

INTRODUCTION
Hepatocellular carcinoma may develop from multistep carcinogenesis via dysplastic nodules in the cirrhotic liver. The first stage between high-grade dysplastic nodule to overt hepatocellular carcinoma is vaguely nodular, early hepatocellular carcinoma. The consensus on the nomenclature and pathologic characteristics of both entities were recently established by an international consensus group for hepatocellular neoplasia,1 and were adopted in the recent World Health Organization series of tumor classification.2
We present herein a case of early hepatocellular carcinoma in a 58-year-old man with B-viral macronodular cirrhosis. We discuss the histopathologic features and differential diagnosis from high-grade dysplastic nodule of the liver.
CASE SUMMARY
A 58-year-old male was transferred to our hospital for surgery to remove a recently found liver mass. The liver nodule was found on abdominal ultrasound during a regular checkup. The hepatocellular carcinoma was suspected after subsequent abdominal computed tomography (CT) at a private clinic.
The initial hematologic and blood chemistry data were as follows: white blood cell count, 6,000/┬ĄL; hemoglobin, 14.6 g/dL; platelet count, 81,000/┬ĄL; blood urea nitrogen, 13 mg/dL; creatinine, 0.7 mg/dL; albumin, 3.5 g/dL; aspartate aminotransferase, 44 IU/L; alanine aminotransferase, 32 IU/L; and total bilirubin, 0.8 mg/dL. He was positive for hepatitis B surface antigen (HBsAg) and anti-hepatitis B envelop (HBe), and negative for anti-HBs, HBeAg, and hepatitis C virus. His alpha-fetoprotein and cancer antigen 19-9 levels were elevated, at 20.4 ng/mL and 65.3 U/mL, respectively. He was negative for both protein-induced by vitamin K absence or antagonist II and carcinoembryonic antigen, 21 mAU/mL and 0.6 ng/mL, respectively. The preoperative work-up revealed a slightly enhancing and delayed washout nodule of about 1.1 cm in segment (S) 6 of the liver on liver dynamic magnetic resonance imaging with enhancement. It was not well delineated on T1- or T2-weighted images and exhibited opposing signal intensities on in and out phases. Hepatocellular carcinoma was suspected, and a S6 segmentectomy was performed.
PATHOLOGY FINDINGS
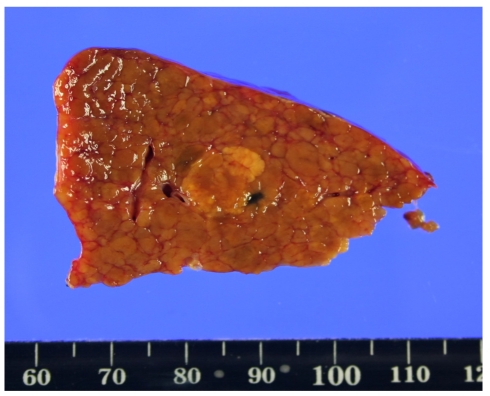
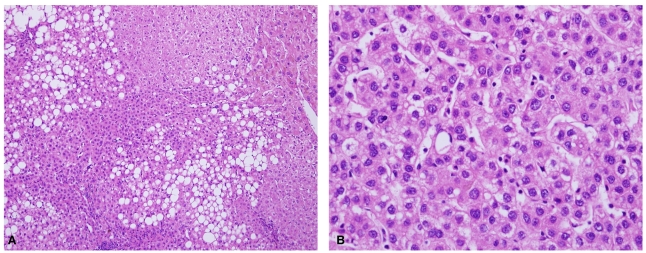
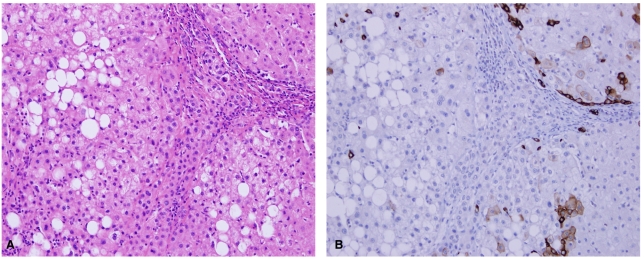
The resected portion of the left liver weighed 82 g and measured 10├Ś6├Ś3.5 cm. Gleason's capsule was smooth and intact. Sectioning revealed an ill-defined, vaguely nodular, and somewhat yellow-brown solid mass measuring 1.2├Ś1.0 cm (Fig. 1). The surrounding liver parenchyma had been replaced by large cirrhotic nodules. Microscopic examination of the nodule disclosed proliferation of well-differentiated hepatocytes in a microtrabecular pattern, accompanied by diffuse macrovesicular fatty metamorphosis (Fig. 2). The hepatic cords were irregular in arrangement, and on average, two cells thick. They spread laterally in a replacing growth pattern without a surrounding tumor capsule or pseudocapsule. Residual portal tracts could be observed within the nodule (Fig. 3A). The nuclear density was variably increased, mostly more than twice that of normal hepatocytes. The cell size was constant, but smaller than usual and with an increased nuclear cytoplasmic ratio, consistent with small-cell change (Fig. 3B). A few foci of stromal invasion were noted within and around the portal tract (Fig. 4A). These findings were highlighted by immunohistochemistry for cytokeratin 7 (Fig. 4B). Sinusoidal capillarization was not evident and was rather focally localized in the periphery of the dysplastic portion. Foci of portal vein invasion was not found.
DISCUSSION
Ultrasound screening allows the early detection of small hepatocytic lesions, and the progress of radiologic techniques has meant that pathologists experience a greater number of smaller lesions in the liver. Any hepatocytic nodules in cirrhotic liver tissue, including large regenerative nodules, low-grade dysplastic nodules, high-grade dysplastic nodules, and small hepatocellular carcinomas, can present similarly. A small hepatocellular carcinoma is defined as being less than 2 cm in diameter, and can be divided into two types: vaguely nodular early hepatocellular carcinoma and distinctly nodular progressed hepatocellular carcinoma. Early hepatocellular carcinoma cannot be easily differentiated from the high-grade dysplastic nodules on either macroscopic or microscopic examination. Although there are some differences in nuclear density (1.3-2 times greater in high-grade dysplastic nodules vs. 2 times greater in hepatocellular carcinoma than in adjacent hepatocytes), the two lesion types share many common features, such as an indistinct margin, no capsule, increased cell density, irregular thin-trabecular pattern, intratumoral portal tracts, pseudoglandular pattern, diffuse fatty change, nodule-in-nodule appearance or subnodules with an increased Ki-67 proliferation index, and varying numbers of unpaired arteries or a varying extent of sinusoidal capillarization.3 Masking of the cytologic atypia of malignant cells by fatty change renders it more difficult to recognize them. The characteristic features of definite malignancy seen in progressed hepatocellular carcinoma, such as portal vein invasion or metastasis, are not usually seen in early hepatocellular carcinoma.3 The only convincing helpful finding of malignancy in early hepatocellular carcinoma is stromal invasion.1-3
Stromal invasion is invasion of tumor cells into the intratumoral portal tracts. The liver is different from other organ sites, which have a well-developed basement membrane structure, and because of this anatomic difference, the foci of destruction of the stromal-parenchymal interface must be recognized by invading growth. The identification of stromal invading foci is not easy and can be frequently missed in needle biopsy of the liver, where the portal tracts might not be included in the small specimen, although it can be assisted by special staining or immunohistochemistry. Victoria blue or reticulin stains help to discriminate the residual portal tracts, while imunohistochemical stains for cytokeratin 7 and 19 can help to determine whether the equivocal lesion of stromal invasion is true tumor cell invasion or ductular reaction of pseudoinvasion around nonmalignant nodules.4
Other biomarkers have been applied to the differential diagnosis of high-grade dysplastic nodule from well-differentiated hepatocellular carcinoma. A panel of triple immunohistochemical markers-glypican-3, heat shock protein 70 (HSP70), and glutamine synthetase (GS)-can increase the sensitivity and specificity to 72% and 100%, respectively, in cases where there is positivity for any two markers.5 However, it is recognized that the interpretation of theses markers should be made with caution, and some helpful tips have been suggested. The characteristic staining pattern of glypican-3 is usually focal cytoplasmic staining; its application as a sole marker of malignancy is thus not recommended, and it should be remembered that it can yield a positive reaction in other lesions and in regenerating hepatocytes. HSP70 can be approved in cases of simultaneous positivity in both the nucleus and cytoplasm, with the internal positive control of hepatobiliary cells of ductular reactions. GS should be accepted in cases of diffuse, intense positivity because of the stepwise increasing pattern from dysplastic nodules through to well-differentiated hepatocellular carcinoma and further to poorly differentiated hepatocellular carcinoma. Another, recently introduced marker, clathrin heavy chain, reportedly exhibits a very promising specificity and positive predictive value.6 However, there is no perfect single marker or panel that allows a confirmative diagnosis of malignancy.
The use of these markers may help to discriminate the equivocal nodule, but may also lead to false confidence, particularly in the case of limited samples, such as those obtained by needle biopsy. Therefore, a final decision of early hepatocellular carcinoma can only be drawn on the basic findings of routine hematoxylin-and-eosin staining, such as abnormal-appearing cytologic and architectural findings, with meticulous effort to find the foci of stromal invasion.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




