


INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) is a leading cause of chronic liver disease globally [1]. It encompasses a spectrum ranging from simple hepatic steatosis to nonalcoholic steatohepatitis (NASH), which can progress to liver fibrosis and cirrhosis [2]. The global prevalence of NAFLD has been increasing over time, with a recent meta-analysis estimating that 32% of the adult population is afflicted by NAFLD [3]. This has occurred in tandem with the global obesity and diabetes epidemics [4,5]. NASH is now the fastest-rising cause of hepatocellular carcinoma worldwide [6,7] and is also the fastest-rising indication for liver transplantation in the United States [8].
INCIDENCE OF NAFLD
A recent meta-analysis by Riazi et al. [3] estimated the incidence of NAFLD at 46.9 cases per 1,000 person-years. The incidence of NAFLD was higher in males (70.8 cases per 1,000 person-years) vs. females (26.9 cases per 1,000 person-years, P<0.0001). However, all included studies were conducted in Asia, hence it is unclear whether these data are generalizable to other parts of the world. A previous meta-analysis published in 2016 had estimated the NAFLD incidence at 52.34 per 1,000 person-years in Asia and 28.01 per 1,000 personyears in Israel [9]. Another meta-analysis focused on NAFLD in Asia reported an incidence of 50.9 per 1,000 person-years, with the highest incidence of 63 per 1,000 person-years in mainland China and the lowest incidence of 29 per 1,000 person-years in Japan (Fig. 1) [10]. The NAFLD incidence in South Korea was around 45 cases per 1,000 person-years [10,11]. Taken together, the estimates for NAFLD incidence in Asia remain consistent across several meta-analyses (Table 1).
PREVALENCE OF NAFLD
Riazi et al. [3] pooled data from 72 studies (1,030,160 individuals) and estimated that the global prevalence of NAFLD in adults was 32% (Table 2). The prevalence was higher in males than females (40% vs. 26%, P<0.0001). The prevalence of NAFLD increased from 26% in studies from 2005 or earlier to 38% in studies from 2016 or beyond. However, data from this study by Riazi et al. [3] requires cautious interpretation, as data were available from only 17 countries, hence it is unclear if the estimates from this study are a true reflection of ŌĆśglobalŌĆÖ prevalence. The relative lack of studies emphasizes the need to improve data collection from regions such as Africa, Oceania, and South America, where data was lacking. Le et al. [12] also pooled data from 245 studies (2,699,627 individuals) and estimated the global prevalence of NAFLD at 29.8%, which is consistent with RiaziŌĆÖs findings. Likewise, in this study, there was limited or no data from Africa, Oceania, and North and South America.
Asia
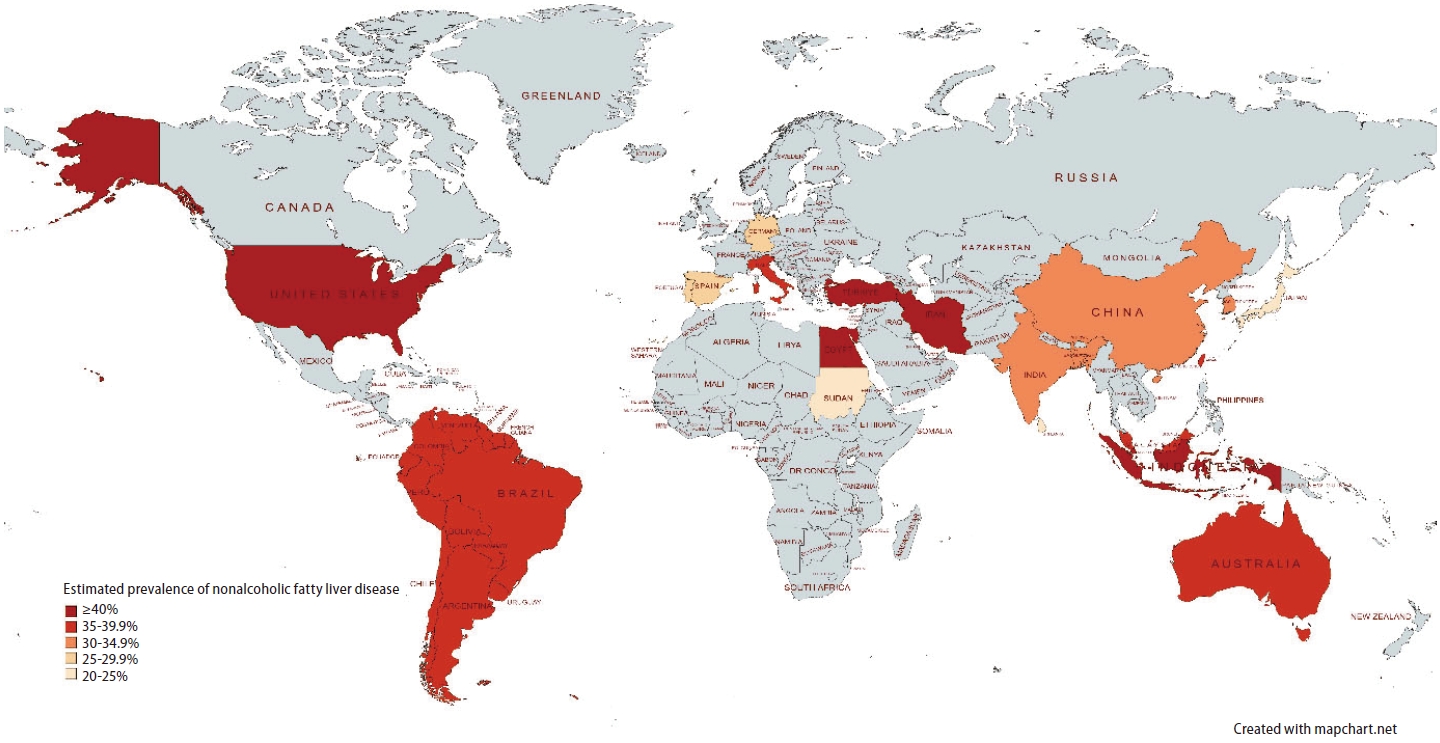
The prevalence of NAFLD varies substantially by region (Fig. 2). The overall prevalence of NAFLD in Asia is approximately 30%. A meta-analysis by Le et al. [12] conducted a literature search in 2019 (182 studies with 2,385,999 individuals) and estimated NAFLD prevalence in Asia at 30.5%. A recent meta-analysis by Riazi et al. [3] which included 63 studies (1,000,681 individuals) found that NAFLD prevalence in Asia was 31.6%. This is consistent with a previous meta-analysis by Li et al. [10] which reported NAFLD prevalence in Asia to be 29.62%.
The prevalence of NAFLD within Asia is highly variable as it encompasses countries with a wide spectrum of ethnicities and socioeconomic factors. Among Asian subregions, Southeast Asia had the highest NAFLD prevalence of 42%. Among Asian countries with more than 3 studies available, Li et al. [10] determined that the highest pooled NAFLD prevalence was in Iran (38.07%), and the lowest pooled NAFLD prevalence was in Japan (22.28%). Riazi et al. [3] determined similar results and found that Iran had the highest NAFLD prevalence (40.8%), followed by Taiwan (36.1%), South Korea (34.6%), and China (32.5%). On the other hand, Japan had a strikingly low NAFLD prevalence of 22.3%, which may be related to a low prevalence of obesity.
In China, a meta-analysis by Wu et al. [13] estimated a NAFLD prevalence of 29.88%, and another study by Zhou et al. [14] estimated that NAFLD prevalence was 29.2%. NAFLD prevalence in South Korea is also approximately 30%ŌĆöa meta-analysis by Im et al. [15] reported a NAFLD prevalence of 30.3%, and Li et al. [10] reported a similar prevalence of 32.9% [11]. A large cross-sectional study of 571,872 Korean males in their early 20s found that even among young adult males, NAFLD prevalence was 13.47%, with an increase from 10.66% in 2015 to 16.44% in 2021. There was a higher prevalence of metabolic risk factors such as hypertension, hypercholesterolemia, and hyperglycemia during the same period [16]. Another study utilizing data from Korea National Health and Nutrition Examination Survey found that NAFLD prevalence increased from 18.6% in 1998ŌĆō2001 to 21.5% in 2016ŌĆō2017, and there was a higher prevalence of obesity and diabetes over the same period [17]. These suggest that the increasing NAFLD prevalence may be driven by an increase in metabolic risk factors. Ito et al. [18] reported a comparatively lower NAFLD prevalence of 25.5% in Japan, in line with the findings by Li and Riazi. This could be attributed to a lower prevalence of obesity and diabetes in Japan compared to other countries [19,20], and may be related to a diet that is traditionally lower in fat and red meat [21].
In South Asia, India had a NAFLD prevalence of 25.7ŌĆō32.74%, Bangladesh had a NAFLD prevalence of 26.2ŌĆō33.86%, and Sri Lanka had a NAFLD prevalence of 24.74% [3,10]. In Southeast Asia, Li et al. [10] reported that NAFLD prevalence was 38.5% in Malaysia, 40.43% in Singapore, and 51.04% in Indonesia. Data from Central Asia is lacking, but the Global Burden of Disease Study (GBD) 2019 reported NAFLD prevalence in Central Asia increased from 12.4% in 1990 to 19.7% in 2019, although these estimates require cautious interpretation as the Global Burden of Disease Study relied on complex modeling and past trends when data was limited [22].
A distinct feature of the NAFLD epidemic in Asia is the high prevalence of lean NAFLD (body mass index [BMI] <23) and non-obese NAFLD (BMI <25) [23]. Up to 19% of non-obese Asians have NAFLD [24], which may be contributed to a higher percentage of visceral adiposity in Asians compared to other ethnicities [25]. Visceral adiposity plays an important role in atherogenic dyslipidemia and insulin resistance. It is a major risk factor for type 2 diabetes and has been implicated in the development and progression of NAFLD [26]. Asians also tend to develop diabetes at a younger age and lower BMI level, resulting in a longer duration of disease and increased likelihood of complications [27-29]. Worryingly, emerging data suggest that individuals with lean NAFLD may be at a higher risk of progressive liver disease, but this hypothesis requires validation [30].
Europe
Meta-analyses by Le and Riazi had similar estimates of the prevalence of NAFLD in Europe at 30.9% (11 studies with 15,062 individuals) [12] and 32.6% (7 studies with 14,111 individuals) [3], respectively. Another meta-analysis by Cholongitas et al. [31] pooled data from 17 studies (85,203 individuals) and estimated NAFLD prevalence in Europe to be 26.9%. Cholongitas also found that NAFLD prevalence in Mediterranean countries at 23.9% compared to non-Mediterranean countries at 28.5%, although the difference was not statistically significant.
Within Europe, Turkey had the highest NAFLD prevalence at 48.4%, followed by Italy at 38.2%. Germany, Portugal, and Spain had NAFLD prevalence between 25ŌĆō27% [3]. A cross-sectional study utilizing data from a large population-based cohort in France found that NAFLD prevalence in France was 18.2% [32]. A study involving individuals from population-based studies in Russia reported that NAFLD prevalence was 40% in the Ural Eye and Medical Study (UEMS) (5,852 individuals), and 69.8% in the Ural Very Old Study (UVOS) (1,130 individuals) [33]. However, it should be noted that in the UVOS, individuals were older with minimum age of 85 years, and methods for diagnosis of NAFLD differed between studies as well.
North America
Based on subgroup data from 4 studies (18,356 individuals), Le et al. [12] estimated that the prevalence of NAFLD in North America was 35.3%. More recently, NAFLD prevalence was reported at 47.8% in the meta-analysis by Riazi which included 2 large studies with 15,178 individuals from the USA [3]. This is driven by a high prevalence of obesity in the USA. In North America, Hispanics have the highest NAFLD prevalence, followed by non-Hispanic Whites and non-Hispanic blacks [34-39]. Based on data from National Health and Nutrition Examination Surveys (NHANES) 2017ŌĆō2018, NAFLD prevalence was estimated at 63.7% in Hispanics, 56.8% in non-Hispanic whites, and 46.2% in non-Hispanic blacks [37]. This could be attributed to genetic factors like the patatin-like phospholipase domain-containing protein 3 (PNPLA3) mutation, which is associated with elevated risk for hepatic steatosis and NASH, occurring more frequently in Hispanics [40,41]. This could also be related to metabolic factors like the higher prevalence of central adiposity and insulin resistance in Hispanics compared to non-Hispanic whites [34,42]. Lower serum triglyceride levels in African-Americans may also contribute to reduced NAFLD prevalence [38].
South America
A meta-analysis comprising 19 studies (5,626 individuals) by Rojas et al. estimated the prevalence of NAFLD in South America at up to 59% [43]. Notably, the majority of the studies included in this meta-analysis were hospital-based studies and included patients with risk factors for NAFLD, hence the results may not have been fully representative of the general population. Le et al. [12] pooled data from 3 studies (5,716 individuals) and determined that South America had the greatest estimated NAFLD prevalence among the continents at 35.7%. This may be due to a combination of genetic susceptibility and a greater prevalence of metabolic risk factors [44]. There is a high prevalence of PNPLA3 genetic polymorphism in the general population, especially among individuals with Native American ancestry [45-47]. Furthermore, obesity is extremely common in the regionŌĆöa cross-sectional study across 4 geographical regions found that central obesity was highest in South America [48]. Type 2 diabetes has also been rising in prevalence in South America [49]. Data from the meta-analysis by Le showed that compared to other regions, NAFLD individuals in South America had a higher likelihood of having diabetes and higher mean cholesterol levels [12]. In addition, physical activity is often inadequateŌĆöLatin America was ranked as the top region for physical inactivity, with a third of the population experiencing a lack of physical activity [50].
Africa
There is a paucity of data from Africa on the epidemiology of NAFLD. A meta-analysis estimated the prevalence of NAFLD in Africa at 13.5%, ranging from 9% in Nigeria to 20% in Sudan [51]. More recently, NAFLD prevalence was reported at 28.2% in the meta-analysis by Le, and 56.8% in the meta-analysis by Riazi [3,12]. Of note, the meta-analysis by Riazi only included 1 study from Egypt. The wide variation in estimates of NAFLD prevalence is likely related to a lack of reliable data from Africa [52,53].
Oceania
Likewise, there is scarce data from Oceania on the incidence and prevalence of NAFLD. Population-based studies using fatty liver index have demonstrated NAFLD prevalence of 35.7ŌĆō38% in Australia [54,55]. There are no population-based studies on NAFLD prevalence using imaging modalities such as ultrasound [56].
PROJECTIONS IN THE PREVALENCE OF NAFLD
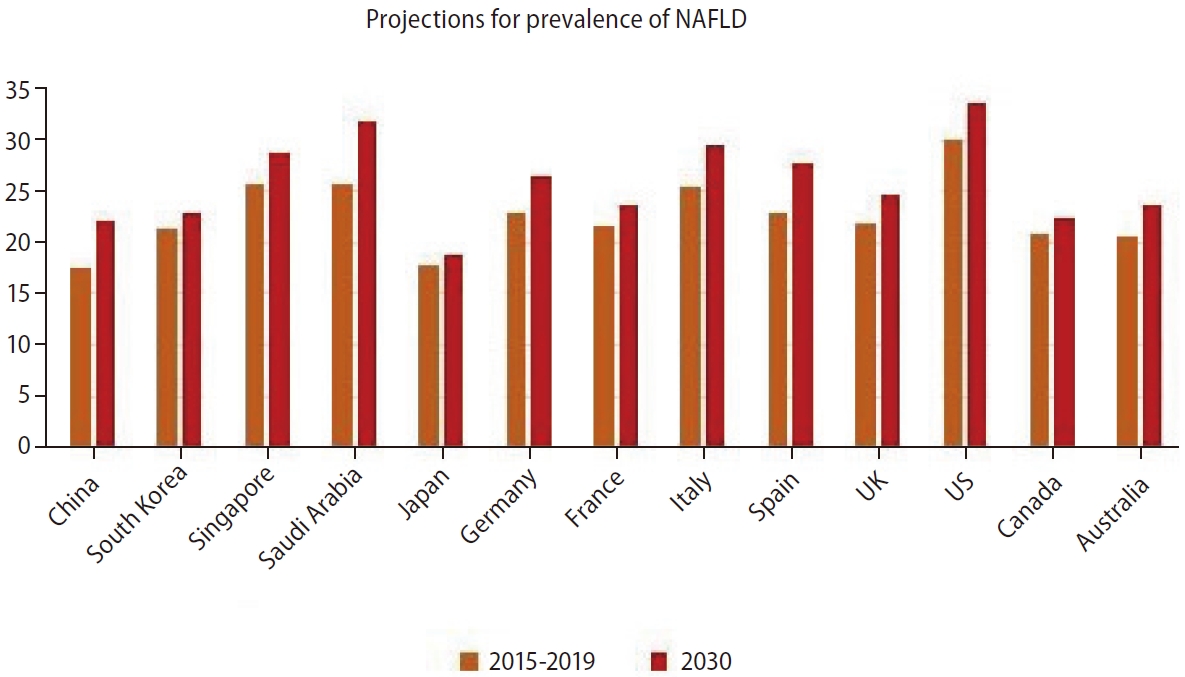
Based on mathematical modeling studies, the burden of NAFLD and NASH will continue to increase over the next 10 years worldwide (Fig. 3). The global prevalence of NAFLD is forecasted to reach 55.4% by 2040 [57]. It was estimated by Estes et al. [58] that China would have the greatest overall and relative increase in NAFLD prevalence, with the estimated number of individuals afflicted by NAFLD increasing from 243.67 million in 2016 to 314.58 million in 2030. Comparatively, Japan was forecasted to have the lowest increment in NAFLD population from 22.67 million in 2016 to 22.74 million in 2030, with an estimated prevalence of 18.8% in 2030 [58]. A similar modeling study including 4 other Asian countries predicted that Singapore would have the highest relative increase of 20% in NAFLD cases, from 1.49 million in 2019 to 1.8 million in 2030, with an expected prevalence of 28.7% in 2030 [59]. South Korea was predicted to have the lowest relative increment of 6% from 10.95 million in 2019 to 11.64 million in 2030, with an expected prevalence of 22.8% in 2030 [59]. These models were based on data on obesity prevalence and were predicated on the assumption that changes in NAFLD prevalence would occur in concordance with changes in obesity prevalence. In the Middle East, it was projected that in Saudi Arabia, NAFLD cases would increase from 8.45 million in 2017 to 12.53 million in 2030, with an expected prevalence of 31.7% by 2030; in the United Arab Emirates (UAE), NAFLD cases were projected to increase from 0.255 million in 2017 to 0.372 million in 2030, with an expected prevalence of 30.2% by 2030 [60].
In Europe, a modeling study found that between 2016 to 2030, the number of NAFLD cases could potentially increase from 13.98 million to 16.05 million in France; 18.45 million to 20.95 million in Germany; 15.22 million to 17.42 million in Italy; 10.53 million to 12.65 million in Spain; and 14.08 million to 16.92 million in the United Kingdom (UK). By 2030, the estimated prevalence of NAFLD was forecasted to be highest in Italy (29.5%), followed by Spain (27.6%), Germany (26.4%), the UK (24.7%), and France (23.6%) [58].
This trend of increasing NAFLD prevalence has also been predicted to occur in North America and Australia. A modeling study based on data from the US predicted that the number of individuals with NAFLD would increase by 21% from 83.1 million in 2015 to 100.9 million in 2030, reaching an expected prevalence of 33.5% in 2030 [61]. A separate modeling study from Canada projected that NAFLD individuals would rise by 20% from an estimated 7.76 million in 2019 to 9.31 million in 2030 [62]. A similar study from Australia estimated that NAFLD cases would increase by 25% from 5.55 million in 2019 to 7.02 million in 2030, and NAFLD prevalence was expected to rise from 22% to 23.6% in 2030 [63]. Taken together, these data suggest that the prevalence and burden of NAFLD is likely to increase across multiple world regions if current trends are left unchecked. This serves as a call to action for greater political will and resources directed toward combating metabolic risk factors for NAFLD, at a regional and global level [64,65].
CONCLUSION
In summary, the global burden of NAFLD is substantial and is projected to increase. It is important to maintain and increase data collection from all world regions to improve the understanding of the burden of disease associated with NAFLD and NASH worldwide. Improving our understanding of the burden of NAFLD can facilitate the development of healthcare policies and strategies to slow this epidemic.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





