

INTRODUCTION
Hepatitis B virus (HBV) infection is now the leading cause of chronic hepatitis, cirrhosis and hepatocellular carcinoma (HCC) in the Asian countries.1 Acute self-limiting HBV infection usually has little impact on morbidity, whereas persistent HBV infection is a major public health problem in Korea.2 The natural history of HBV infection varies, according to the age at which the infection was contracted. Perinatal transmission of HBV, particularly mother-to-child transmission of the virus during the perinatal period, is a common source of chronic infection.1
Host genetic factors may significantly influence the ability to clear HBV following infection. In recent years, increasing attention has been drawn to the role of host genetic factors in the natural course of viral hepatitis. Previously, we demonstrated that polymorphisms in TNF-╬▒, IL-10, IFN-╬│ genes were correlated with the susceptibility to chronic HBV infection.3,4 However, the exact role of host genetic factors in the clearance of HBV and the risk of HCC occurrence remain uncertain.
Apolipoprotein (ApoE) is mainly found in the lipoprotein bound form, present in chylomicrons, very low density lipoproteins, and high density lipoproteins, as well as a key regulator of lipid and cholesterol metabolism.5,6 ApoE is a polymorphic protein, which arises from three alleles at a single gene locus. The three major isoforms, apo-╬Ą2, apo-╬Ą3, and apo-╬Ą4, differ from one another by single amino acid substitutions, a change, which has profound functional consequences at both the cellular and molecular levels.7 ApoE has raised particular concern since ApoE polymorphisms are related to several chronic disorders, such as Alzheimer's disease and cardiovascular disease.8,9
ApoE genotype could be an important host genetic factor affecting disease progression in chronic liver disease. ApoE isoform appears to have a hepatitis C virus (HCV)-specific protective effect on liver disease, and the outcome of chronic HCV infection is better among the ╬Ą4 carriers, due to slow fibrosis progression.10,11 Since HBV may use apolipoprotein pathways to recycle and infect hepatocytes, it is possible that apolipoprotein polymorphism may play a role in the natural history of HBV infection. However, evidence regarding the contribution of ApoE genotype to outcome of HBV infection is limited.12
The aims of this study were to assess if ApoE functional polymorphisms determine disease outcome in HBV infected individuals, and to verify the association with the occurrence of HCC in patients with chronic liver diseases of various etiologies.
MATERIALS AND METHODS
Study patients
This study is a retrospective case-control study, in which ApoE genotyping and measuring of serum ApoE were performed on the enrolled subjects who were randomly selected. A total of 156 subjects were enrolled in this study, which included 109 case subjects who were diagnosed with liver cirrhosis (LC) or HCC at Ajou University Hospital, between September 2007 and May 2009. Diagnosis of HCC was based on imaging findings of nodules larger than 1 cm, which showed an intense arterial uptake, followed by a washout of contrast in the venous-delayed phases in 4-phase multi-detector CT scan or dynamic contrast enhanced MRI and/or biopsy. Cirrhosis of the liver, on the other hand, was diagnosed pathologically or based on the clinical evidence of portal hypertension, such as visible collateral vessels on the abdominal wall, esophageal varices on esophagogastroscopy, palpable splenomegaly, and sonographically definite findings of cirrhotic liver or ascites. Samples from 47 healthy volunteer, without history of liver disease, were collected as a control. A total of 156 participants underwent Apo E genotyping and of those, 136 participants (87.1%) underwent serum ApoE measurements. All specimens for this study were provided by the Ajou Human Genome Research & Bio-Resource Center, a member of the National Biobank of Korea, which is supported by the Ministry of Health and Welfare. All samples derived from the National Biobank of Korea were obtained with informed consent under institutional review board-approved protocols.
ApoE genotyping and serum ApoE measurements
ApoE genotyping was performed by extracting DNA from whole blood samples. Genotyping for ApoE polymorphisms was carried out by PCR. Amplification reactions were performed in a thermal cycler (Veriti, Life technologies co., CA, USA), using ApoE genotyping PrimerMix Kit (Genotech co., Daejeon, Korea) as a reaction mix. Each reaction mixture was heated at 94Ōäā for 10 minutes, followed by 30 cycles of amplification (94Ōäā for 45 s, 60Ōäā for 45 s, and 72Ōäā for 45 s). Upon completion of PCR, the products were analyzed by electrophoresis on a 2% ethidium bromide-stained agarose gel.
Of the 156 subjects, serum was available in 136 subjects. Serum ApoE levels were measured in study subjects with the use of an ELISA Kit (ApoE4/Pan-ApoE ELISA Kit; minimum detection limit=4 ng/mL; MLB international co., Woburn, MA, USA) on the absorbance reader (Sunrise, Tecan Group Ltd., M├żnnedorf, Switzerland).
Statistical analysis
All categorical variables are reported as counts and percentages, and comparisons were conducted using a chi-square or Fisher's exact test, as appropriate. Continuous variables are reported as the means┬▒standard deviation with its ranges, and comparisons were conducted using ANOVA with Bonferroni-Dunn test. The homogeneity of variance was tested by Levene's test. Two-sided P values <0.05 were considered statistically significant. All statistical analyses were performed with SPSS software version 16.0.
RESULTS
Patient characteristics
The comparisons of the baseline characteristics, between the three groups who had assessed their ApoE genotypes, are summarized in Table 1. A total of 156 subjects were included (116 men and 40 women), and their ages ranged from 9 to 82 years. The mean age of patients with LC and HCC was higher than that of the healthy controls. The cause of LC and HCC in the enrolled subjects was exclusively HBV infection. Of the 59 HCC patients, 49 patents had liver cirrhosis.
ApoE genotype in case-control population
The ApoE genotype distribution and allele frequencies of the subjects are shown in Table 2. Among the 156 subjects, the most common genotype was ╬Ą3/3, accounting for 69.9%, followed by ╬Ą3/4 and ╬Ą2/3, accounting for 15.6% and 10.1%, respectively. The genotypes of ╬Ą2/4 and ╬Ą4/4 were minor genotypes, which only accounted for 1.3% together. The ╬Ą3 allele was the most common allele, with allele frequencies of 5.8% for ╬Ą2 allele, 84.3% for the ╬Ą3 allele and 9.9 % for ╬Ą4 allele in all participants.
To examine the effect of ApoE genotype on the progression to LC or occurrence of HCC, we analyzed the genotype frequencies among the control, the LC and the HCC subjects. The ApoE genotype was associated with the progression to liver cirrhosis. The odds of developing LC associated, with the carrying of the ╬Ą3/3 genotype, were significantly increased (OR 2.71, CI 1.10-6.21) (Table 2). Compared with the subjects, who were ╬Ą4 carrier, ╬Ą4 non-carrier had an increased susceptibility to LC development (OR 0.26, CI 0.09-0.80). There was no significant difference in the allele frequencies or genotype distribution of ApoE, between liver cirrhosis and HCC patients (Table 2). There is no difference of genotype frequencies according to Child-Pugh score in cirrhotic patients.
Serum ApoE levels in study subjects
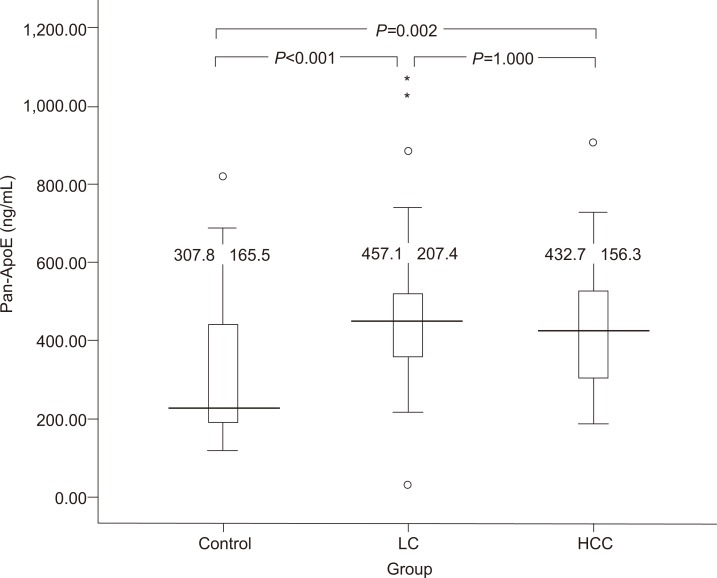
Among to investigate the functional significance at the protein level, we had performed serum ApoE measurements among the 136 individuals in the same set of subjects. The level of serum ApoE was significantly higher in the LC group (P<0.001) and the HCC group (P=0.002) compared with that of the control group (Fig. 1). The mean ApoE level of the LC group tended to be higher than that of the HCC group, but significant differences between the two groups were not observed (Fig. 1).
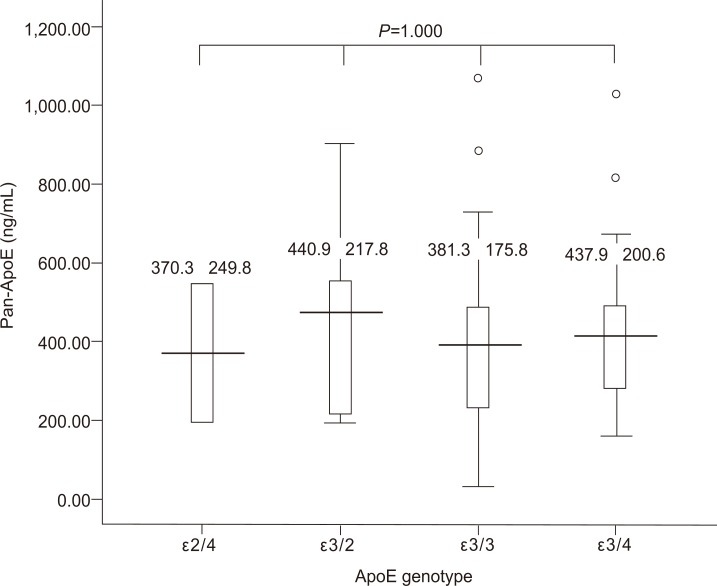
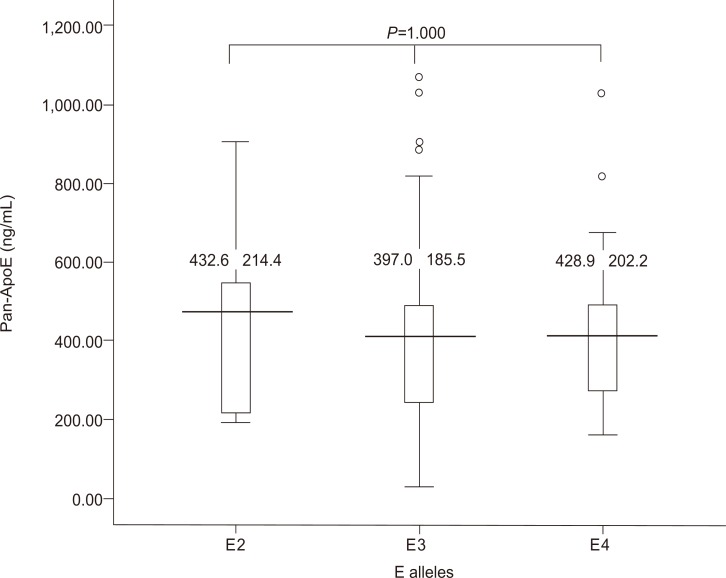
We analyzed whether the serum levels of ApoE correlate with that of ApoE genotypes. Figure 2 demonstrates the serum ApoE levels with regard to ApoE genotype. There was no significant difference in the serum ApoE levels among the different ApoE genotypes. Serum ApoE levels in subjects with different ApoE alleles showed no significant difference (Fig. 3).
DISCUSSION
Increasing evidence indicates that genetic factors influence the natural history of chronic liver disease. In this study, we have determined whether the ApoE genotypes can predict the outcome of HBV infection and the occurrence of HCC originated from various etiologies. The carriers of apoE4 allelic variant had lower probability of disease progression to liver cirrhosis, but the occurrence of HCC was not affected by ApoE genotypes. Although there is insufficient data to show a direct functional effect of ApoE genotype on the progression to liver cirrhosis, our results suggest a possible genetic association between ApoE genotype and viral clearance in HBV infected patients.
In the current study, ApoE3 allele was associated with a higher probability of progression to HBV-related liver cirrhosis, and ApoE4 allele was a protective factor for developing liver cirrhosis. This result is an agreement with previous report, that a strong association was observed between the apoE3/E3 genotype and the occurrence of more severe liver disease.12 Another recent investigation of the influence of ApoE polymorphism and outcome of HCV infection also suggested that the apoE4 allele protected against severe liver diseases.10
The role of ApoE in the pathogenesis and eradication of chronic HCV is becoming clearer. It is well known that HCV is linked to lipoproteins and mainly uses the LDL receptor pathway to colonize liver cells.13,14 A strong interaction has been postulated to exist between ApoE and hepatitis C virus infection.15 Taken together, ApoE4 seems to be protective against CHC infection and retards the progression of fibrosis. In contrast, HBV interacts with ApoH and possibly interacts with other lipoproteins.16,17 By modulating the transport and the entry of HBV into hepatocytes, apolipoproteins may influence the course of infection, although the virological effects of HBV and HCV are different.
Polymorphisms should have a functional significance. It is essential to show that the change in the gene causes a relevant alteration in the function or level of gene product to establish medically useful links between polymorphism and disease.18 In this study, we assessed both the ApoE genotype and the serum ApoE levels in the same set of patients and sought to confirm the relationship between the serum ApoE levels and liver cirrhosis progression in the enrolled subjects. Higher ApoE levels are observed in patients with liver cirrhosis than in the healthy controls. These results suggest that genetic factor and its gene product may affect the natural course of viral infection. It is not clear that allelic polymorphisms, in the ApoE, can affect the capacity to product ApoE. We assessed whether ApoE production varies, according to the genetic composition of the ApoE. According to our results, ApoE production was not affected by ApoE genotype.
The serum ApoE predominantly originates from the liver and the macrophages.19 ApoE has additional roles, as a modulator of the immune function. Proliferation of both CD4 and CD8 lymphocytes is suppressed by ApoE, which reduces the production of biologically active IL-2.20 In addition, ApoE can have a direct effect on tissue macrophage recruitment, independently, of the lipoprotein metabolism.21 Several data on the role of ApoE in the regulation of inflammation were reported. ApoE has been observed to increase in the serum of patients with sepsis.22 Recently, serum proteomic profiling in patients with drug-induced liver injury demonstrated that elevation of the serum ApoE had the diagnostic power for differentiating patients with drug-induced liver injury from that of the controls.23 In our study, patients with liver cirrhosis showed higher ApoE levels than that of the controls. This result suggests that the elevated ApoE levels can be caused by repeated hepatic inflammation seen in patients with liver cirrhosis.
ApoE was up-regulated in the tissue of HCC developed in patients with chronic viral hepatitis C and serum of HCC patients.24,25 The course of HCC development is a multistep process, and cirrhosis has been considered as a precancerous stage. Because only a subset of LC patients develops HCC, it is of great interest to identify factors that affect the transition from LC to cancer. Hence, only patients with cirrhosis were enrolled in our study, however, there were no differences between liver cirrhosis and HCC patients in ApoE genotype and serum ApoE levels.
Our study has some limitations in its study design. First, study subjects did not include the patients with chronic hepatitis or inactive HBV carrier. Thus, this study could not adequately evaluate the effects of the ApoE genotype on the progression of fibrosis. As a consequence, ApoE genotype could, in fact, be associated with an increased susceptibility to the HBV persistence, not to fibrosis progression. It would be more reasonable to select non-cirrhotic chronic liver disease as a control to find factors of disease progression. Second, sample size was small. Prediction of patients who will develop HCC in patients with chronic liver disease is an important unmet clinical need. We were unable to assess this issue clearly in this current study because of the sample size being small. Further investigations with a larger sample size are needed.
In conclusion, the ApoE ╬Ą3/3 genotype frequencies were higher in patients with HBV associated liver cirrhosis rather than controls. The serum ApoE levels are higher in patients with liver cirrhosis compared with that of the healthy individuals. It appears that the usefulness of ApoE genotype as a predictor of viral clearance after HBV infection and diagnostic value of the serum ApoE levels for the diagnosis of liver cirrhosis need to be defined.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




