,253]. On-treatment factors, such as HBV DNA levels, quantitative HBeAg levels, and qHBsAg levels, are also associated with virological response during peginterferon therapy [116,254-256].
MONITORING DURING ANTIVIRAL TREATMENT
NAs
Persistent HBV replication during antiviral treatment is a major risk for hepatitis progression and viral mutation [257]. Serum HBV DNA should be measured every 1 to 6 months during antiviral therapy to facilitate treatment adjustments based on serum HBV DNA levels.
Although serum HBV DNA is less than 2,000 IU/mL during therapy, the incidence of HCC is higher in patients with detectable HBV DNA persistently or intermittently than in patients with undetectable HBV DNA persistently [205]. Therefore, serum HBV DNA should be measured every 3 to 6 months during antiviral therapy even after virological response. Serum HBV DNA reduction to an undetectable levels by real-time PCR (<10–15 IU/mL) should ideally be achieved [97,258].
Although qHBsAg levels is less likely to decrease with NAs compared to peginterferon alfa [259-261], the degree of reduction in HBV DNA is correlated with the degree of reduction in HBsAg levels [259]. Low pretreatment HBsAg levels and greater HBsAg decline after 24 weeks of treatment were reported to be positive predictors of a long term virological response [262-264]. In patients with CHB having received ten years of NA therapy, low baseline HBsAg levels (<1,000 IU/mL) and a greater rate of HBsAg reduction on-therapy (>0.166 log10 IU/mL/year) were predictive of HBsAg loss [265]. Low HBsAg levels (10–200 IU/mL) on cessation of therapy have been reported to be a good predictor of persistent virological response and HBsAg loss after antiviral cessation [118,266-269]. Therefore, monitoring of qHBsAg could be helpful in practice.
Drug compliance and emergence of antiviral-resistance mutations should be monitored in patients who develop virological breakthrough while receiving NAs, and an appropriate rescue therapy should be initiated if necessary (Fig. 3) [35,79,270-272].
Most NAs are excreted through the kidney, and hence dose adjustment is required in patients with renal insufficiency (refer to section on renal impairment). Regular monitoring of renal function and bone mineral density should be performed in patients receiving adefovir or tenofovir DF [273,274]. A large prospective study of entecavir-related carcinogenicity found comparable cancer incidence between entecavir and other NAs [232]. There have been few reports on telbivudine-related myositis; however, monitoring of serum creatine kinase (CK) levels is recommended due to the possibility of CK elevation [178,275]. Levels Serum CK levels and related symptoms should also be monitored in patients receiving clevudine (Fig. 3) [276,277].
Peginterferon alfa
The serum CBC and ALT levels of patients receiving peginterferon alfa should be tested monthly. Serum HBV DNA should be measured after 1–3 months of treatment to facilitate treatment adjustments based on serum HBV DNA levels. There is a high probability of HBsAg loss if serum HBV DNA becomes undetectable during treatment. Patients with who are HBeAg-positive should be tested for HBeAg and anti-HBe at 6 and 12 months during treatment and 6 months post treatment. Patients should be monitored for 6–12 months after treatment cessation. For response prediction, a qHBsAg levels can be used before treatment and after 12 and 24 weeks of treatment [116,255,256,278,279]. All patients treated with peginterferon alfa should be assessed for known adverse effects of interferon at every visit.
[Recommendations]
1. During treatment with NAs, liver function tests and serum HBV DNA measurement at 1–6 month intervals and HBeAg/antiHBe at 3–6 month intervals are recommended. (B1)
HBsAg quantification may be considered, which may help predict antiviral response and determine treatment cessation. (B2)
2. During peginterferon alfa therapy, CBC and liver function tests every month, serum HBV DNA at intervals of 1–3 months, and HBeAg/anti-HBe at 6 months and one year during treatment and 6 months after treatment are recommended. (B1)
HBsAg quantification is recommended pre-treatment, after 12 and 24 weeks of treatment, and at the end of treatment. (B1)
3. Even after virological response, serum HBV DNA measurement is recommended at intervals of 3–6 months. (B1)
4. Monitoring the side effects of each drug during antiviral therapy is necessary. (A1)
CESSATION OF TREATMENT AND MONITORING ANTIVIRAL TREATMENT
Clinical biomarkers for treatment endpoint
In patients with CHB, it is realistically difficult or impossible to determine the appropriate timing of treatment cessation after achieving the ultimate goal of therapy, which is improvement in survival. Therefore, alternative biomarkers that reflect achievement of treatment goals that can easily be measured are needed when evaluating treatment cessation. ALT normalization, undetectable HBV DNA, HBeAg loss or seroconversion and HBsAg loss or seroconversion have been used as treatment endpoints. Cessation of therapy is not recommended in patients with liver cirrhosis because there is a risk of serious liver failure due to relapse and flare after cessation of therapy [67,97].
The standard treatment duration of peginterferon alfa is 48 weeks [217,238]. However, there have been some reports that extended dosing could be more effective in HBeAg-negative CHB [280,281].
ALT normalization
Normalization of ALT in CHB treatment reflects a decrease in hepatic inflammatory response, mostly associated with undetectable HBV DNA, and reduces clinical deterioration [174]. Normalization of ALT during treatment reflects improvement in cirrhosis and therefore could be considered reflective of treatment goals [149].
However, 14–40% of patients with persistently normal ALT could have more than significant fibrosis (≥F2) and there are a variety of factors affecting ALT, such as non-alcoholic or alcoholic fatty liver [162,172,282]. As such, ALT normalization alone is insufficient when determining the endpoint of treatment.
Undetectable HBV DNA
HBV DNA level is the strongest predictor of disease progression and long-term outcomes in the natural course of CHB [45,47]. HBV DNA levels are associated with histological activity in patients with CHB, and rate of progression to decompensation is low and that of survival is high in patients with low HBV DNA [283,284].
Antiviral therapy can reduce HBV DNA, and histological improvement can be achieved in proportion to HBV DNA reduction [285]. When HBV DNA is not detectable for long-term and virological response is well maintained [286,287], the HBsAg loss rate increases even after cessation of therapy in HBeAg-negative CHB patients [286,288]. Therefore, cessation of therapy could be considered in HBeAg-negative CHB patients with long-term undetectable HBV DNA [289]. However, in practice, most patients relapsed after cessation of therapy [290-292]. Hence, undetectable HBV DNA cannot be the sole factor determining treatment cessation.
HBeAg loss and/or seroconversion
HBeAg seroconversion in HBeAg-positive CHB is accompanied by HBV DNA reduction, ALT normalization, and improvement in histological findings after antiviral therapy [285,293]. After HBeAg seroconversion, HBsAg loss also increases to 1.15% per year [31]. The incidence of liver cirrhosis and HCC is reduced and survival is improved in both patients with spontaneous or treatment-induced HBeAg seroconversion compared to patients who are persistently HBeAg positive [7,15,283,294,295]. Therefore, HBeAg loss/seroconversion in HBeAg-positive CHB could be considered biomarkers reflecting achievement of treatment goal.
However, HBeAg-negative hepatitis has been reported in 24% of patients even after HBeAg seroconversion [15]. Furthermore, the incidence of HBeAg reversion and an increase in HBV DNA was noted after treatment cessation in patients who achieved HBeAg loss/seroconversion on antiviral therapy [286,287,296,297]. Therefore, the evidence for recommending treatment cessation depending on HBeAg loss/seroconversion alone is lacking. Nevertheless, the risk of recurrence is reduced if treatment is discontinued after being maintained for a sufficient period of time (e.g., more than 12 months) after HBeAg loss/seroconversion [298,299].
HBsAg loss
HBsAg levels quantified by qHBsAg assay reflect the natural course of disease in patients with CHB [112], and are also proportional to the levels of cccDNA in the liver [300]. HBsAg levels may decrease after HBeAg loss during antiviral therapy [259]. The incidence of HCC is significantly reduced when HBsAg loss occurs before age 45–50 [23,301]. Some patients with HBsAg loss/conversion during antiviral therapy showed HBsAg reversion or low but detectable HBV DNA, but most patients maintain HBsAg loss and undetectable HBV DNA levels, and their incidence of HCC is significantly lower compared to patients without HBsAg loss [154,302]. Therefore, HBsAg loss is the ideal endpoint of antiviral therapy in CHB, reflecting the treatment goal, at which point NAs can be discontinued. Recently, it has been reported that HBsAg reversion can be better avoided if antiviral therapy is discontinued after maintaining treatment for 6–12 months or longer despite HBsAg loss [302].
However, HBsAg loss is very rare and long-term treatment (50 years or longer) is required based on the decreasing dynamics of HBsAg levels during treatment with NAs [303,304]. Despite HBsAg loss, there is always a risk of developing HCC and surveillance is still necessary [301,305,306]. It remains unclear whether HBsAg loss will further improve the long-term clinical prognosis beyond that expected by undetectable HBV DNA.
Monitoring after antiviral treatment
The response to antiviral treatment persists in some patients, while others relapse. Therefore, regular monitoring of liver function tests, HBeAg, anti-HBe, and HBV DNA is needed to evaluate the durability of the treatment response, relapse, and deterioration in liver function. qHBsAg levels may be helpful in monitoring HBsAg reduction or loss in patients without HBsAg loss after cessation of therapy. Even in patients in whom HBsAg loss has been achieved, there is the potential risk for reversion of HBsAg or development of HCC [154,301,302]. Therefore, serum HBsAg and/or antiHBs should be monitored and HCC surveillance should be performed continuously.
[Recommendations]
1. Cessation of NAs is recommended after serum HBsAg loss in CHB patients. (A1)
2. In HBeAg-positive CHB patients, cessation of NA therapy could be considered at least 12 months after HBV DNA is undetectable and serum HBeAg loss or seroconversion has been achieved. (B2)
3. Long-term treatment should be considered in patients with liver cirrhosis. Indefinite NA therapy is recommended in patients with decompensated liver cirrhosis. (B1)
4. Peginterferon alfa is administered for 48 weeks. (A1)
5. Liver function testing and serum HBV DNA measurement at 1–6-month intervals and HBeAg/anti-HBe testing at 3–6-month intervals are recommended during the first year after cessation of antiviral treatment. Liver function testing and serum HBV DNA measurement at 3–6-month intervals and HBeAg/anti-HBe testing at 6–12-month intervals are recommended if treatment response is maintained beyond one year after antiviral therapy. (B1)
6. If virological response is maintained after cessation of antiviral treatment, follow-up HBsAg/anti-HBs testing should be performed to confirm HBsAg loss, maintenance, or reversion. (B1)
ANTIVIRAL RESISTANCE
The development of antiviral resistance decreased significantly after the use of drugs with high genetic barriers such as entecavir and tenofovir (including tenofovir DF and tenofovir AF) as first-line treatments. Nonetheless, antiviral resistance is an important factor that determines success or failure of CHB treatment. The emergence of antiviral resistance results in resumption of active viral replication that had been suppressed by antiviral therapy and can impair biochemical or histological improvement. Therefore, prevention, early diagnosis, and management of antiviral resistance may significantly affect the long-term prognosis of CHB patients undergoing antiviral therapy [307-309].
Mechanism of antiviral resistance and definitions
Mutations in HBV can occur in all four open reading frames (ORF) of preS/S, polymerase, precore/core, and X. Among the mutations in the polymerase ORF, which is the target of several NAs, those that can replicate under the influence of the antiviral agent are selected, and the ratio is increased. Although the first-occurring antiviral-resistant mutant has decreased replication capacity, a compensatory mutation develops over time that restores replication capacity to the wild-type level [310]. Selection for a particular mutation affects both resistance to the drug being administered and the replication capacity.
A genetic barrier is defined as the number of genetic mutations needed to develop antiviral resistance, with a higher genetic barrier indicating a lower risk of resistance [311]. The antiviral potency of drugs also influences the development of resistance. Therefore, as a first-line treatment, it is important to use drugs with a high barrier to HBV resistance such as entecavir, tenofovir, and besifovir, which have a high inhibitory effect on virus proliferation, or, alternately, peginterferon alfa. If other drugs have been used, careful monitoring for resistance development is required.
Mutations conferring resistance to antiviral agents
Antiviral agents used in treatment of HBV infection are classified into two groups: nucleoside analogues (L-nucleoside analogues [lamivudine, telbivudine, and clevudine] and cyclopentenes [entecavir]) and nucleotide analogues (acyclic phosphonates [adefovir, tenofovir, besifovir]) [312]. Cross-resistance between nucleosides and nucleotide analogues is rarely observed. Tables 7 and 8 summarize the types and frequencies of known drug resistance mutations.
Nucleoside analogues
L-nucleoside analogues (lamivudine, telbivudine, and clevudine): All L-nucleosides have a similar molecular structure and target site of action, resulting in similar patterns of antiviral resistance mutations. Mutations at rtM204 are the primary resistance mutations to L-nucleosides [309,313-315]. The rtM204V and rtM204I mutations involve substitution of methionine with valine and isoleucine, respectively, at codon 204 of the reverse transcriptase gene [316]. Originally, these were termed YMDD mutations [316]. The specific primary mutations conferring resistance are rtM204V/I substitutions for lamivudine and only the rtM204I substitution for telbivudine and clevudine [178,317-319]. An rtM204V mutant may commonly accompany rtL180M but not rtM204I [320]. These mutants are sensitive to nucleotide analogues, but they exhibit cross-resistance to entecavir and an eight-fold decrease in sensitivity. The rtA181T mutation has been detected in 5% of lamivudine-resistant patients, in whom susceptibility to telbivudine and clevudine is also reduced. This mutation confers concomitant resistance to adefovir, but these mutants remain susceptible to entecavir [321].
Cyclopentene (entecavir): Resistance to entecavir occurs through a two-hit mechanism. rtL180M and rtM204V first develop as background mutations, and then additional mutations such as rtT184L/F/A/M/S/I/C/G, rtS202G/I/C, or rtM250V/I/L develop as primary resistance mutations to entecavir, resulting in a marked decrease in drug susceptibility [311,322]. rtI169T is a compensatory mutation that increases the fold resistance of rtT184, rtS202, and rtM250 mutants. Since multiple genetic mutations are needed to develop high-level resistance to entecavir (high genetic barrier), the resistance rate in treatment-naïve CHB patients is very low. However, a resistance rate as high as 51% has been reported after five years of treatment in lamivudine-refractory subjects [323]. In addition, exposure to lamivudine increases the risk of resistance to entecavir even if no previous resistance has occurred [324]. Thus, it is important to use drugs with a high barrier to HBV resistance as first-line treatment.
Nucleotide analogues
Adefovir: rtN236T and rtA181V/T are the primary resistance mutations to adefovir [325,326]. The levels of resistance of rtN236T and rtA181T to adefovir are 7- to 10-fold and 2.5- to 5-fold, respectively, compared to the wild-type virus [312,321]. rtA181T can be detected in subjects receiving lamivudine monotherapy or combination therapy comprising adefovir plus lamivudine [327,328].
Tenofovir: rtA194T can decrease susceptibility to tenofovir by 6.9- to 10-fold in the presence of rtL180M+rtM204V mutations [329-331]. It has been reported that rtS78T/sC69* inhibits tenofovir sensitivity 1.6-fold [332], but its clinical significance needs to be confirmed. Recently, a novel mutation was found in sera of patients with viral breakthrough in the treatment of tenofovir DF in Korea [333]. In a laboratory phenotypic resistance study, rtS106C+ rtH126Y+rtD134E+rtL269I conferred a 15.3-fold increase in resistance to tenofovir.
MANAGEMENT OF ANTIVIRAL RESISTANCE
Prior antiviral resistance predisposes individuals to subsequent viral mutations and limits the choice of rescue therapies due to cross-resistance [312,336]. In addition, even if antiviral agents without cross-resistance are selected, resistance to rescue therapy is more frequent than in treatment-naïve subjects [336-338]. Careful selection of a first-line antiviral agent is essential to minimize resistance and cross-resistance to other agents.
Antiviral resistance testing is required when a virological or biochemical breakthrough is detected in subjects with good compliance. In cases of resistance, an appropriate rescue therapy should be initiated with the most effective antiviral agent without crossresistance to minimize the risk of inducing multiple drug-resistant strains [339]. Table 9 shows recommendations for treatment adaptation.
Management of nucleoside analogue resistance
Patients with confirmed resistance to nucleoside analogues such as lamivudine, telbivudine, clevudine, and entecavir can be changed to treatment with tenofovir alone. A prospective study showed that tenofovir DF monotherapy was highly efficacious in patients with lamivudine-resistant HBV and comparable to the combination of tenofovir DF and emtricitabine, without emergence of additional resistance mutations to tenofovir DF throughout 96 weeks of treatment [340]. Although data on rescue therapy with telbivudine and clevudine are lacking, their resistance mutations are very similar, and we recommend that treatment be based on lamivudine resistance. A recent multicenter randomized trial with patients who had lamivudine/entecavir-resistant HBV, found that the proportion of patients with HBV DNA <15 IU/mL was not significantly different between the tenofovir DF and tenofovir DF/ entecavir groups (71% vs. 73%) [341]. A retrospective study that compared tenofovir DF with tenofovir DF/entecavir among patients who had lamivudine/entecavir-resistant HBV found that the HBV undetectable rate up to 24 months (HBV DNA <20 IU/mL) did not differ significantly between groups (85.4% vs. 89.2%) [342]. However, tenofovir DF/entecavir combination therapy was superior to tenofovir DF monotherapy in patients with a high baseline viral load (HBV DNA >4 log IU/mL).
Management of nucleotide analogue resistance
Switching to tenofovir monotherapy or tenofovir/entecavir combination therapy is recommended in cases of adefovir resistance. In vitro studies showed that susceptibility of adefovir-resistant HBV with a single rtN236T or rtA181V/T mutation to tenofovir is similar to that of wild-type HBV, but susceptibility is lower when both mutations are present [321]. Clinically, most studies have found that tenofovir is effective in suppressing adefovir-resistant HBV. Tenofovir DF alone or tenofovir DF and emtricitabine are similarly effective in patients with CHB treated with adefovir (82% vs. 84%) [343]. However, this study reported that only 27.6% of patients had HBV with adefovir resistance mutations. A recent multicenter randomized trial with patients who had adefovir-resistant HBV found that the proportion of patients with HBV DNA <15 IU/mL was not significantly different between those treated with tenofovir DF and tenofovir DF/entecavir (62.0% vs. 63.5%) [344]. When these patients were followed for three years, there was no difference in incidence of undetectable HBV DNA level between the two groups. However, the decrease in serum HBV DNA level tended to be smaller in a subgroup of patients with HBV that had both adefovir resistance mutations, (rtA181T/V and rtN236T), though longer follow-up is needed to confirm this finding [345]. A Korean retrospective study reported that tenofovir DF had inferior efficacy in adefovir-experienced CHB patients [346]. Thus, CHB patients with a history of adefovir exposure should be monitored closely for response to tenofovir monotherapy and virological breakthrough.
We recommend adding entecavir to tenofovir in cases of tenofovir resistance. However, if the resistance is accompanied by that to entecavir, treatment with a nucleos(t)ide antiviral agent is difficult, indicating the need for a new therapeutic agent.
Management of multidrug resistance
Although there is no clear international definition, management of multidrug resistance (MDR) is defined as resistance to two or more classes of antiviral drugs [336]. This is due to the low efficacy of adefovir and entecavir used as previous rescue therapy for L-nucleoside analogue resistant-HBV and their sequential therapy alone. Most studies on MDR management have few patients with heterogeneous resistance mutations and a diverse combination of therapies. Although there is no established treatment, tenofovir/entecavir combination therapy, tenofovir monotherapy, and adefovir/entecavir combination therapy are the preferred treatment options [347]. The serum HBV DNA non-detection rate (<12 IU/mL) was reported to be 62.5% in a prospective multicenter study of 64 patients with MDR CHB after 48 weeks of treatment with tenofovir DF/entecavir combination therapy [348]. Tenofovir DF monotherapy had non-inferior antiviral efficacy compared with tenofovir DF-based combination therapy in MDR CHB patients in a multicenter cohort studies [47,349]. In addition, there was no significant difference in virological response at 48 weeks between tenofovir DF monotherapy and tenofovir DF/entecavir combination therapy (66.3% vs. 68.0%) in CHB patients with resistance mutations to ETV and/or adefovir [345]. In this regard, patients with MDR CHB may be treated with tenofovir monotherapy.
There has been a recent report of tenofovir resistance in Korea [350]. Also, a prospective study found that approximately onequarter of patients, particularly those with adefovir-resistant CHB, did not have a satisfactory virological response until three years of rescue therapy [345]. It is therefore necessary to identify factors predictive of treatment response and to verify long-term therapeutic effects.
[Recommendations]
1. If a virological breakthrough occurs during NA treatment, patient medication compliance should be assessed, and antiviral resistance testing should be performed. (A1)
2. Rescue therapy for antiviral resistance should be initiated as soon as possible once a virological breakthrough is detected and genotypic resistance is confirmed. (A1)
3. For CHB resistant to L-nucleoside analogues such as lamivudine, telbivudine, and clevudine, switch to tenofovir monotherapy. (A1)
4. For entecavir-resistant CHB, switch to tenofovir monotherapy, or add tenofovir. (A1)
5. For adefovir-resistant CHB, switch to tenofovir monotherapy or tenofovir and entecavir combination therapy. (A1)
6. For tenofovir-resistant CHB, add entecavir. (B1)
7. For multidrug-resistant CHB, switch to tenofovir and entecavir combination therapy or tenofovir monotherapy. (A1)
MANAGEMENT ACCORDING TO TREATMENT RESPONSE
Persistent viral replication during antiviral treatment for CHB is a risk factor for the progression of hepatic fibrosis and the development of antiviral-resistant mutations. Thus, treatment response should be evaluated by measuring serum HBV DNA levels with sensitive real-time PCR methods at 3–6-month intervals. Even for patients who achieved virological response, treatment response needs to be monitored at 3–6 month intervals until the patient is able to stop medication after achieving the treatment goal [109]. When patients under peginterferon alfa treatment show insufficient virological response, early cessation of treatment can be considered.
Management of partial virological response to NAs
Although there have been few studies on partial virological response, it is recommended to switch from one NA to other NA options with no cross-resistance and a high genetic barrier for treatment-adherent patients with partial virological response (Fig. 3). Upon switching to entecavir 1 mg per day in patients with a partial virological response to lamivudine, 67.6% of patients demonstrated an undetectable HBV DNA (<60 IU/mL) rate at week 96 [351]. However, as lamivudine-experienced patients treated with entecavir showed a relatively higher risk of developing entecavir-resistant mutation in lamivudine-experienced patients [324], caution is needed when switching to entecavir. In contrast, tenofovir was reported to provide good antiviral efficacy regardless of prior exposure or resistance to lamivudine [336]. In the case of partial virological response to either entecavir or tenofovir, which have a high genetic barrier, medication can be maintained if serum HBV DNA decreases continuously, since the risk of developing a resistant mutation is low and delayed virological response can be expected without changing the antiviral regimen. However, switching to another drug might be considered if the decrease in HBV DNA is not remarkable within 12 months (Fig. 3) [97]. Recently, a prospective randomized trial in Korea reported that upon switching to tenofovir DF, 55% of patients with partial virological response to 12 months of entecavir treatment showed undetectable serum HBV DNA (<20 IU/mL) at month 12, compared to 20% in an entecavir maintaining group [352]. A meta-analysis also reported that switching to tenofovir DF is effective for those patients [353]. Prior research on the optimal treatment strategy for partial virological response to tenofovir has been highly limited. In a Korean study, 90.2% of patients who showed partial virological response to tenofovir DF treatment at month 12 achieved virological response at year three when they continued tenofovir DF treatment [354].
Management after achieving virological response with NA treatment
Tenofovir DF monotherapy showed comparable antiviral efficacy to tenofovir DF/entecavir combination therapy for patients with entecavir- or adefovir-resistant mutations in prospective randomized trials [341,344,345,349,355]. Based on these studies, a switch to tenofovir monotherapy can be considered in patients achieving virological response to rescue combination therapy with tenofovir and entecavir. Since long-term treatment is currently inevitable for CHB, the potential benefit and risk, or cost of combination therapy should be weighed. A Korean retrospective study reported that virological response was sustained in all 76 patients during a median 2-year follow-up when the rescue treatment was switched from combination treatment with tenofovir DF plus entecavir to tenofovir DF monotherapy [356].
The ideal endpoint of antiviral treatment for CHB patients is a functional cure with HBsAg loss. Although HBsAg can be lost with NAs alone, the annual rate was as low as 0.8% [357]. Therefore, there have been a number of studies on additional interferon treatment and/or therapeutic vaccination on NAs to maximize treatment effect.
Several randomized controlled trials reported 4–9.8% HBsAg seroclearance rates when NA was changed to 48-week peginterferon alfa treatment with/without maintaining NA [358-362]. In addition, 96-week peginterferon alfa treatment increased the HBsAg seroclearance rate to 15.3%. However, another study showed no difference in HBsAg seroclearance rate between the adding peginterferon alfa group (n=92) and continuing NA group (n=93) (7.8% vs. 3.2%; P=0.15) in HBeAg-negative patients achieving virological response with NAs [363]. A recent Korean randomized controlled study reported a 16.2% HBsAg seroclearance rate with an additional 48-week peginterferon alfa-2a treatment period (180 µg every week) and sequential HBV vaccination in patients who achieved virological response with entecavir and qHBsAg was <3,000 IU/mL [364]. However, although additional treatment with interferon and/or therapeutic vaccination can be an option to increase the chance of HBsAg loss, the treatment benefit of combination or sequential therapy over monotherapy with NAs is unclear in Korea, where genotype C HBV is prevalent. Further studies comparing treatment benefit and cost or adverse event of those additional treatments are warranted prior to applying those additional treatment strategies in clinical practice.
Management of suboptimal response to peginterferon alfa
Serum qHBsAg titer is a good predictor of response to peginterferon alfa and is utilized as a stopping rule [67,97]. In HBeAg-positive CHB patients, a decline of qHBsAg levels below 1,500 IU/mL at 12 weeks in a reasonable predictor of HBeAg seroconversion. However, qHBsAg levels >20,000 IU/mL at 12 or 24 weeks are associated with a very low probability of subsequent HBeAg seroconversion and can be considered as peginterferon alfa stopping rules [116,256].
In HBeAg-negative CHB patients, a decline of HBV DNA by ≥2 log10 IU/mL at 12 weeks and a ≥10% decline in serum qHBsAg from baseline to week 12 had a higher probability of achieving a sustained response. However, the combination of a lack of decrease in qHBsAg levels and <2 log10 IU/mL decline in HBV DNA at 12 weeks predicts no treatment response and are considered peginterferon alfa stopping rules [254,255,365].
[Recommendations]
1. Compliance with medication should be carefully monitored in patients with a partial virological response to NA therapy. (A1)
2. In CHB patients with a partial virological response to NAs with low genetic barriers, switching to NAs with high genetic barriers and no cross-resistance is recommended. (A1)
3. In CHB patients with a partial virological response to NAs with high genetic barriers, treatment can be continued while monitoring virological responses at 3–6-month intervals. (B1)
However, in the case of partial virological response to entecavir, switching to tenofovir can be considered. (A2)
4. During peginterferon alfa treatment, qHBsAg levels >20,000 IU/mL after 24 weeks of therapy in HBeAg-positive CHB patients as well as a combination of stable qHBsAg levels and a reduction in serum HBV DNA levels to less than 2 log10 IU/mL after 12 weeks of therapy in HBeAg-negative CHB patients are associated with a very low probability of subsequent treatment response, and cessation of therapy should be considered. (B2)
MANAGEMENT IN SPECIAL CONDITIONS
Patients with HCC
The aims of antiviral treatment in patients with HBV-related HCC are: i) the suppression of HBV replication to prevent the progression of hepatic dysfunction, thereby enabling active treatment of HCC and ii) the reduction of HCC recurrence after potentially curative treatment [97].
Antiviral treatment after curative treatment of HCC
There have been several studies that reported antiviral treatment was associated with lower risk of tumor recurrence after curative treatment (i.e., surgical resection, radiofrequency ablation [RFA], and percutaneous ethanol injection) for HBV-related HCC. A Taiwanese large-scale retrospective study reported that patients who underwent NA treatment with entecavir, lamivudine, telbivudine, etc. showed a significantly lower risk of tumor recurrence or overall death after surgical resection for HCC, although the prevalence of cirrhosis was significantly higher [366]. Even in patients with low-level viremia (HBV DNA <2,000 IU/mL), antiviral treatment was associated with longer recurrence-free survival (P=0.016) and overall survival (P=0.004) [367]. A meta-analysis showed that the antiviral treatment group had significantly lower risk of tumor recurrence (odds ratio [OR], 0.59; 95% confidence interval [CI], 0.35–0.97; P=0.04), liver-related mortality (OR, 0.13; 95% CI, 0.02–0.69; P=0.02), and overall mortality (OR, 0.27; 95% CI, 0.14–0.50; P<0.001), than the no antiviral treatment group [368]. In a retrospective Korean study, antiviral treatment with high-potency NAs (i.e., entecavir and tenofovir) showed significantly longer recurrence-free survival than both antiviral treatment with lowpotency NAs (i.e., lamivudine, clevudine, and telbivudine) and no antiviral treatment [369]. In contrast, a randomized controlled trial reported that adjuvant interferon alfa-2b treatment was not associated with lower risk of post-resection tumor recurrence (P=0.828) [370].
Antiviral treatment during HCC treatment
An increase in serum HBV DNA or HBV reactivation accompanied by abnormalities on biochemical liver function testing has been observed in 14–32% of CHB patients who undergo surgical resection for HCC [371]. A prospective study reported that the HBV reactivation rate after surgical resection was 2.5% in patients that underwent antiviral prophylaxis with telbivudine and 31.8% in controls [372].
The post-RFA risk of HBV reactivation was reported to be 5.6–9.1%, whereas no reactivation was reported after percutaneous ethanol injection [373,374]. After transarterial chemoembolization (TACE), approximately 4–40% of patients with HBV-related HCC developed HBV reactivation [375-380]. Post-TACE risks of HBV reactivation, flare-up hepatitis, and liver failure due to HBV reactivation were 2.8%, 2.8%, and 0%, respectively, in the prophylactic lamivudine treatment group and 40.5%, 29.7%, and 8.1% in the control group. There was a significant difference between the two groups [378]. After hepatic artery infusion chemotherapy (HAIC), HBV reactivation was reported in 24–67% of patients, which was relatively higher than after TACE. This finding can potentially be explained by a larger total amount of cytotoxic chemotherapeutic agent due to shorter treatment interval than TACE [381,382].
In patients who underwent external beam radiation therapy (EBRT) for HCC, reactivation and ALT elevation were reported in 0% and 2.3%, respectively, of the lamivudine-prophylaxis group, and 21.8% and 12.5%, respectively, of the control group. The control group had significantly higher risk of HBV reactivation [383]. The combination treatment with TACE and EBRT had twice the risk of HBV reactivation compared to TACE treatment alone [384]. The incidence of HBV reactivation after cytotoxic chemotherapy was reported to be 30–60%, 30% of which resulted in death [380,381].
In CHB patients, prophylactic antivirals should be maintained for at least 6 months after cessation of cytotoxic chemotherapy and life-long administration is recommended. Interferon is not recommended as a prophylactic antiviral due to bone marrow suppression and transient hepatitis aggravation. There was no reactivation reported during sorafenib treatment in a retrospective study [385], while another study reported a high risk of HBV reactivation [386]. Thus, further observational studies are warranted. Immune checkpoint inhibitors, such as nivolumab and pembrolizumab, may enhance host immunity and consequently have a lower risk of HBV reactivation. However, immune checkpoints can result in severe acute aggravation of hepatitis since it can upregulate antiviral immunity against HBV. Therefore, suppression of HBV replication with antiviral treatment is necessary before use of immune checkpoint inhibitors [387].
In conclusion, HBV reactivation after various treatments for HBV-related HCC is frequently observed and prophylactic antiviral treatment can reduce the risk of HBV reactivation. Thus, prophylactic antiviral treatment is recommended for patients who undergo surgical treatment, locoregional treatment, radiation treatment, and systemic treatment for HBV-related HCC, regardless of detectable serum HBV DNA.
[Recommendations]
1. In patients with HBV-related HCC, antiviral therapy should be initiated if serum HBV DNA is detected. (A1)
2. In patients with HBV-related HCC who undergo anticancer treatment, prophylactic antiviral therapy with NAs should be considered regardless of detectable serum HBV DNA. (B1)
Patients with renal dysfunction or metabolic bone disease
Long-term administration of adefovir or tenofovir DF in the patients with CHB, may result in decreased renal function and bone mineral density. Side effects such as acute on chronic renal failure, hypophosphatemia, and Fanconi syndrome have been reported [274,388-390]. If patients already have risk factors for renal dysfunction and/or metabolic bone disease, or if worsening kidney function or bone disease is detected during treatment, a change in treatment regimens needs to be considered.
Patients with renal dysfunction or metabolic bone disease prior to starting the treatment
Patients with chronic kidney disease are known to have relatively higher rate of exposure to HBV infection [391]. In Korea, around 5% of HBsAg positive rate has been reported among the hemodialysis patients [392-396]. When starting the oral antiviral agents in the patients with chronic kidney disease, we need to adjust the dose according to the creatinine clearance (Table 10). If creatinine clearance is below 15 mL/min without renal replacement therapy, tenofovir AF is not recommended. Same goes for besifovir in case of creatinine clearance below 50 mL/min. Tenofovir DF is not recommended in the patients with both creatinine clearance below 10 mL/min and no renal replacement therapy.
Because nucleotide analogue treatment itself may affect renal function or bone density, it is necessary to select an appropriate drug if there is any risk factor. In a large Phase 3 trial comparing tenofovir AF and tenofovir DF over the 96-week treatment period, among those with any risk factor such as renal insufficiency, decreased bone density, old age, diabetes, or hypertension, patients treated with tenofovir DF had worsening renal function and bone density compared to patients treated with tenofovir AF (Compared to baseline, median changes in estimated glomerular filtration rate [eGFR] were -5.0 mL/min and -0.3 mL/min, respectively; bone mineral density changes were -3.290% and 1.233% [g/cm2 ], respectively) [224-227]. Therefore, it is recommended to avoid the use of tenofovir DF among patients with risk factors for renal dysfunction such as baseline eGFR <60 mL/min, proteinuria, albuminuria (urine albumin: creatinine ratio>30 mg/g), hypophosphatemia (<2.5 mg/dL), uncontrolled diabetes, or hypertension. If patients have a diagnosis of osteopenia or osteoporosis, need to be on chronic steroids treatment, or take other medications that may lower the bone density, other antivirals that affect bone density less should be considered over tenofovir DF (Fig. 4) [97].
In addition to tenofovir AF, entecavir and besifovir have less of an effect on renal function and bone metabolism. In a retrospective study comparing tenofovir DF and entecavir, the mean eGFR percentage decline of was significant in patients with tenofovir DF at week 48, 96, and 144. Also, bone density decline in the lumbar spine and hip was greater in patients with tenofovir DF than those with entecavir. In addition, osteopenia or osteoporosis prevalence (T score <-1.0) was much higher in the tenofovir DF group than the entecavir group at week 48, 96, and 144. Multivariate analysis showed the predictive factor for bone loss at week 144 was tenofovir DF use [397].
Besifovir, recently approved for use, had been evaluated in a clinical trial for safety in reduction of renal function and bone density. In a Phase 2b clinical trial, compared to entecavir, patients on besifovir didn’t have serum creatinine level increase by more than 0.5 mg/dL or a significant decrease in eGFR for a 48- week period [398]. During the two-year extended study period, grade 1 elevation of creatinine level (defined as increase of more than >0.3 mg/dL or 1.5–2.0 times the baseline creatinine) was observed in 35.5%, 17.9%, and 53.5% of the group receiving besifovir 90 mg, 150 mg, and 0.5 mg of entecavir, respectively. Hypophosphatemia was observed in 12.9%, 10.7%, and 10.0% of the same group, respectively, but there was no statistical difference among the three groups, and there was no treatment discontinuation or patients who developed symptoms of hypophosphatemia [335]. Therefore, besifovir is thought to have similar effect on renal function or serum phosphate level compared to entecavir.
Patients who developed renal dysfunction or decrease in bone density on treatment with NAs
If patient develop renal dysfunction or decrease in bone density while on NAs, one needs to find the causative factors to correct them and adjust the dose modification accordingly (Table 10). Or, there needs to be a review of the need for drug change (Fig. 4).
In a Phase 3 clinical trial comparing tenofovir AF and tenofovir DF, patients were given either treatment for 96 weeks each, and afterwards, all received tenofovir AF up until 144 weeks. During the first 96 weeks, regardless of presence of risk factors, renal function and bone density worsened among patients receiving tenofovir DF. After the antiviral was switched to tenofovir AF until the 144th week, both renal function and bone density improved [224-226,399]. In patients receiving tenofovir DF, eGFR decreased by -4.6 mL/min compared to the baseline at the 96th week. After switching to tenofovir AF, the eGFR reduction was 0.06 mL/min compared to the baseline at the 144th week, showing no significant difference between the two groups [224-227]. Patients receiving tenofovir DF showed greater reduction in spine and hip density during the 96-week compared to those receiving tenofovir AF. After switching to tenofovir AF, they showed significant improvement in bone density score at the 144th week compared to the score at the 96th week [399]. Therefore, it is thought that the reduction in renal function and/or bone density while on tenofovir DF may be improved by switching to tenofovir AF.
In a Phase 3 trial comparing besifovir with tenofovir DF for 48 weeks, patients receiving besifovir 150 mg had smaller reduction in the eGFR compared to those receiving tenofovir DF (-1.7 mL/min and -7.8 mL/min, respectively). After switching from tenofovir DF to besifovir and re-evaluated at the 96th week, the eGFR recovered close to the baseline. Therefore, the decrease in renal function while on tenofovir DF may be improved after switching to besifovir. In addition, specifically for bone density change, patients receiving besifovir 150 mg had a small reduction of the T-score change (reflective of bone density) of -0.02±0.44 at the end of the 48th week. Those receiving tenofovir DF had higher reduction of -0.09±0.87. Besifovir had significantly less effect on the bone density. In particular, after switching from tenofovir DF to besifovir, T-score reduction changed from -0.09±0.87 to -0.0±0.59, showing an improvement in the bone mineral density [334].
Therefore, during the NA treatment of CHB, if patients develop renal dysfunction or metabolic bone disease, and/or carry risk factors, appropriate drug change can be an option for overcoming the side effects of the NAs (Fig. 4).
[Recommendations]
1. Entecavir, tenofovir AF, and besifovir are preferred over tenofovir DF in treatment-naïve CHB patients with or at risk of renal dysfunction or metabolic bone disease. (B1)
2. Treatment can be switched to tenofovir AF, besifovir, or entecavir depending on treatment history, in patients on tenofovir DF with or at risk of renal dysfunction or metabolic bone disease. (B1)
3. NA doses should be adequately adjusted for creatinine clearance. Tenofovir AF is not recommended for CHB patients with creatinine clearance <15 mL/min. Besifovir is not recommended for those with creatinine clearance <50 mL/min, and tenofovir DF is not recommended for those with creatinine clearance <10 mL/min without renal replacement therapy. (B1)
Patients with acute hepatitis B
It is well known that more than 95% of adult patients with acute hepatitis B infection clear the virus without antiviral therapy and do not progress to chronic illness, but some patients go onto develop severe hepatitis [400,401]. Severe acute hepatitis B can be defined as having an international normalized ratio (INR) >1.5, severe jaundice, or progression to hepatic failure [402,403].
Regarding the need to antiviral therapy for acute hepatitis B, in the past, there were studies that suggested antiviral therapy could interfere with body’s natural immune response, prevent developing virus-specific neutralizing antibodies, and increase the risk of progression to CHB [404]. In a meta-analysis of 7 studies, involving 597 patients who received antiviral treatment for acute hepatitis B, those receiving lamivudine compared to placebo had higher risk of progression to CHB (OR, 1.99; 95% CI, 1.05–3.77) [405]. A randomized controlled trial of 71 patients with severe acute hepatitis B showed that those receiving lamivudine (n=31) had significantly lower serum HBV DNA after 4 weeks (3.7 log10 copies/mL) compared to those receiving placebo (n=40; 4.2 log10 copies/mL). After 12 months, there was no significant difference in the HBsAg-negative rates between the two groups (93.5% vs. 96.7%, respectively). Additionally, after 1 year, anti-HBs seropositive rate for those receiving lamivudine was 67.7%, lower than 85% for those receiving placebo, but there was no statistically significant difference between the two [406]. In another randomized controlled trial involving 80 patients, comparing lamivudine (n=40) and placebo (n=40), the anti-HBs seropositive rate was significantly lower for those receiving lamivudine at 62.5% compared to those receiving placebo (85%). However, those receiving lamivudine had significant improvement in blood levels such as coagulopathy or jaundice, and significantly lower mortality rate than those receiving placebo (7.5% vs. 25%, respectively) [407].
There is insufficient evidence from randomized controlled trials for early antiviral therapy in hepatitis B infection. In one cohort study, on the other hand, early administration of a potent antiviral medication was associated with prevention of acute hepatic failure as well as lower rate of liver transplantation ultimately and improved survival [402,408].
For the treatment of acute hepatitis B, lamivudine has been widely used based on results from several well-designed controlled trials [406,407,409,410]. In a study of entecavir comparing patients who received lamivudine (n=69) and entecavir (n=21), HBsAg seroconversion rates after 24 weeks were 23.18% for the lamivudine group and 52.38% for the entecavir group [411]. There is a case report of using tenofovir DF as a treatment for acute hepatitis B [412].
Patients on immunosuppression or chemotherapy
The progression of CHB is determined by the interaction between the virus and host immune response. Therefore, if the immune response is suppressed by immunosuppressive therapy or anticancer chemotherapy, the risk of reactivation increases [413].
Reactivation of CHB
Reactivation of hepatitis B indicates to the recurrence of active necrotizing inflammatory disease in patients in inactive phase of CHB or those recovered from previous active infection. It can be largely divided into two categories, “exacerbation of chronic HBV infection” for those with positive HBsAg and “relapse of past HBV infection” for those with negative HBsAg and positive anti-HBc [414]. In the latter category, patients who remained in an “occult HBV infection” status may show viral replication triggered by immunosuppression, leading to reverse seroconversion or seroreversion, with redetection of HBsAg [415-418]. The exacerbation of chronic HBV infection is defined in those with seropositive HBsAg as an increase of serum HBV DNA by more than 100 times the baseline level. The relapse of past HBV infection is defined as seroconversion of HBsAg negative to positive, or detection of serum HBV DNA from none to positive. Hepatitis flare is defined as serum ALT level more than 3 times the baseline level or increase by more than 100 IU/L [419,420].
Various rates of reactivation had been reported, but it is generally known to be about 20–50%. For an accurate diagnosis, liver damage related to chemotherapy, tumor metastasis, or hepatitis secondary to other viruses should be excluded. In many cases, patients are asymptomatic but occasionally present with jaundice, or are found in various stages such as decompensated liver diseases or even death [418,421-423]. Typical reactivation is seen by detection of serum HBV DNA during immunosuppression or chemotherapy, or elevation of serum ALT after stopping the immunosuppressive therapy. If the reactivation occurs during chemotherapy, it can lead to reduction or discontinuation of chemotherapy, adversely affecting the success of the chemotherapy [424-426]. There are risk factors, related to the virus, the host, and treatment, which are predictive of hepatitis B reactivation: virus factors include serum HBV DNA, HBeAg seropositivity, hepatocyte cccDNA, and PC/BCP mutation prior to the treatment; host factors include types of malignant tumors, male gender, young age, and high serum ALT levels; and, treatment factors include the type and intensity of immunosuppressant or chemotherapy regimen, HSCT, and/or solid organ transplantation [427]. The type and intensity of chemotherapy regimen related to the risk of hepatitis B reactivation can be classified into three categories: high risk group (reactivation risk of 10% or more), moderate risk group (reactivation risk between 1–10%) and low risk group (reactivation risk below 10%) (Table 11) [387,428,429].
Reactivation of hepatitis B during chemotherapy for hematologic malignancy: During the chemotherapy for lymphoma, hepatitis B reactivation is reported to be frequent with the rate up to 24–67%. It not only implies that the chemotherapy used for lymphoma is strong enough to cause bone marrow suppression, but also that patients with lymphoma have higher rates of seropositive HBsAg than those without lymphoma [422,430-432]. Rituximab, commonly used in combination with steroids for the treatment of lymphoma, is known to increase the risk of reactivation [433,434]. Rituximab therapy increased the risk of hepatitis B reactivation in patients with non-Hodgkin’s lymphoma who had seropositive HBsAg or seronegative HBsAg/seropositive anti-HBc combination (relative risk [RR], 2.14; 95% CI, 1.42–3.22; P=0.0003). In particular, in patients with seronegative HBsAg/seropositive anti-HBc combination, the use of rituximab therapy was associated with higher RR of reactivation (RR, 5.51) [435].
There was a significant difference in the reactivation of hepatitis B in patients with and without prophylactic antiviral therapy (13.3% vs. 60%) during treatment with rituximab [436]. Furthermore, prior to receiving chemotherapy (e.g. rituximab-cyclophosphamide, hydroxydaunorubicin, Oncovin, prednisone [R-CHOP]), screening for hepatitis B in all patients, rather than limiting to high-risk groups, resulted in a 10-fold reduction in hepatitis B reactivation rate and economic and survival benefits [437].
With other hematologic malignancies, if patients are receiving high-intensity chemotherapy prior to HSCT, the risk of reactivation is high [438,439]. In particular, in patients with seropositive HBsAg or seronegative HBsAg/seropositive anti-HBc awaiting high intensity chemotherapy prior to HSCT, antiviral therapy with a high barrier to resistance is recommended [440]. During immunosuppressive therapy or chemotherapy for hematologic disorders, for patients with evidence of hepatitis B infection, prophylactic treatment with lamivudine or entecavir can significantly lower the reactivation rate of hepatitis B [441,442].
Reactivation of hepatitis B during chemotherapy for solid tumors: Reactivation of hepatitis B in patients with solid tumors is known to be about 14–21%, but for those with breast cancer, it is higher at about 41–70%, which is thought to be related to the high dosages of breast cancer treatment agents as well as the use of anthracycline-based chemotherapy and steroids [426,443,444]. Steroids not only suppress immune system but directly stimulates the replication of HBV, thus raising the risk of reactivation. It is reported that the use of prophylactic antiviral agents in most solid tumors, such as breast and lung cancers, has significantly reduced the rate of hepatitis B reactivation and discontinuation of chemotherapy treatment [445-448].
Reactivation of hepatitis B during treatment for inflammatory bowel disease (IBD) or rheumatoid arthritis (RA): The reactivation of hepatitis B may also be associated with the use of TNF α inhibitors (infliximab, etanercept, adalimumab, etc.) for the treatment of IBD or RA [449-451]. In case of TNF α inhibitors and disease-modifying antirheumatic drugs (DMARDs) used for RA treatment, the rate of reactivation of hepatitis B was reported to be around 12.3% in patients with seropositive HBsAg [452]. In another study, the reactivation was reported in 39% of HBsAg-positive patients and 5% of anti-HBc-positive patients, and among those given antiviral prophylaxis, the reactivation rate was significantly lower [453].
Acute exacerbation of hepatitis B while on immune check point inhibitors: Recently, immune checkpoint inhibitors such as anti-PD-1 (nivolumab) and anti-CTLA4 (ipilimumab) therapy have been used in various carcinomas including liver cancer. Although there is a concern about the possibility of acute exacerbation of hepatitis B in relation to these therapeutic agents, there isn’t sufficient data yet, and the discussion regarding the consideration of future antiviral prophylaxis is necessary.
Start and end point of prophylactic antiviral treatment
When the reactivation of hepatitis B occurs, there is a risk of liver failure or even death. Therefore, the prevention is foremost important. Prior to starting an immunosuppressive therapy or chemotherapy, screening for HBsAg and anti-HBc is necessary. If there is no evidence of HBV infection in the past (with negative HBsAg and anti-HBc), HBV vaccination may be considered. In HBsAg positive cases, regardless of serum HBV DNA level, antiviral prophylaxis is recommended. Instead of waiting for the serum HBV DNA level to rise, administering an antiviral agent at the start of the immunosuppressive therapy or chemotherapy, or 7 days prior to the treatment start date, is reported to be more effective [448,454-456]. The end point of the prophylactic antiviral treatment should theoretically be continued until the immune system is adequately recovered, but there is lack of sufficient evidence to suggest a specific end point. It has been reported that the risk of HBV reactivation is high when prophylactic lamivudine is discontinued about 3 months after the end of chemotherapy. The risk is especially higher when the serum HBV DNA prior to the treatment is elevated (≥2,000 IU/mL) [457]. Therefore, when HBV is actively replicating before prophylactic antiviral therapy, following the present CHB treatment guidelines for the discontinuation of antiviral agents may prevent virus reactivation after treatment. However, regardless of the serum HBV DNA level prior to the treatment, reactivation still is reported more than 6 months after the completion of chemotherapy, so caution is required. Therefore, antiviral prophylaxis should be maintained for at least 6 months minimum after the chemotherapy is completed, and extension should be considered according to the chemotherapy risk. Especially, for patients receiving chemotherapy involving rituximab, it is recommended to extend the antiviral prophylaxis to at least 12 months after the completion of chemotherapy [458-460]. There is a need to closely monitor for relapse for at least 12 months after the prophylaxis is over.
On the other hand, reactivation of hepatitis B may occur not only when HBsAg is positive, as described above, but also when HBsAg is negative and anti-HBc is positive. Especially, when immunosuppressed, patients with seropositive anti-HBc alone had a higher risk of hepatitis B reactivation than patients with both seropositive anti-HBc and anti-HBs [387,461]. Thus, when patients, who are HBsAg negative and anti-HBc positive, receive rituximab-involving therapy or fall into a high-risk group such as being considered for HSCT for leukemia, antiviral prophylaxis should be considered regardless of HBV DNA detection or HBsAg seroconversion. For patients in a moderate or low-risk group of chemotherapy, HBsAg and HBV DNA levels should be periodically monitored (at intervals of 1–3 months) during or after chemotherapy to initiate antiviral treatment when hepatitis B reactivation is detected [387].
Treatment medications
Lamivudine is the most widely studied drug for prophylactic antiviral therapy. It is well known to significantly reduce reactivation, liver failure, and death according to randomized controlled trials of lymphoma patients in Hong Kong and Taiwan [431,439,454,462] However, lamivudine has been reported to be resistant even during prophylaxis. If the treatment duration is expected to be long, it is necessary to select a therapeutic agent with a high barrier to resistance considering the resistance rate [431]. In a retrospective study of lymphoma patients, the incidence of hepatitis and chemotherapy disruption due to HBV reactivation was significantly lower in the entecavir group than in the lamivudine group [463]. In a metaanalysis, entecavir prophylaxis was shown to prevent reactivation of hepatitis B more effectively compared to lamivudine prophylaxis [464]. Tenofovir DF was also reported to be effective for this purpose. In a recent randomized prospective controlled trial, under treatment with rituximab the rate of hepatitis B reactivation was 0% in the group prophylactically treated with tenofovir DF compared to 10.7% in the control group (P=0.091) [438]. It is necessary to conduct prospective studies on appropriate antiviral agents and treatment duration for various types of cancer, including solid tumors, and chemotherapeutic agents.
[Recommendations]
1. Screening for HBsAg and anti-HBc before immunosuppression or chemotherapy is recommended. If either is positive, HBV DNA testing should be performed. (A1)
2. If either HBsAg is positive or HBV DNA is detected, prophylactic antiviral therapy should be initiated before or at the start of immunosuppression or chemotherapy. (A1)
Antiviral agents should be selected based on comprehensive consideration of serum HBV DNA levels, the intensity and duration of immunosuppression or chemotherapy, and the cost. If baseline serum HBV DNA is high or long-term therapy is anticipated, tenofovir or entecavir is preferred. (B1)
3. In HBsAg-negative, HBV DNA-undetectable, anti-HBc-positive patients, serum HBsAg and HBV DNA should be monitored during high-risk immunosuppression/chemotherapy and antiviral therapy started when HBV reactivation occurs. (A1)
In particular, when a regimen includes rituximab, antiviral therapy can be initiated promptly at the start of immunosuppression or chemotherapy. (B1)
4. Prophylactic antiviral therapy should be maintained for at least 6 months after the termination of immunosuppression or chemotherapy and for at least 12 months after the termination of therapy if rituximab was included. (B1)
5. Periodic monitoring of serum HBV DNA is recommended during and after prophylactic antiviral therapy. (A1)
Liver transplant patients
Before the era of prophylactic antivirals, most patients with liver diseases related to hepatitis B experienced severe liver damage and had low survival rates from reactivation of hepatitis B after liver transplantation [465-471]. After the introduction of HBIG, a large cohort study of 372 HBsAg-positive patients reported that patients treated with HBIG for more than 6 months post-transplantation had significantly lower hepatitis B reactivation rates and higher long-term survival rates compared to patients treated for less than 6 months or who never received prophylaxis [472]. Lamivudine and HBIG combination therapy reduced the reactivation rate of hepatitis B in 1–2 years to less than 10%. From the cost-effective perspective, the combination therapy had better result compared to high-dose HBIG monotherapy (10,000 IU) [473-476]. In a meta-analysis, lamivudine and HBIG combination therapy has shown a 12-fold reduction in the reactivation rates and related mortality rates of hepatitis B virus compared to HBIG alone [477,478].
HBsAg-positive recipients
Lamivudine therapy without HBIG was associated with 40% reactivation rate of hepatitis B 4 years after liver transplantation [479,480]. When adefovir and lamivudine were administered together, no reactivation was noted during the 22-month follow-up period [481]. In a study using entecavir, during the 26–53 months follow-up period, HBsAg seronegative rate was 88–91%, over 98% had non-detectable level of HBV DNA, and reactivation rate was lower than when lamivudine alone was used [482,483]. In patients with non-detectable HBV DNA level at the time of liver transplantation, a study was conducted using a single agent of antiviral prophylaxis without HBIG was attempted. During the 8-year follow-up of 362 patients, HBsAg negative rate was 88% and hepatitis B reactivation rate was 2% [482]. In the same study group, 265 patients were given entecavir only and followed for 59 months, and there was no reactivation of hepatitis B [484]. However, in a meta-analysis of 519 patients from 17 studies, the combination of lamivudine and HBIG (6.1%) had a similar effect of suppressing reactivation compared to using entecavir or tenofovir DF alone (3.9%, P=0.51), but had a higher rate of reactivation compared to the combination therapy of entecavir or tenofovir DF with HBIG (1%, P<0.001) [485]. Therefore, to prevent reactivation after the transplantation, a potent antiviral agent combined with HBIG is recommended.
On the other hand, to reduce the use of expensive HBIG, there have been studies that use a small amount of HBIG or HBIG combined with an antiviral agent for a short term and then switched to an antiviral agent alone. Gane et al. reported in a study of 147 liver transplant patients, lamivudine combined with low dose HBIG (400–800 IU) resulted in 4% reactivation rate of hepatitis B over 5 years [486]. In another case where lamivudine and adefovir were used in combination with low-dose HBIG (400–800 IU) only at the beginning of transplantation and then switched to lamivudine and adefovir only, no reactivation was reported during the 57-month follow-up period [481]. When HBIG was used in combination initially, and then switched to entecavir or tenofovir DF alone, no reactivation was reported afterward [487,488]. Recently, based on the results of these studies, it is recommended to adjust the dose and the duration of HBIG use by assessing the hepatitis B reactivation risk of an individual patient at the time of the transplantation. One may consider using HBIG for a short duration in patients with non-detectable HBV DNA level at the time of transplantation [489-491]. Conversely, patients with a high risk of hepatitis B reactivation (e.g. Patients with detectable HBV DNA level, positive HBeAg, HCC, or HDV or HIV co-infection at the time of transplantation, or those with anticipated poor compliance with antiviral medications) may require a lifelong use of HBIG and anti-viral agent [492,493].
HBsAg-negative/anti-HBc-positive donors
If HBsAg-negative patients receive liver transplantation from HBsAg-negative/anti-HBc-positive donors, about 75% of the recipients are known to newly develop hepatitis B infection. It is reported to be dependent on the recipient’s HBV immunization status. Especially when the recipient is anti-HBs negative, the risk of new hepatitis B infection becomes higher [494-496]. After HBsAg-negative patients receive liver transplantation from HBsAg-negative/antiHBc-positive donors, when HBIG alone was used, more than 20% newly developed hepatitis B but when lamivudine alone was used, only 2–3% went onto develop hepatitis B. However, lamivudine and HBIG combination therapy did not show any additional preventive effect compared to lamivudine alone [494,497,498]. Therefore, if HBsAg-negative patient receive liver transplantation from HBsAg-negative/anti-HBc-positive donors, NA monotherapy is recommended to prevent new hepatitis B infection after transplantation [499]. However, in a retrospective study of 14 patients receiving liver transplantations from HBsAg-nega tive/anti-HBc-positive donors in Korea, 11 patients receiving HBIG monotherapy had 0% of new hepatitis B infection [500]. In a small retrospective study in Japan, HBIG monotherapy had 0% of recurrence rate of hepatitis B.501 Thus, in clinical practice, HBIG monotherapy may also be considered [500,501].
Treatment medications
In selecting an antiviral agent, lamivudine was shown to be cost-effective in a cost-effectiveness analysis using the Markov model [502]. In a study of NA monotherapy, including entecavir and tenofovir DF, the recurrence rate with these two agents were similar to lamivudine [502]. However, when lamivudine was used longterm after liver transplantation, over 50% had reported lamivudine resistance in 3 years [503-505]. This lamivudine resistance has negative effects, known to induce inflammatory changes and liver fibrosis between the grafts, or, in severe incidences, to cause death from the liver failure [504,506,507]. Therefore, as long-term antiviral therapy may be required, the use of antiviral agents with low resistance, such as entecavir and tenofovir, is recommended.
[Recommendations]
1. In hepatitis B-related liver transplant recipients, a combination of lifelong NAs and HBIG is recommended to prevent recurrence of hepatitis B after liver transplantation. (B1)
However, in the case of HBV DNA not detected before transplantation, modification of HBIG dose and duration may be considered after assessment of risk factors. (B2)
2. After liver transplantation, entecavir or tenofovir DF is recommended. (B1)
In cases of drug resistance, refer to the antiviral resistance chapter. (B1)
3. If the recipient is HBsAg negative and the donor is anti-HBc positive, administration of NAs is recommended after liver transplantation. (B1)
If NAs cannot be administered, HBIG monotherapy may be considered. (B2)
Non-liver organ transplant recipients
Non-liver solid organ transplantation
HBsAg-positive renal transplant recipients are at high risk for persistent viral activity or reactivation and have a significantly higher mortality rate due to liver-related complications such as liver cirrhosis and HCC [508]. Recent reports indicate that antiviral therapy increases the survival of HBsAg-positive renal transplant recipients [509,510]. Lamivudine therapy improves the survival of renal transplant recipients, but in cases of long-term administration, the drug resistance rate is 62% at 4 years [511]. Entecavir improves virological response, graft survival, and overall survival compared to lamivudine [512,513].
Small studies of HBsAg-positive heart transplant recipients have also demonstrated the safety and efficacy of NAs, and the use of entecavir or tenofovir DF is recommended to avoid liver failure due to drug resistance [514,515].
The risk of HBsAg reversion is low in recipients who are HBsAg negative and anti-HBc positive. In a Korean cohort study of 951 recipients of kidney transplantation recipients with seronegative HBsAg/seropositive anti-HBc, the HBsAg reversion rate was 5.6% for anti-HBs negative patients, but there was no difference between anti-HBs-positive and anti-HBc-negative recipients [516]. However, because HBsAg reversion followed by liver failure was reported in recipients with seronegative HBsAg/seropositive anti-HBc, hepatitis B reactivation should be monitored regularly. In patients who are ABO-incompatible and highly sensitized, rituximab is commonly used prior to renal transplantation. However, it can lead to liver failure in those with past HBV infection due to HBsAg reversion or HBV DNA redetection, albeit this risk is very low at low rituximab doses (200 mg) [516-518].
In recipients without prior HBV infection who receive a graft from an HBsAg-negative/anti-HBc-positive donor, the HBsAg positivity rate and anti-HBc detection rate are 0.3% and 3.2%, respectively [519]. However, in other studies, the HBsAg positivity rate of recipients of a transplanted kidney, heart, lung, or other organ from an HBsAg-negative/anti-HBc-positive donor did not differ from the rate for recipients receiving organs from anti-HBc-negative donors [520,521]. More studies are needed to determine whether either prophylactic antiviral treatment or HBIG reduces hepatitis B reactivation or HBV transmission in recipients of organs transplanted from a donor with past HBV infection.
Hematopoietic stem cell transplant
Patients with CHB who require HSCT for hematologic malignancies are immunosuppressed for a prolonged period due to the high-dose chemotherapy and hematological diseases itself. This increases the risk of hepatitis B reactivation and leads to a poor prognosis [522,523]. In small retrospective studies of HBsAg-positive recipients of allogeneic or autologous stem cell transplantation, prophylactic lamivudine treatment for 6-12 months significantly reduced the frequency of hepatitis B reactivation (5–10% vs. 45–50%) [439]. In another study, HBsAg-positive recipients of allogeneic stem cell transplants underwent prophylactic antiviral treatment for up to 6 months after termination of immunosuppressive therapy and were followed for 24 months after transplantation. The cumulative reactivation rate of hepatitis B was significantly higher in patients receiving lamivudine (24%) compared to patients receiving entecavir (2%). Recent meta-analyses have also demonstrated the efficacy of entecavir in preventing hepatitis B reactivation [524,525].
Hepatitis B reactivation is not infrequent in HSCT recipients with seronegative HBsAg/seropositive anti-HBc. In a prospective cohort study in which 62 HBsAg-negative and anti-HBc-positive allogeneic stem cell transplant recipients were followed for 48 weeks, the 2-year cumulative reactivation rate (detectable HBV DNA >10 IU/mL) was 40.8% [526].
[Recommendations]
1. All HBsAg-positive solid organ transplant recipients and HSCT recipients should start prophylactic antiviral treatment at the time of transplantation. (A1)
Entecavir or tenofovir DF is preferred for long-term treatment. (B1)
2. HBsAg-negative, HBV DNA undetectable, but anti-HBc-positive solid organ transplant recipients need regular follow-up to monitor the reactivation of hepatitis B. (B1)
3. HBsAg-negative, HBV DNA undetectable, but anti-HBc positive HSCT recipients are recommended to start prophylactic antiviral treatment at the time of transplantation. (B1)
Coinfection with other viruses
HCV coinfection
In patients with CHB, the anti-HCV positivity rate varies from 1.5% to 2.37% in Korea [527,528]. Patients with HBV/HCV coinfection have more severe necroinflammation and fibrosis than those with a monoinfection, as well as a high risk of cirrhosis and HCC [529,530]. When introducing direct-acting agents (DAA) in HBV/HCV coinfection, serum HBV DNA and HCV RNA levels should be analyzed to evaluate the replicative status of each virus. If the patient is HCV RNA positive, they should be treated as for HCV monoinfection. If the patient meets the criteria for antiviral treatment for CHB, proper treatment should be started promptly. Hepatitis B reactivation is possible during or after HCV treatment. One meta-analysis showed that detectible or increased levels of HBV DNA were reported in 14.1% of patients at 4–12 weeks after DAA treatment, and the incidence of elevated ALT (active hepatitis) was 12.2% [531]. In a prospective study of patients in Taiwan who were treated with ledipasvir/sofosbuvir, the HBV DNA detection rate was 83%, the HBV DNA 10-fold increase rate was 53%, and the active hepatitis rate was 6.3% [532]. According to the US Food and Drug Administration (FDA) Adverse Event Reporting System, two cases resulted in death, and 1 case resulted in liver transplantation. Therefore, serological tests, such as HBsAg and HBV DNA, are recommended before and during DAA therapy. Antiviral treatment for HBV should be considered if there is a marked HBV DNA elevation during DAA therapy [533]. Entecavir and tenofovir DF are recommended for the treatment of CHB in patients with HCV coinfection, but renal function monitoring is warranted if ledipasvir is used with tenofovir DF because it can increase the renal toxicity of tenofovir DF [534]. The drug interactions between HBV and HCV antiviral agents are summarized in the 2017 KASL Clinical Practice Guidelines for Management of Hepatitis C.
HIV coinfection
The incidences of cirrhosis and HCC are higher in patients with HBV/HIV coinfection than in those with HBV monoinfection [535]. The rate of HBV superinfection among Korean HIV patients is estimated to be approximately 5% [536]. With the changes in treatment strategies for HIV infection, the initiation of highly active antiretroviral therapy (HAART) has recently been recommended regardless of the number of CD4+ T cells. Therefore, simultaneous treatment for each virus is recommended for HIV and HBV coinfection. Therapeutic agents should be selected from the tenofovir-based antiretroviral regimen, and combination therapy with emtricitabine or lamivudine, which can inhibit the replication of both viruses, is recommended [537]. When HAART regimens are changed, antiviral agents that are effective against HBV should be included to avoid HBV reactivation, except in patients who meet the criteria for cessation of antiviral treatment for HBV.
HDV coinfection
It is estimated that ~20 million people are infected with HDV worldwide, and HDV infections are prevalent in Mediterranean countries, the Middle East, central Africa, and South America [538]. In one Korean study, the HDV coinfection rate was 0.3% in 940 patients with CHB, including 75 patients with HCC. In another study of 194 patients that included 64 CHB patients and 130 HCC patients, the rate was 3.6% [539,540]. The incidences of cirrhosis and HCC are higher in patients with HBV/HDV coinfection than in those with HBV monoinfection [541,542]. HDV infection can be diagnosed by detecting anti-HDV or HDV RNA in the serum or by detecting HDV antigens in liver tissues using immunohistochemistry.
The treatment goals are to inhibit HDV replication, normalize ALT levels, and improve histology findings. If the HBV/HDV coinfection patients meet the criteria for antiviral treatment for CHB, oral administration of CHB treatment is necessary to prevent the progression of liver disease. However, NAs for CHB are not recommended for the treatment of HDV infection in patients with HDV superinfection because they cannot inhibit HDV replication. Peginterferon alfa therapy was superior to high-dose interferon alfa therapy and that a combination therapy using an NAs and peginterferon alfa did not improve virological response compared to peginterferon alfa therapy alone [543]. The sustained virological response at 24 weeks after 48 week of peginterferon alfa therapy is 23–28%, and a sustained virological response can be predicted 24 weeks after the initiation of treatment by measuring serum HDV RNA levels [544-546]. However, relapse is frequent during longterm follow-ups, as seen in one study with an average follow-up of 4.3 years where sustained virological response was maintained at only 12% [547]. In a small study using extended peginterferon alfa therapy for 24 months, 47% of patients achieved sustained virological response during an average follow-up of 19.5 months after treatment, but further studies are needed [548].
[Recommendations]
1. CHB patients with HDV co-infection are recommended to be treated with peginterferon alfa for at least 1 year. (A1)
2. In CHB patients with HDV co-infection, initiation of NAs for CHB is recommended to prevent the progression of liver disease if either the indications for CHB treatment are met or liver cirrhosis is present. (B1)
Pregnant women and women preparing for pregnancy
Treatment in pregnant women and women preparing for pregnancy
Immunological changes during pregnancy: Pregnant women with chronic HBV infections are usually in the immune tolerance phase, and changes in the maternal immune system during pregnancy, such as a shift in the Th1-Th2 balance toward a Th2 response, lead to an increase in HBV DNA levels and a reduction in ALT levels [549,550]. These immune responses are restored after delivery causing a reduction in HBV DNA levels and ALT elevation, and therefore careful monitoring is needed [551,552].
Antiviral treatment: The optimal antiviral treatment strategy during pregnancy is based on the general principles for the treatment of CHB. However, all decisions regarding the timing and duration of treatment in pregnancy should include an analysis of the risks and benefits for both the mother and the fetus.
Peginterferon alfa preparations are preferred for patients who are planning a pregnancy as the period of treatment is more clearly defined. However, peginterferon alfa may cause fetal malformations; thus, it is contraindicated during pregnancy. Contraception must be emphasized during therapy and until 6 months after the cessation of therapy.
NAs may cause mitochondrial toxicity by inhibiting mitochondrial DNA replication [553]. The safety data of various NAs during pregnancy can be found at the Antiretroviral Pregnancy Registry (APR; http://www.apregistry.com). According to the APR, the rates of birth defects among the babies exposed to lamivudine or tenofovir DF in the first trimester (3.1% and 2.4% of live births, respectively) are similar to that in the general population (2.7%) as reported by the Center for Disease Control and Prevention birth defect surveillance system. Recently, further studies on the efficacy and safety of NAs have been carried out in pregnant women and infants. A small-scale prospective study of Chinese infants of patients who received telbivudine during pregnancy reported that mental development index and psychomotor developmental index at 12–24 months of age were significantly lower than those of the control group [554]. These results suggest that prenatal telbivudine exposure may lead to motor development delay in offspring. Meanwhile, infants exposed to tenofovir DF did not differ from those who were not exposed in terms of preterm birth, fetal anomalies, and poor development at birth and up to 6–12 months postnatally. In a large cohort study on tenofovir DF-based antiretroviral therapy to prevent MTCT of HIV infection in South Africa and the United States, there was no difference in the growth rate or the standard growth curve at 12 to 24 months after birth, regardless of the duration of antiretroviral therapy exposure or the duration of breastfeeding [555]. Based on the results of these clinical studies, tenofovir DF is preferred for treatment in pregnant women or patients preparing for pregnancy. Tenofovir AF requires further study.
Maintaining or altering the use of NAs: The decision as to whether to discontinue treatment with NAs in pregnant patients should be individualized. One retrospective study showed that 14% of pregnant patients with active CHB who did not receive antiviral therapy progressed to hepatic failure or maternal or fetal death. Another retrospective study reported moderate ALT elevations in 16% of pregnant patients who discontinued NAs pre-pregnancy and in 29–31% of pregnant and postpartum patients who discontinued NAs in the first trimester [556,557]. Therefore, if there is a high risk of complications in pregnant women and fetuses due to liver failure, appropriate maintenance of NAs should be considered. Taken together, if patients needed to maintain NAs, tenofovir DF can be continued in patients already taking tenofovir DF. The other agents should be switched to tenofovir DF in preparation for pregnancy or when a pregnancy is detected.
Prevention of MTCT of HBV with NAs
Influence of breastfeeding on infants: Several studies show the effects of breastfeeding on MTCT in HBsAg-positive pregnant women without antiviral treatment. In a prospective cohort study of 435 HBeAg-positive pregnant women, the HBsAg positivity rate of infants aged 8–12 months was 8.3% in the breastfeeding group and 9.2% in the formula milk feeding group, which was not significantly different [558]. Although studies on the safety of breastfeeding during the administration of NAs are very limited, recent studies in HIV-positive mother taking tenofovir DF have reported very low concentrations of the drug found in breast milk and that tenofovir is not absorbed through the intestines of infants. Therefore, considering the degree of liver disease in pregnant women and the risk of infants and young children, tenofovir DF can be carefully administered [559-561]. Based on this, the World Health Organization recommends the use of tenofovir DF during pregnancy and lactation [562].
Antiviral treatment for preventing MTCT: In the case of pregnant women with high serum HBV DNA levels (≥200,000 IU/mL), postnatal HBIG injections and sequential immunization for the prevention of MTCT have a high failure rate [563,564]. Therefore, there is a growing interest in lowering the MTCT rate through NAs during pregnancy.
- Lamivudine or telbivudine: In one prospective study of HBeAg-positive pregnant women with high serum HBV DNA levels (>107 copies/mL), they were treated with lamivudine from week 24 to week 32 in addition to neonatal passive-active immunoprophylaxis. The HBsAg-positivity rates of infants at 1 year after birth were significantly lower in the treatment group (0%, 0/94) compared to the placebo group (7.7%, 7/91) [565]. Another prospective study included pregnant with high serum HBV DNA levels (>106 copies/mL) who were treated with telbivudine starting at week 12–30 until birth in addition to neonatal passive-active immunoprophylaxis as the treatment group. The HBsAg-positivity rates of infants at 6 months after birth were also significantly lower in the treatment group (0%, 0/54) compared to the placebo group (8.6%, 3/35) [566].
- Tenofovir DF: In a non-randomized prospective study on administration of tenofovir DF starting at 30–32 weeks of gestation until 1 month postpartum, the HBsAg positivity rate of infants at 6 months of age was significantly lower in the experimental group (1.5% vs. 10.7%) [567]. In another non-blinded, randomized, prospective study in which tenofovir DF was administered over the same period, the per-protocol analysis showed that the HBsAg positivity rate of infants at 24 week of birth was significantly lower in the experimental group (0% vs. 7%) [568]. In a meta-analysis of ten studies using tenofovir DF, including the above studies, tenofovir DF was reported to reduce MTCT by 77% [569]. However, in a recent double-blind, randomized, prospective study, tenofovir DF was starting at 28 weeks of gestation until 2 months after birth, the difference in HBsAg positivity in infants at 6 months of age was insignificant (0% vs. 2%).570 It should be noted that in that study, hepatitis B vaccinations were performed 5 times after birth and the rate of MTCT was relatively low in the control group. In a recent meta-analysis of the two randomized prospective studies, there was no significant difference in the intention-to-treat analysis results, but the per-protocol analysis showed that tenofovir DF reduced MTCT by 98%.571 Therefore, the administration of NAs in pregnant women with serum HBV DNA levels of 200,000 IU/mL or more beginning at 24 to 32 weeks of gestation until 2 to 12 weeks postpartum can minimize the MTCT rate. However, in the case of pregnant women who do not meet into the general criteria for treatment for CHB, the decision whether to administer NAs to prevent MTCT should be individualized and consider the timing of drug administration, the timing of withdrawal, and the preference of the pregnant women. double-blind, randomized, prospective study, tenofovir DF was starting at 28 weeks of gestation until 2 months after birth, the difference in HBsAg positivity in infants at 6 months of age was insignificant (0% vs. 2%).570 It should be noted that in that study, hepatitis B vaccinations were performed 5 times after birth and the rate of MTCT was relatively low in the control group. In a recent meta-analysis of the two randomized prospective studies, there was no significant difference in the intention-to-treat analysis results, but the per-protocol analysis showed that tenofovir DF reduced MTCT by 98%.571 Therefore, the administration of NAs in pregnant women with serum HBV DNA levels of 200,000 IU/mL or more beginning at 24 to 32 weeks of gestation until 2 to 12 weeks postpartum can minimize the MTCT rate. However, in the case of pregnant women who do not meet into the general criteria for treatment for CHB, the decision whether to administer NAs to prevent MTCT should be individualized and consider the timing of drug administration, the timing of withdrawal, and the preference of the pregnant women.
[Recommendations]
1. The administration of NAs in pregnant women or in patients preparing for pregnancy should follow the general principles of CHB treatment. Therapy should be carefully chosen considering the short- and long-term effects on both the mother and fetus, and tenofovir DF is currently recommended. (B1)
2. Child-bearing is contraindicated during peginterferon alfa treatment, and it should not be used in pregnant women. (A1)
3. If a CHB patient becomes pregnant while taking an NA other than tenofovir DF, it is recommended to switch the medication to tenofovir DF, which is relatively safe for the fetus as well as for pregnant women and is not contraindicated during breastfeeding. (B1)
4. There are no limitations regarding breastfeeding in CHB patients without antiviral treatment. (B1)
5. For pregnant women with serum HBV DNA levels >200,000 IU/mL, administration of tenofovir DF is recommended for the prevention of MTCT (A2), starting at 24–32 weeks of gestation and stopping 2–12 weeks after delivery. (B1)
Children and adolescents
Providing HBIG and HBV vaccines to newborns of HBsAg-positive mothers within 12 hours of birth can prevent 90–95% of cases of perinatal infection [76,77]. Ninety percent of infants infected as neonates progress to chronic infection. Most children remain in the immune-tolerant phase until late childhood or adolescence; however, some children progress to the immune-active phase. The spontaneous HBeAg seroconversion rate in Korean children is 4.6%, 7.1%, and 28.0% for patients aged <6, 6–12, and >12 years, respectively [572]. Children who are in the immune-active phase are usually asymptomatic. If ALT is continuously elevated in children with CHB, serum HBV DNA levels should be examined to confirm viral replication. In a study of 104 children and adolescents in Taiwan with a median follow-up of 23.7 years, spontaneous HBeAg seroconversion could be predicted in patients with ALT levels >60 IU/L [573].
If long-term treatment is expected in children with CHB, a prudent decision should be made based on the adverse effects of the antiviral treatment and the potential for antiviral resistance to affect future therapies. The treatment window should not be missed because cirrhosis can occur even in the patient’s twenties, and HCC can occur later in life. The goals of CHB therapy are to suppress viral replication, reduce liver inflammation, reverse liver fibrosis, and prevent cirrhosis and HCC. Treating children in the immune-tolerant phase is not beneficial, and there is a high risk of developing antiviral resistance, which would limit treatment options later in life. However, a recent small-scale, randomized, prospective study reported that HBeAg seroconversion rates was 32.6% and HBsAg loss rates was 21.6% after 72 weeks of interferon-only or sequential lamivudine treatment [574].
Children with a persistently elevated serum ALT level should be evaluated for active viral replication, including measuring HBV DNA levels. Children should be considered for treatment when their serum ALT levels are ≥2 times the ULN for at least 6 months and their HBV DNA levels are ≥20,000 IU/mL (for HBeAg-positive children) or ≥2,000 IU/mL (for HBeAg-negative children). It is important to rule out other causes of ALT elevation, such as nonalcoholic fatty liver disease, before treatment and necessary to consider any family history of cirrhosis or HCC. Liver biopsy is helpful in the decision to treat, especially for children with moderate-tosevere necroinflammation or significant fibrosis (≥F2) [575].
Interferon alfa
Interferon alfa is approved in children older than 12 months, and its advantages include a finite duration of treatment and no development of antiviral resistance. A randomized controlled trial of interferon alfa therapy involving children with CHB aged 1 to 17 years found that 36% of those with a baseline ALT level of at least 2 times the ULN lost HBeAg by the end of treatment. HBsAg seroconversion occurred in 10% of the treated children [576]. Factors predictive of a positive response among children are age less than 5 years, low serum HBV DNA levels, and active inflammation as determined from a liver biopsy [577]. The recommended treatment regimen for interferon alfa is 6 million IU/m2 three times per week via subcutaneous injection for 24 weeks. The adverse effects include fever, flu-like symptoms, bone marrow suppression, depression, and transient growth delay. In a recent phase 3 study, pediatric and adolescent CHB patients between 3 and 16 years of age were treated with peginterferon alfa 2a for 48 weeks. The HBeAg seroconversion rate was significantly higher in the peginterferon alfa 2a group (25.7%) than in the control group (6%) at 24 weeks after the treatment completion, and the HBsAg disappearance rate, virological response rate, and ALT normalization rate were all significantly high [578].
Entecavir
Entecavir and tenofovir DF are potent NAs with a high barrier to resistance, and entecavir is considered the first-line therapy in children older than 2 years. In a randomized controlled study involving 180 children aged 2 to 17 years with HBeAg-positive CHB, the HBeAg seroconversion and HBV DNA <50 IU/mL rates at week 48 were significantly higher with entecavir than placebo (24.2% vs. 3.3%). The cumulative probability of entecavir resistance at 1 and 2 years was 0.6% and 2.6%, respectively. Entecavir showed no difference in safety compared with placebo [579]. A small-scale retrospective study of Koran pediatric and adolescent patients given entecavir reported second-year virological response (serum HBV DNA <20 IU/mL) and HBeAg seroconversion rates of 78.6% and 35.7%, respectively [580]. Entecavir is administered at a daily dose of 0.015 mg/kg (up to 0.5 mg).
Tenofovir DF
Tenofovir DF is approved for use in persons older than 12 years. A randomized controlled trial of tenofovir DF in adolescents aged 12 to 18 years reported that the rate of a virological response (HBV DNA <400 copies/mL) at week 72 was significantly higher in patients who received tenofovir DF (n=52) than in those who received placebo (n=54) (89% vs. 0%) [581]. No resistance to tenofovir developed during 72 weeks. The rate of grade 3/4 adverse events was higher among patients treated with placebo (24%) than those treated with tenofovir DF (10%). In a small-scale study in Korean children and adolescents using tenofovir DF, the virological response (serum HBV DNA <357 IU/mL) was 93.8% at week 48 and 100% at week 96 [582]. The rate of HBeAg loss associated with undetectable HBV DNA was 41.7% (5/12) at week 96. Tenofovir DF is administered at a daily dose of 8 mg/kg (up to 300 mg).
Lamivudine
Lamivudine is approved in children older than 2 years. A randomized controlled study of lamivudine involving children aged 2–17 years found that loss of HBeAg at 52 weeks of treatment occurred in 34% of those with a baseline ALT level of at least ≥2 times the ULN and that the resistance rate was 18% [583]. The antiviral resistance rate was 64% in children who received lamivudine for 3 years [584]. Other studies of Korean children found that the HBeAg seroconversion rates after 2 and 3 years of treatment were 65% and 70%, respectively. Loss of HBsAg was observed in 20% of children after 2 years of lamivudine treatment, and the resistance rates at 1 and 2 years of treatment were 10% and 23%, respectively [585,586]. Lamivudine is orally administered at a dose of 3 mg/kg/day with a maximum dose of 100 mg/day. If lamivudine resistance develops, it should be treated in accordance with the guidelines for antiviral resistance management in adults. In a small-scale study of lamivudine-resistant pediatric patients in Korea, the virological response rate at week 24 was significantly higher (P=0.029) in both lamivudine-adefovir combination therapy and in entecavir therapy alone compared to adefovir alone [587].
The preferable duration of NA treatment in HBeAg-positive CHB children and adolescents is at least 1 year from initiation of treatment and more than 1 year after HBeAg seroconversion. In HBeAg-negative CHB children, the optimal treatment duration is not clear, but the standard recommendations for adults may be followed.
[Recommendations]
1. In HBeAg-positive CHB patients with HBV DNA levels ≥20,000 IU/mL or HBeAg-negative CHB patients with ≥2,000 IU/mL, antiviral treatment is recommended if the ALT level is ≥2 times the ULN or if liver biopsy shows moderate to severe necroinflammation or significant fibrosis (≥F2). (A1)
2. Treatment with entecavir, tenofovir DF, or peginterferon alfa 2a is recommended in children and adolescent CHB patients. (A1)
3. If antiviral resistance develops during treatment, the recommendations for management of antiviral resistant CHB in adults given in the present guidelines should be followed. (B1)
Authors’ contribution
Yim HJ, directed the guideline committee, and outlined and supervised the manuscript writing and editing; Yoon EL edited the manuscript. All the committee members participated drafting the manuscript; Yim HJ (preamble, and supplementary material), Yoon EL (epidemiology, natural history, prevention, and diagnosis and initial evaluation), Kim JH (treatment goal and aims, monitoring during antiviral treatment, and cessation of treatment and monitoring after antiviral treatment), Sinn DH (treatment indication, monitoring of patients who are not indicated for treatment, treatment strategy, and definition and predictors of antiviral treatment response); Lee HW (therapeutic agents and management in patients with renal dysfunction or metabolic bone disease); Park JY (antiviral resistance and management of antiviral resistance), Lee JH (management according to treatment response and management in patients with hepatocellular carcinoma), Kwon JH (therapeutic agents and management in patients with renal dysfunction or metabolic bone disease), Park H (management in patients with acute hepatitis B, patients on immunosuppression or chemotherapy, and liver transplant patients), and Lee SH (management in non-liver organ transplant recipients, coinfection with other viruses, pregnant women and women preparing for pregnancy, and children and adolescents) contributed to the manuscript writing.
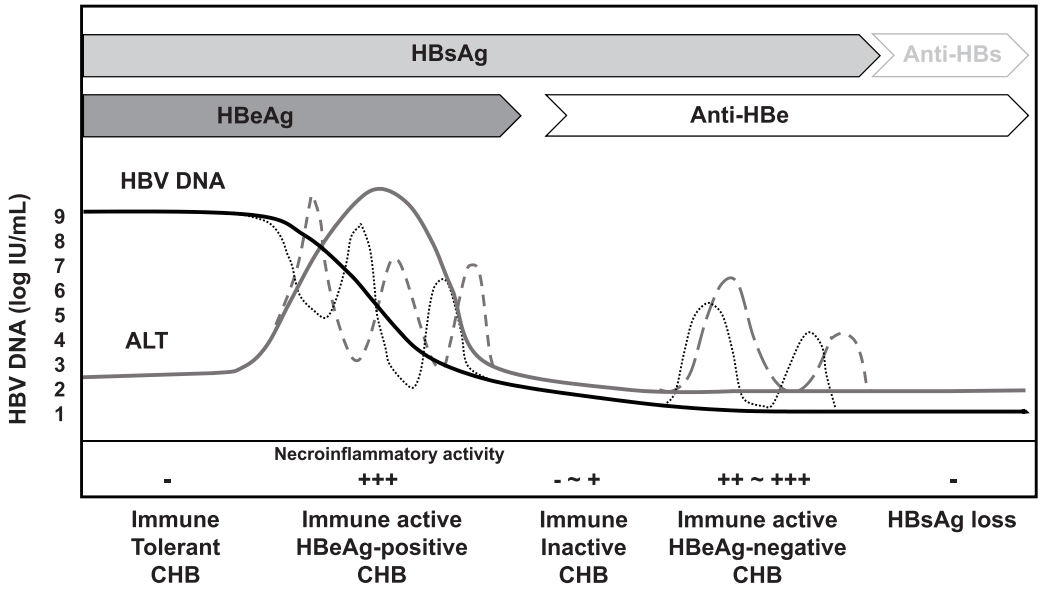

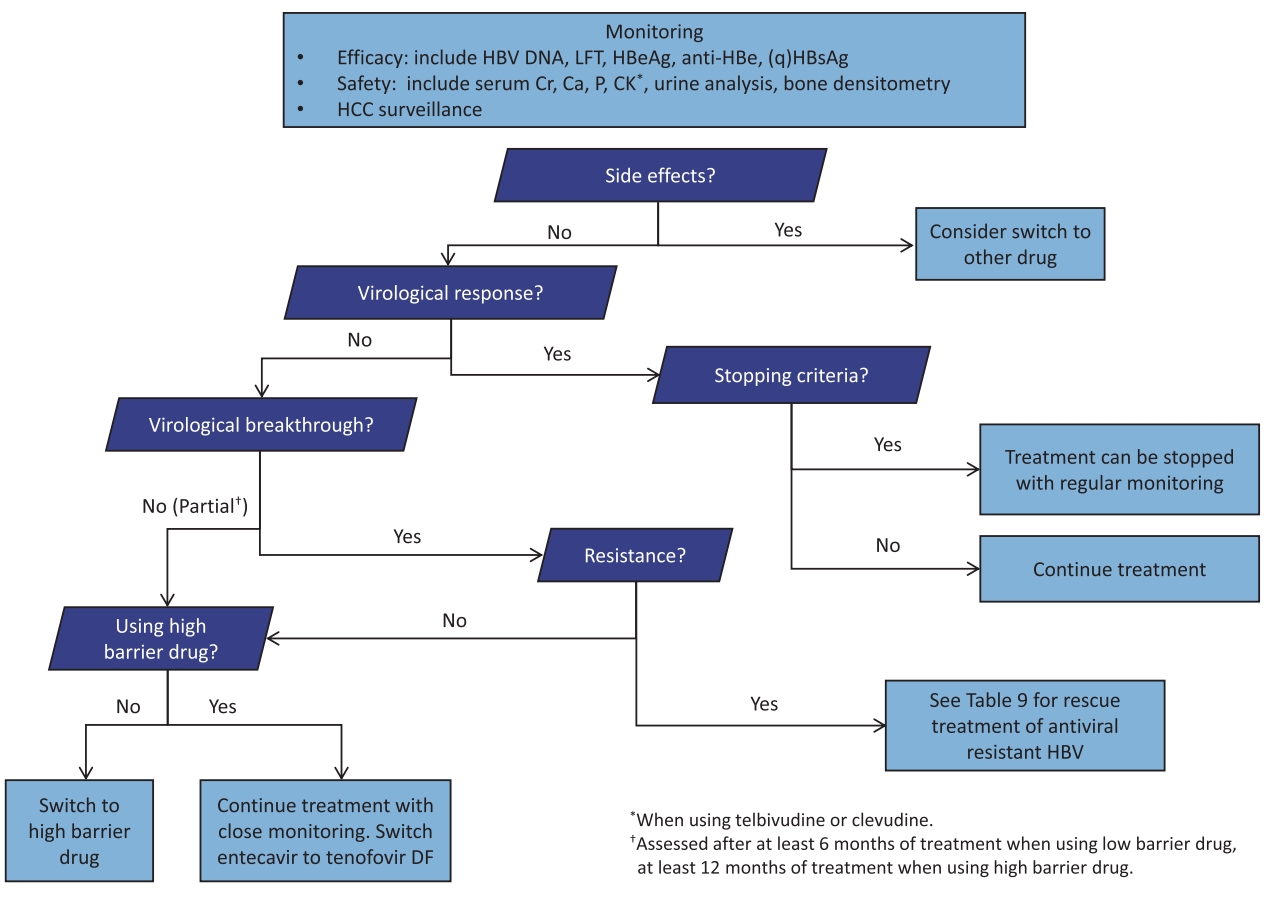

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Supplement
Supplement Print
Print




