


Graphical Abstract
INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease in which steatosis is present in greater than 5% of the liver cells. NAFLD is a progressive disease in up to 20% of patients, but until recently, there has been a paucity of non-invasive tests for both steatosis and fibrosis diagnoses, so our understanding of progressive NAFLD has mostly come from those who have undergone a liver biopsy or abdominal imaging which limits large population studies [1-16].
As such, our understanding of the factors associated with adverse outcomes of NAFLD, such as race and ethnicity, is evolving. From prior studies conducted in the United States, Hispanic origin is associated with the highest risk of having NAFLD, while those of non-Hispanic Black origin have a lower risk of having NAFLD but a higher risk for adverse outcomes, including mortality [17-23]. However, the majority of prior studies on race, ethnicity, and NAFLD used data from large population-based databases that preclude survival analysis or were limited by the availability of follow-up outcomes.
Therefore, the purpose of this study was to use individual patient-level data from a large medical center to provide a longitudinal picture of the role of ethnicity in patients residing in the United States who have NAFLD.
MATERIALS AND METHODS
Study design and study population
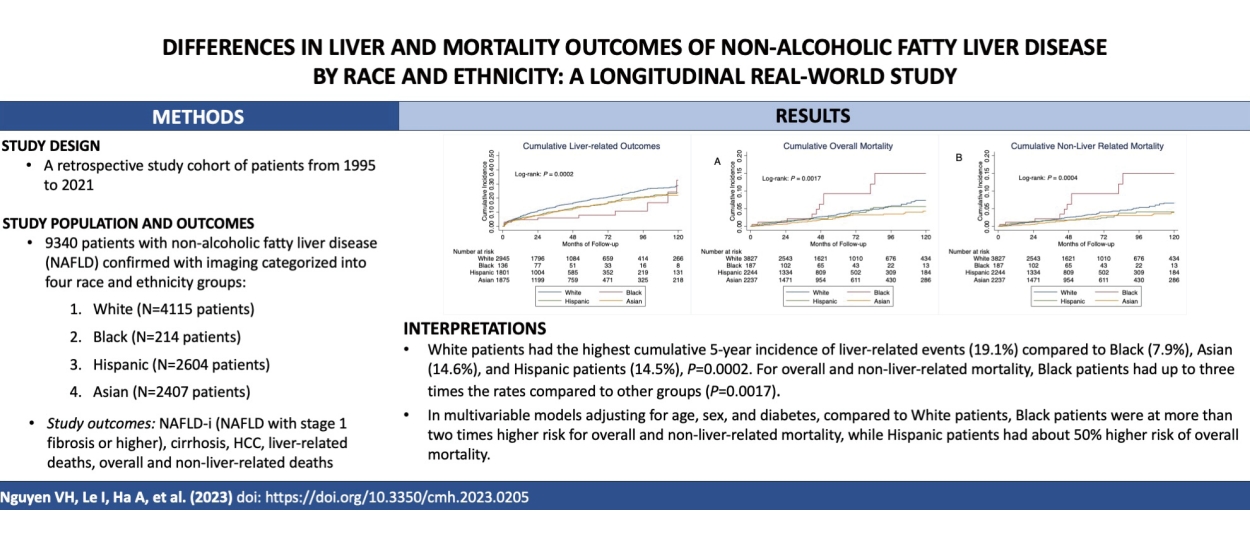
We retrospectively identified patients with NAFLD at Stanford University Medical Center, Palo Alto, California, USA, between 1995 and 2021. NAFLD was confirmed by the presence of hepatic steatosis in abdominal ultrasound, computed tomography, or magnetic resonance imaging on manual chart review. We excluded patients with significant alcohol use and/or concurrent viral hepatitis, autoimmune hepatitis, alpha-1 antitrypsin deficiency, hemochromatosis, or WilsonŌĆÖs disease. Data on race and ethnicity are extracted from the demographics section in the electronic medical records, which are self-reported by the patients. Patients with unknown, mixed race and ethnicity, or race and ethnicity other than White, Black, Hispanic, or Asian, were excluded due to small numbers. The final study cohort was grouped into four race and ethnicity groups: White, Black, Hispanic, and Asian. Study data were obtained via individual chart review of included patients with mortality data supplemented/confirmed by National Death Index search [24]. The study was approved by the Institutional Review Board at Stanford University, Stanford, CA. All authors had access to the study data and reviewed and approved the final manuscript.
Study outcomes and study definitions
The primary study outcomes included the incidence of liver events and overall and non-liver-related mortality. Liver-related outcomes included the development of NAFLD-i (defined as NAFLD with stage 1 fibrosis or higher), cirrhosis, hepatocellular carcinoma (HCC), and/or liver-related deaths, whichever came first. Cirrhosis was defined by liver histology; clinical diagnosis of portal hypertension, platelet <120,000/┬ĄL, history of ascites and/or hepatic encephalopathy; by radiographic findings such as nodular liver contour; or by noninvasive methods (Fibrosure┬«, FIB-4 >3.25, shear wave ultrasound, Fibroscan┬«, or magnetic resonance elastography).
The study observation period began at the time NAFLD was confirmed, and the censor criteria included the development of study outcomes, loss to follow-up, death, or end of the study period, whichever came first.
Statistical analysis
We described and compared continuous variables among the 4 study groups using the analysis of variance test if the variables followed a normal distribution and the KruskalŌĆōWallis test if not. We reported results for continuous variables as mean (┬▒standard deviation) or median and interquartile range. For categorical variables, we reported data as numbers and percentages (%) and used the Žć2 test to compare values among groups.
We used the KaplanŌĆōMeier methods to determine the incidence of liver-related outcomes, overall mortality, and non-liver-related mortality. We used the log-rank test to compare the incidence of events of interest among the study groups.
We used univariable Cox proportional hazards regression to estimate the unadjusted hazard ratio (HR) and identify potential factors (with P<0.10) to include in the multivariable model to estimate adjusted hazard ratios (aHR) for factors associated with the development of liver events, overall or non-liver related mortality. Factors with potential association with outcomes by prior reports were also included in the multivariable models. Statistical significance was defined with a two-tailed P-value <0.05, and all analyses were done using the Stata version 17 (Stata Corporation, College Station, TX, USA).
RESULTS
Patient characteristics
Our study cohort included a total of 9,340 NAFLD patients who met our study criteria. The study patients were divided into four groups: White (4,115 patients, 44.1%), Black (214 patients, 2.3%), Hispanic (2,604 patients, 27.9%), and Asian (2,407 patients, 25.7%) (Table 1). Hispanic patients were the youngest group with a mean age of 44.5 years, about 10 years younger than the White patients (mean age 54.1 years), followed by Asian and Black patients (mean age 48.3 and 51.4 years, respectively) (P<0.0001). The Hispanic group was most likely to be female (63.3%) while the majority of patients in the Asian group were males (55.5%) (P<0.0001). Black patients had the highest body mass index (BMI) and the highest percentage of diabetes mellitus, hypertension, cardiovascular disease, and chronic kidney disease. In fact, the majority of Black patients in the cohort had hypertension (65.9%), close to one-half had diabetes mellitus (42.1%), and about one in three (30.4%) had chronic kidney disease. Patients in the Black group had the lowest aspartate aminotransferase, alanine aminotransferase, and the highest platelet levels compared to other groups, but they had the highest alkaline phosphatase (Table 2). However, we found no significant difference in the total cholesterol, triglycerides, or glucose levels among the four racial and ethnic groups. White patients were most likely to have non-liver cancer (23.0% compared to 13.1ŌĆō14.8% in other groups, P<0.0001). The percentage of cirrhosis was lowest in the Asian group (15.5%), followed by the Hispanic group (17.8%), and highest in the White (21.8%) and Black (23.3%) groups (P<0.0001) (Table 1). Notably, while Black patients made up 2.29% of the total cohort, only 0.67% of the liver biopsies were performed in Black patients as compared to 49.11% among White patients who made up 44.06% of the cohort.
Liver-related outcomes (NAFLD-i, cirrhosis, HCC, and liver-related mortality)
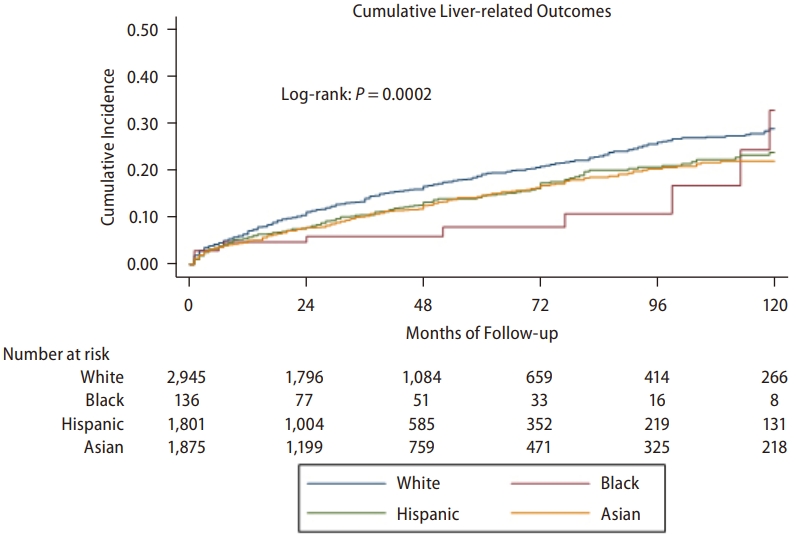
Over a follow-up of 140,167 persons-years for White patients, 5,985 persons-years for Black patients, 76,684 persons-years for Hispanic, and 97,556 persons-years for Asian patients, there were 2,711 liver-related events among White patients, 149 among Black patients, 1,898 among Hispanic patients, and 1,793 among Asian patients. Figure 1 shows that the rate of development of liver-related events differs significantly among the racial and ethnic groups (P=0.0002). The highest cumulative 5-year incidence was observed among White patients (19.1%), the lowest among Black patients (7.9%), and the Asian and Hispanic patients having fairly similar rates (14.6% and 14.5%, respectively). The difference among the White, Hispanic, and Asian groups remained significant even after Black patients, as the group with the lowest rate was excluded (P<0.0001).
On univariable Cox proportional hazard regression, compared to the White group, Black, Hispanic, and Asian groups were all associated with lower risk of NAFLD-i (aHR 0.60 to 0.82), but the association between Black patients and NAFLD-i was not statistically significant (P=0.07) (Table 3). On the multivariable model adjusted for age, sex, race and ethnicity, and diabetes mellitus, compared to White patients, only Asian patients were significantly associated with about 20% lower risk of NAFLD-i (aHR 0.81, 95% confidence interval [CI] 0.70ŌĆō0.95, P=0.008) and cirrhosis (aHR 0.81, 95% CI 0.68ŌĆō0.96, P=0.02). In addition, Hispanic patients had nearly four times greater risk of having liver-related mortality compared to White patients (aHR 3.84, 95% CI 1.63ŌĆō9.04, P=0.002) after adjusting for age, sex, and diabetes mellitus. However, in another multivariable model adjusting for additional comorbidities such as cardiovascular diseases, chronic kidney disease, high BMI, and hyperlipidemia, we found that Black patients were less likely to have NAFLD-i and cirrhosis compared to White patients in this study (Table 3).
Overall and non-liver-related mortality
Among all death events in this study, two most common causes were cardiovascular-related (32.47%) and non-liver cancer-related (36.16%). In contrast to the findings of liver-related outcomes above, we found much higher overall and non-liver-related mortality rates among Black patients as compared to the other three groups (Fig. 2, P=0.0017 and 0.0004, respectively). Over a follow-up of in persons-years of 205,137 for White, 8,054 for Black, 103,652 for Hispanic, and 122,929 for Asian patients, there were 137, 10, 65, and 49 deaths of any cause, respectively. The 5-year and 10-year cumulative overall mortality was highest for Black patients (9.2% and 15.0%, respectively), about 3 times higher than those of the other groups (3.5% and 7.3% for White, 2.6% and 5.6% for Hispanic, and 2.5% and 4.3% for Asian groups). In a sensitivity analysis excluding Black patients as the group with the highest rate, there remained significant differences in both the overall (P=0.031) and non-liver related (P=0.026) mortality among the White, Hispanic, and Asian groups.
We found that the majority of deaths in all racial and ethnic groups to be non-liver related and similar patterns of differences were among the study groups with non-liver related mortality. The numbers of non-liver-related deaths were 127, 10, 52, and 45 for White, Black, Hispanic, and Asian groups, respectively (corresponding follow-up time in persons-years: 205,137; 8,054; 103,653; and 122,929, respectively). The 5-year and 10-year cumulative rates for non-liver mortality were highest at 9.2% and 15.0% for Black, followed by White (3.2% and 6.5%), and lowest for Hispanic (2.0% and 4.0%) and Asian (2.3% and 3.9%) patients.
On multivariable regression analysis (Table 4), compared to White patients, Black patients were at more than two times higher risk of both non-liver related (aHR 2.35, 95% CI 1.22ŌĆō4.51, P=0.010) as well as overall mortality (aHR 2.13, 95% CI 1.11ŌĆō4.08, P=0.022). Hispanic patients also had about 50% higher risk of overall mortality compared to White patients (aHR 1.44, 95% CI 1.05ŌĆō1.99, P=0.022), but there was no statistically significant difference between Hispanic and White patients in regard to non-liver-related mortality risk (aHR 1.23, 95% CI 0.87ŌĆō1.75, P=0.22). Meanwhile, though not statistically significant, there was a trend for also lower risk of overall (aHR 0.70, 95% CI 0.50ŌĆō1.00, P=0.053) and non-liver related (aHR 0.70, 95% CI 0.48ŌĆō1.01, P=0.059) deaths among Asian patients as compared to White patients. In a sensitivity analysis adjusting for other comorbidities such as BMI, diabetes mellitus, cardiovascular diseases, chronic kidney disease, and hyperlipidemia, we found similar trends and direction to the results described above, except the hazard ratio for overall mortality for Black patients no longer reached statistical significance (Table 4).
DISCUSSION
Using clinically based individual longitudinal data, we were able to closely examine the association of race and ethnicity and long-term outcomes among patients with NAFLD in this study. We found that although Black patients made up the smallest group of our overall cohort, they carried a significantly higher comorbidity burden compared to White, Hispanic, and Asian patients. As such, this may explain why they also were at the highest risk for overall and non-liver-related mortality despite having a lower incidence of liver-related outcomes. Black patients with NAFLD incurred a two times higher risk for overall and non-liver-related mortality compared to White patients. Hispanic patients followed a similar pattern as Black patients but were at a lower rate compared to Black patients. Asian patients were at a 19% less risk for liver-related outcomes compared to White patients.
Because Black patients were the smallest group but carried such a high comorbidity burden and had the highest prevalence of cirrhosis, we removed them from our sensitivity analysis to determine the impact of race and ethnicity among White, Hispanic, and Asian groups. We found that White patients retained the highest risk for the cumulative incidence of liver-related outcomes, while Hispanic and Asian patients remained similar. White patients also had the highest cumulative incidence of overall and non-liver-related mortality, followed by Hispanic and then Asian patients.
Our data provides further evidence on the prevalence of NAFLD by race and ethnicity, where Black patients tend to comprise a smaller proportion among those with NAFLD [25]. On the other hand, these data provide additional information on long-term outcomes among persons with NAFLD in the United States, an area that has been under-reported due to the use of cross-sectional data. We found that Black patients with NAFLD carry a substantial risk for overall mortality and non-liver-related mortality outcomes, followed by White, Hispanic, and Asian patients. These findings held true after adjusting for the clinical differences between the groups. These results hold significance for policymakers as although Black individuals may have a lower susceptibility to developing NAFLD with fibrosis, but once present, they are disproportionately affected [2,26]. Therefore, continued actions are needed to prevent the development and progression of NAFLD in Black patients and address barriers to healthcare. Hispanic patients also appear to be affected by various social determinants of health that increase their risk of developing NAFLD, so efforts in determining culturally sensitive and appropriate healthy living interventions are needed in these communities [27-31].
These recommendations take on more significance for Hispanic and Black females as they not only comprised the largest group among Black and Hispanic individuals but results from a recent study found that Hispanic and Black females experienced significant increases in the liver transplant wait-list due to non-alcoholic steatohepatitis (NASH) [32]. In fact, this study reported that NASH was the second leading indication for liver transplantation overall but the number one indication among women, especially in Hispanic and Black females. In addition, a previous study highlighted that Black patients who developed HCC after 2010 had worse survival compared to White patients due to their more advanced stage at presentation, while race and ethnicity was not an independent predictor for mortality, highlighting again the need to improve access to healthcare for Black patients [33]. Most importantly, Black patients were significantly more likely to have comorbidities such as higher BMI, hypertension, diabetes mellitus, hyperlipidemia, and cardiovascular and chronic kidney diseases, which are all well-documented risk factors for worse health outcomes and mortality in this group [34-36]. In fact, 60% of the deaths among Black patients in our study were due to cardiovascular diseases. The causes of these disparities are multifactorial and likely due to social and structural determinants of health, such as structural racism and income inequality, that together limit access to care and early diagnosis, education, and intervention [37,38].
On the other hand, Asian patients were at lower risk for NAFLD-i and cirrhosis compared to White patients and marginally at lower risk for overall and non-liver-related mortality compared to White patients. Such findings are in line with what has been reported in prior studies [19,39,40]. In one specific study conducted among patients with HCC, investigators determined that Asian patients had improved survival compared to White patients. The investigators suggested that their improved survival could be due to genetic differences that altered the detrimental effects of factors associated with severe disease development. Although further research is needed to understand this premise among patients with NAFLD, this reasoning may be plausible as Asian patients in our study also had the lowest prevalence of cirrhosis.
Though our study was conducted retrospectively at a single tertiary care center, the cohort was large and racially and ethnically diverse, with a large proportion of Hispanic and Asian patients, and spanned over 25 years. Patients were followed longitudinally, and the study data reflected a collective experience of more than 400,000 person-years. We minimized the risk of selection bias by selecting the cohort consecutively and included patients from all clinics and diverse clinical settings in our healthcare system and not just gastroenterology or liver clinics. With the recent announcement of the metabolic dysfunction-associated steatotic liver disease (MASLD) nomenclature, which highlights the cardiometabolic factors affecting steatotic liver disease, our studies found consistent results with Black patients who had more metabolic risks at presentations had the highest mortality risk compared to patients in other racial and ethnic groups. This further highlights the multifactorial disease pathophysiology of fatty liver disease and metabolic factors as major contributors to worse outcomes. Even though we used the NAFLD definition in our study, these results are still likely applicable with the new MASLD classification, as a recent study has shown that the discrepancy between NAFLD and MASLD is minimal, and findings from NAFLD studies should still be valid even with the nomenclature change [41].
In this large cohort of patients with NAFLD who were followed longitudinally in a major medical center in Northern California, we were able to determine long-term outcomes, including mortality by race and ethnicity. Although Black patients comprised the smallest proportion of our study cohort, they had the worst mortality outcomes. Black patients were at more than 2 times higher risk for both overall and non-liver-related mortality compared to White patients. Hispanic patients were 1.5 times increased risk for overall mortality compared to White patients, while Asian patients were 19% less likely to develop NAFLD-i and cirrhosis. As our understanding of NAFLD pathophysiology is expanded, our findings extend previous reports that used cross-sectional data and provide further evidence that policymakers need to develop interventions that are culturally appropriate and sensitive to the needs of different communities to help improve success.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





