


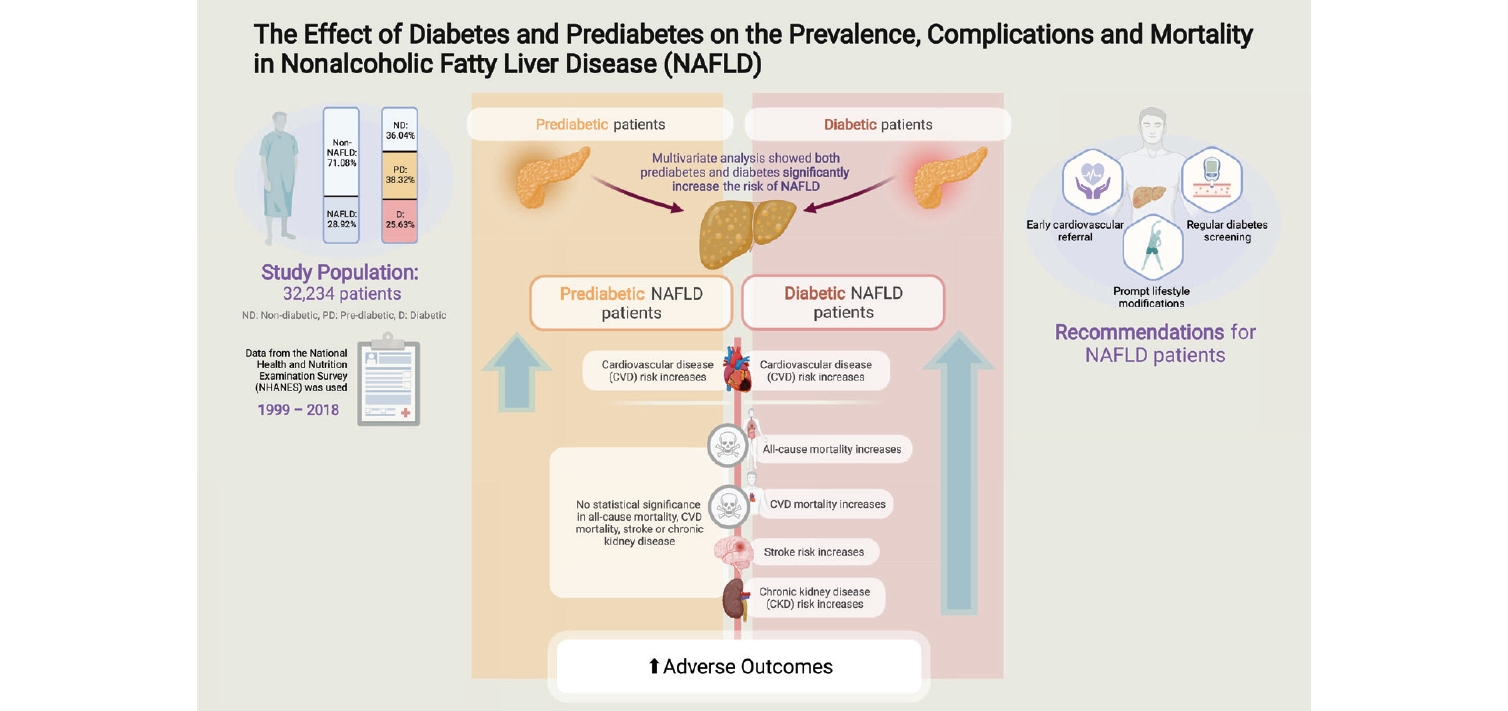
Graphical Abstract
INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) is the fastest growing cause of chronic liver disease and is estimated to affect 25ŌĆō33% of the global population [1-3]. The spectrum of NAFLD ranges from nonalcoholic fatty liver (NAFL) to nonalcoholic steatohepatitis (NASH), with the latter being characterized by the presence of lobar inflammation, ballooning, and fibrosis [4]. The presence of NAFLD is associated with an increased risk of systemic complications including the development of cardiovascular disease (CVD) [5,6], hepatocellular carcinoma [7], extrahepatic malignancy, and even depression [8]. In particular, the development and progression of NAFLD is closely associated with diabetes which is driven by insulin resistance and alterations in lipoprotein metabolism [9].
A recent meta-analysis estimated that up to half of individuals with NAFLD [10] have diabetes and the cumulative impact of both diseases synergistically increases the risk of both hepatic and extrahepatic events [9]. Pooled analysis of prospective studies has also shown a 2.19 increase in hazard ratio in the development of diabetes among patients with NAFLD, which supports a bi-directional relationship between both disease pathways [11]. Current consensus by the American Diabetic Association recommends that patients with type 2 diabetes with either elevation in liver enzymes or fatty liver on ultrasound imaging should be screened for NASH [12] or fibrosis. Several observational studies have also found that the presence of diabetes in NAFLD increases the risk of all cause and cardiovascular mortality compared to non-NAFLD diabetics [13,14].
While the awareness of diabetes and NAFLD is well established, prediabetes is a lesser-known entity in NAFLD. Prediabetes, a state of dysfunction albeit to a lesser degree of insulin sensitivity and impairment of ╬▓-cell function, has been found to be associated with NAFLD and its accompanying metabolic complications [15]. However, current literature mainly focuses on the prevalence and risk factors of NAFLD in prediabetes patients [16,17] with limited studies on clinical outcomes. Additionally, studies on the outcomes of prediabetes and diabetes with NAFLD are often conducted with reference to patients without NAFLD. Hence, we sought to examine the prevalence, outcomes, and impact of prediabetes and diabetes with reference to NAFLD without diabetes, using patients recruited in the United States National Health and Nutrition Examination Survey (NHANES) between 1999ŌĆō2018.
MATERIALS AND METHODS
This study analyses patients recruited between 1999ŌĆō2018 of NHANES. Briefly, the NHANES study was a cross-sectional survey platform that adopted a stratified, multistage, clustered probability sampling design which studies individuals representative of the general non-institutionalised population. Longitudinal outcomes of mortality are supplemented with data from the national death index. The NHANES study also involved a structured interview conducted in patientsŌĆÖ home, with subsequent standardised health examination conducted at a mobile examination centre for physical examinations and laboratory tests. The original survey was approved by the National Centre for Health Statistics Research Ethics Review Board. As the data used in the analysis is publicly available and de-identified, Institutional Review Board for the present analysis was not required.
Definition
The definition of NAFLD was adapted based on the American Association for the Study of Liver Disease (AASLD) guidelines for NAFLD. We defined NAFLD as the presence of steatosis is the absence of substantial alcohol use (Ōēź2 drinks a day in men, Ōēź3 drinks a day in women). The presence of steatosis in NAFLD was quantified with either Fatty Liver Index (FLI) or United States FLI (US-FLI) with a cut-off of Ōēź60 [18] and Ōēź30 [19], respectively. Diabetes was defined as glycohemoglobin (HbA1c) Ōēź6.5%, fasting plasma glucose Ōēź7 mmol/L, self-reported diabetes or the use of anti-diabetic medications. Prediabetes was defined as HbA1c between 5.7ŌĆō6.5% or fasting plasma glucose between 5.6ŌĆō7 mmol/L [20]. Non-invasive tests (NITs) for fibrosis include Aspartate Aminotransferase to Platelet Ratio Index (APRI), fibrosis-4 (FIB-4) index and NAFLD Fibrosis Score. These tests have accuracies of area under curve 0.74, 0.80 and 0.75ŌĆō0.82, respectively in the diagnosis of advanced fibrosis [21]. Lean patients were defined as having a body mass index (BMI) of <23 kg/m2 for Asians and a BMI <25 kg/m2 for other races. Patients were considered overweight when they had BMI between 23ŌĆō27.5 kg/m2 for Asians and 25ŌĆō30 kg/m2 for other races. Obese patients were defined as BMI >27.5 kg/m2 for Asians and BMI >30 kg/m2 for other races [22]. Hypertension was defined as a systolic or diastolic blood pressure Ōēź130/85 or the use of anti-hypertensive medications. Chronic kidney disease (CKD) was defined as the presence of kidney damage or an estimated glomerular filtration rate of less than 60 mL/min/1.73 m2 under the modification of diet in renal disease (MDRD) equation [23].
Statistical analysis
All statistical analysis was conducted in STATA (ver. 16.1; Statacorp, Chicaco, IL, USA) and Rstudio (ver. 4.0.3; PBC, Boston, MA, USA). Continuous variables were examined with Wilcoxon ranked sum test and Kruskal-Wallis analysis of variance while binary variables were examined with chi-square test and fisher exact where appropriate. A multivariate generalized linear model with a log link and robust variance estimator was use to examine the risk of binary events including risk of NAFLD, CVD, CKD, stroke [24]. A risk ratio (RR) was used to compare risk between both groups. The RR is a better approximation of events in common events and provides better interpretability compared to odds ratios [25]. Survival analysis was conducted with Cox proportional model for all-cause mortality and a Fine Gray sub-distribution hazard ratio (SHR) was calculated for cardiovascular mortality to account for competing risk. The multivariate model included variables that are common confounders of both all-cause and cardiovascular mortality in NAFLD including age, gender, race, BMI, previous myocardial infraction, and CKD.
RESULTS
Baseline characteristics and associated factors
A total of 32,234 patients were included in the analysis and 13,112 (28.92%) individuals were found to have NAFLD. A total of 20,139 individuals were non-NAFLD and non-diabetic. Of the 13,112 individuals with NAFLD, 12,932 had glycaemic measures quantified and of these, 4,661 (36.04%; 95% confidence interval [CI], 35.22% to 36.87%) were non-diabetic, while 4,956 (38.32%; 95% CI, 37.49% to 39.16%) and 3,315 (25.63%; 95% CI, 24.89% to 26.39%) were NAFLD patients with prediabetes and diabetes respectively (Fig. 1). A comparison between baseline characteristics of diabetic NAFLD, prediabetic NAFLD and non-diabetic NAFLD is summarized in Table 1. After adjusting for confounders including age, gender, race, and BMI, results from a generalized linear regression with robust estimator found older age (RR, 1.02; 95% CI, 1.02 to 1.03; P<0.01) and higher BMI (RR, 1.02; 95% CI, 1.02 to 1.03; P<0.01) to be associated risk factors of prediabetes in NAFLD. Hispanics (RR, 1.10; 95% CI, 1.04 to 1.15; P<0.01) and African Americans (RR, 1.07; 95% CI, 1.03 to 1.12; P<0.01) were also associated with an increased risk of prediabetes in NAFLD. Conversely, Caucasians (RR, 0.81; 95% CI, 0.78 to 0.84; P<0.001) and female gender (RR, 0.84; 95% CI, 0.82 to 0.86; P<0.01) were associated with reduced risks of prediabetes in NAFLD compared to non-diabetic NAFLD patients. Similarly, older age (RR, 1.04; 95% CI, 1.02 to 1.04; P<0.01), and higher BMI (RR, 1.04; 95% CI, 1.04 to 1.05; P<0.01) were found to be associated risk factors for diabetes in NAFLD. Female gender (RR, 0.82; 95% CI, 0.79 to 0.85; P<0.01) was associated with lower risk of diabetes in NAFLD. Comparisons of NITs for fibrosis can be found in Figure 2. The NITs were generally found to be the highest in diabetic individuals, although the presence of prediabetes also significantly increased NITs for hepatic steatosis and fibrosis compared to non-diabetic NAFLD. A multivariate generalized linear model with robust variance estimator found that both prediabetes (RR, 1.27; 95% CI, 1.22 to 1.32; P<0.01) and diabetes (RR, 1.38; 95% CI, 1.30 to 1.50; P<0.01) significantly increased the associated risk of NAFLD respectively.
Diabetic and prediabetic NAFLD vs. non-diabetic NAFLD
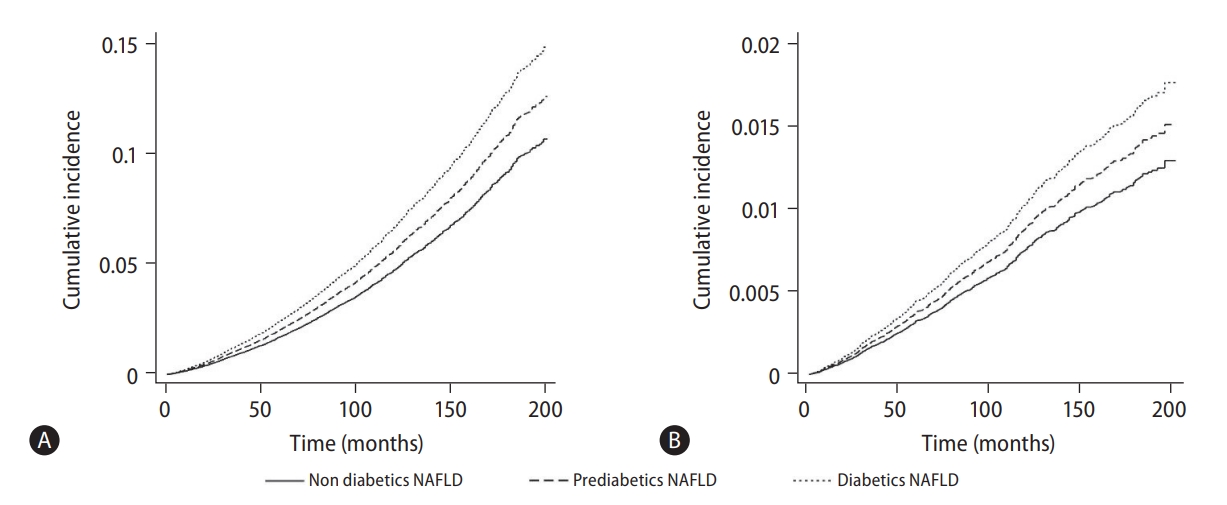
A multivariate generalized linear model was conducted to examine the risk of CVD, stroke, and CKD in NAFLD patients with prediabetes and diabetes (Fig. 3, Table 2). Both the presence of prediabetic NAFLD (RR, 1.20; 95% CI, 1.03 to 1.41; P=0.02) and diabetes NAFLD (RR, 1.90; 95% CI, 1.64 to 2.21; P<0.01) were associated with a significant increase in risk of CVD compared to non-diabetic NAFLD in an adjusted model. However, only diabetic NAFLD (RR, 1.66; 95% CI, 1.29 to 2.15; P<0.01) and not prediabetic NAFLD (RR, 0.89; 95% CI, 0.69 to 1.66; P=0.41) was associated with an increased risk of stroke compared to non-diabetic NAFLD in an adjusted multivariate analysis. Similarly, the risk of CKD was only significantly higher in diabetic NAFLD (RR, 1.47; 95% CI, 1.10 to 1.97; P=0.01) and not in prediabetic NAFLD (RR, 0.93; 95% CI, 0.81 to 1.09; P=0.41), compared to non-diabetic NAFLD. Survival analysis was conducted to examine the overall mortality and CVD mortality between diabetic NAFLD, prediabetic NAFLD, and non-diabetic NAFLD (Table 2). In a multivariate cox proportional model adjusted for age, gender, race, BMI, previous myocardial infraction, and CKD, diabetic NAFLD (HR, 1.60; 95% CI, 1.38 to 1.85; P<0.01; Fig. 4A) but not prediabetic NAFLD (HR, 1.14; 95% CI, 0.99 to 1.34; P=0.06; Fig. 4A) increased all-cause mortality compared to non-diabetic NAFLD. A competing risk analysis was conducted with a Fine Grey model for the SHR of CVD mortality with NAFLD. There was a significant increased risk of CVD mortality in diabetic NAFLD (SHR, 1.41; 95% CI, 1.02 to 1.94; P=0.04; Fig. 4B) but not in prediabetic NAFLD (SHR, 1.11; 95% CI, 0.82 to 1.52; P=0.49; Fig. 4B), compared to non-diabetic NAFLD.
Diabetic and prediabetic NAFLD vs. non-diabetic non-NAFLD
A sensitivity analysis was also conducted to examine the relative effect of prediabetic NAFLD and diabetic NAFLD with non-diabetic non-NAFLD (Table 2). Both prediabetic NAFLD (RR, 1.18; 95% CI, 1.03 to 1.35; P=0.02; RR, 1.17; 95% CI, 1.01 to 1.36; P=0.04) and diabetic NAFLD (RR, 1.85; 95% CI, 1.63 to 2.10; P<0.01; RR, 1.82; 95% CI, 1.60 to 2.08; P<0.01) were at an increased risk of CVD events and CKD, respectively. Stroke however was only associated with an increased risk in diabetic NAFLD (RR, 1.35; 95% CI, 1.26 to 1.43; P<0.01), but not in prediabetic NAFLD (RR, 0.98; 95% CI, 0.91 to 1.05; P=0.61) when compared to non-diabetic non-NAFLD. In survival analysis of overall mortality, there was no significant increased risk of overall mortality in prediabetic NAFLD compared to non-diabetic non-NAFLD (HR, 0.98; 95% CI, 0.87 to 1.10; P=0.98). However, diabetic NAFLD significantly increased the risk of overall mortality compared to non-diabetic non-NAFLD (HR, 1.35; 95% CI, 1.19 to 1.52; P<0.01). There was no increase in CVD mortality in prediabetic NAFLD (SHR, 1.00; 95% CI, 0.77 to 1.31; P=0.99) compared to non-diabetic non-NAFLD. However, diabetic NAFLD (SHR, 1.30; 95% CI, 0.99 to 1.71; P=0.06) resulted in a borderline non-significant increase in CVD mortality compared to non-diabetic non-NAFLD.
DISCUSSION
Evidence from meta-analyses have shown that NAFLD increases the risk of CKD, CVD, stroke, cardiovascular and all-cause mortality compared to the general population [13,14]. While insulin resistance is a core pathway in the pathogenesis of NAFLD [9], current large scale population studies [13,14] were conducted with reference to non-NAFLD diabetic patients, and were less focused on the effect relative to NAFLD without diabetes or have not accounted for competing risk [26] mortality. Moreover, the implications of prediabetes, a sign of metabolic perturbation, have not been examined among NAFLD patients. The present analysis of 23,987 patients adds to the literature by examining the synergistic effect of prediabetes and diabetes respectively in NAFLD compared to controls of non-diabetic NAFLD. In a population level analysis of NAFLD, 38.32% and 25.63% of NAFLD individuals had prediabetes and diabetes respectively which was associated with an increase in end organ complications in NAFLD.
Prediabetes is an intermediate state of hyperglycaemia with raised glycaemic parameters below the diabetic threshold [27]. Pathogenically, it differs from diabetes in its smaller extent of insulin resistance [28] and its potential for reversibility with lifestyle modification [29]. Additionally, it is a condition that is easily detectable in clinical settings. In our study, prediabetic NAFLD was found to increase only CVD but was not associated with a higher risk of stroke, CKD, overall mortality and CVD mortality. Importantly, only diabetics with NAFLD was associated with an increased risk of cardiovascular mortality compared to non-diabetic NAFLD in a competing risk analysis. Conventional wisdom suggests CVD disease to be the leading cause of death in NAFLD [30] and a previous meta-analysis conducted by Mantovani et al. [31] found a higher rate of fatal and non-fatal myocardial infarction among NAFLD patients with diabetes. CVD is similarly a major burden in diabetics with synergistic effect from both diseases, where patients with diabetes may experience adverse CVD events at an earlier age [32]. Previous studies have found up to 2.5 times increase in risk of CVD mortality in diabetic patients as compared to non-diabetic patients [33]. Considering the aggregate burden of diabetes and NAFLD, individuals with prediabetic and diabetic NAFLD may benefit from early referrals for cardiovascular risk assessment.
Despite the significant burden of NAFLD, current guidelines by the AASLD have not yet emphasised the need for routine assessment of glycaemic assessment in NAFLD individuals [34] without diabetes. NAFLD patients without diabetes at presentation may benefit from frequent monitoring of the Hba1c test. Prompt treatment with lifestyle modifications should be initiated to prevent progression from prediabetes to diabetes, which can significantly reduce the morbidity and mortality of these individuals. Lifestyle modifications are an essential aspect of both conditions and can potentially be synergistically employed with wearable technologies or electronic health applications. NAFLD patients with diabetes on the other hand may benefit from the use of glucagon-like peptide-1 receptor agonists (GLP1-RA [35]) or sodium-glucose co-transporter-2 inhibitors (SGLT2i [36]) in addition to metformin, with both agents showing significant reduction in fibrosis, steatosis and added benefits of cardiovascular protection in diabetics [37].
Limitations
The current analysis uses a population database from the NHANES study from 1999 to 2018. There are, however, several limitations to the results. Firstly, the quantification of alcohol intake is subject to recall bias. Next, FLI and US-FLI are NITs that only offer a gauge measure of steatosis but were deemed suitable measures in the setting of population studies. Glycaemic control is a flexible measure that can change with time, and the analysis only captured a snapshot of control at the point of inclusion. Despite adjusting for age, a younger age may also serve to be a confounder of the analysis since events of mortality may have yet to occur in younger individuals.
Conclusion
The current analysis reinforces the importance of glycaemic control in NAFLD. Individuals identified with NAFLD will benefit from frequent monitoring and prompt lifestyle changes should be initiated early in the course of disease to prevent the progression into type 2 diabetes which can significantly increase mortality and morbidity of the disease. Individuals with prediabetic and diabetic NAFLD might also benefit from early cardiovascular risk assessment. Pharmacological agents similarly should be targeted to improve glycaemic control, fibrosis and provide cardiovascular protection.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print





