


INTRODUCTION
Chronic hepatitis B virus (HBV) infection is the leading cause of liver-related morbidity and mortality, and remains a major threat to global public health, affecting 296 million people worldwide [1]. Antiviral treatment using nucleos(t)ide analogues (NA) effectively inhibits viral replication, ameliorates hepatic necroinflammation, attenuates or reverses liver fibrosis, and reduces the risk of hepatocellular carcinoma (HCC) [2-4]. Current NA regimens include entecavir, tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide (TAF), all of which possess high genetic barriers to the selection of resistance-associated variants and sustained viral suppression can be achieved in the vast majority of treated patients [5]. Nevertheless, NA fails to eradicate HBV because their pharmacological activities are confined to the reverse transcriptase domain of the viral polymerase, without direct effects on the episomal covalently closed circular HBV DNA (cccDNA) and fragments of viral DNA integrated into the host genome, both of which can be transcriptionally active despite NA treatment [6,7]. NA withdrawal almost inevitably reactivates viral replication with potential clinical consequences [8].
The optimal duration of NA treatment for chronic HBV infection has not been clearly defined and recommendations are inconsistent among current guidelines [9-11]. It is generally acceptable to stop NA after seroclearance of hepatitis B surface antigen (HBsAg), or the so-called functional cure, which signifies quiescence of replicational and transcriptional activities of the virus and predicts durable remission off NA treatment [12]. Unfortunately, HBsAg seroclearance rarely occurs during ongoing NA treatment with an annual incidence rate below 1% [13-15]. This treatment endpoint is literally synonymous with indefinite treatment duration for most patients receiving NAs.
Indefinite NA treatment may have several theoretical disadvantages, including the challenge of maintaining medication adherence over an extended period [16], the concern of long-term toxicity from prolonged drug exposure [17], and the financial burden of sustained prescription costs [18]. More importantly, it was found that the incidence of HBsAg seroclearance was paradoxically higher after NA discontinuation compared to during treatment [14,19], and a finite NA strategy of ŌĆ£stop to cureŌĆØ was thus proposed [20,21]. The practice of stopping NA therapy without the requirement of HBsAg seroclearance is currently debatable with both perceived pros and cons (Table 1). For patients who have initiated NA therapy with positive hepatitis B e antigen (HBeAg), current guidelines generally agree treatment cessation may be considered after achieving HBeAg seroconversion, followed by consolidation for one year or longer [9-11]. Contrary to HBsAg seroclearance, however, HBeAg seroconversion does not consistently predict sustained remission after NA cessation, even with additional consolidation for several more years [22,23]. The practice of finite NA therapy in patients with HBeAg-negative hepatitis B is highly debated with conflicting recommendations found in international and local guidelines (Table 2) [9-11,24-30]. Such contradictory recommendations highlight the limitations of current knowledge on this issue. Central to the controversy is the concern about patient safety and most concerning is the risk of acute-on-chronic liver failure (ACLF), which is potentially fatal [31].
Amid interests in and disputes over the finite approach of NA treatment for chronic HBV infection, there is a growing body of evidence reporting clinical outcomes following NA withdrawal [32]. Knowledge about the safety of treatment cessation is indispensable to inform the practice of finite NA therapy, and data have been emerging to quantify the risk of severe withdrawal hepatitis flares and to identify the associated risk factors [33-35]. In this review with a special focus on patient safety, we summarized the data available to date and discussed the selection of patients suitable/unsuitable for NA cessation, patterns of off-therapy flares with implications for patient monitoring, and pragmatic considerations for the timing to resume antiviral therapy. We also stressed current knowledge gaps, pointed out pitfalls in existing literature, and provided our perspectives on future directions of research.
RISK OF SERIOUS ACUTE EVENTS ACCORDING TO CURRENT STOPPING RULES
Incidence of acute hepatitis flares following NA withdrawal
The risk of acute flare-up, a unique feature of chronic HBV infection that can abruptly develop without preceding symptoms and rapidly progress to liver failure within weeks [36,37], must be factored in the consideration of finite NA therapy. It is not surprising to observe acute hepatitis flares following NA withdrawal, because the sudden increase of viral replication along with surge in viremia is known to trigger host immunity against HBV [38], as seen in the setting of immunosuppressive treatment without antiviral prophylaxis [39,40].
The incidence and ŌĆ£natural historyŌĆØ of HBV flares induced by NA withdrawal can be discerned in recent studies from Taiwan, where the reimbursement coverage for anti-HBV therapy is finite (usually three years of treatment) in principle, and patients need to withhold retreatment according to the strict criteria for treatment eligibility [34]. In a large hospitalbased cohort study that applied the Asian Pacific Association for the Study of the Liver (APASL) criteria to select and monitor patients, Liu and colleagues found that acute flares (defined by elevation of serum alanine aminotransferase (ALT) Ōēź5 times the upper limit of normal [ULN]) occurred in 516 out of 1,234 patients (41.8%) within two years after treatment cessation, and reported that the corresponding cumulative incidence reached 42% [35]. In a population-based study with a less selected patient population to represent real-world practice in Taiwan, Hsu and colleagues estimated the cumulative incidence of acute flares (ALT >200 U/L) was 30.7% (95% confidence internal [CI], 29.4ŌĆō32.0%) at four years [41].
Risk estimation for severe withdrawal flares with hepatic decompensation
Most but not all of the withdrawal flares can wane spontaneously or subside with NA retreatment. A severe episode may either present with or progress to ACLF that, in turn, could lead to mortality or the need of liver transplantation. Quantifying the risk of such a severe episode is hence important, but was found to be difficult in earlier studies with small samples and/or few events [42]. This crucial gap in knowledge has recently been addressed by large cohort studies with more than 500 participants and also by pooled analyses of individual studies (Table 3) [33-35,43-46]. In the Taiwanese population-based study by Hsu and colleagues, the cumulative incidence of severe flares with hepatic decompensation (defined by both hyperbilirubinemia and coagulopathy) was estimated at 1.8% (95% CI, 1.5ŌĆō2.2%) at four years after treatment withdrawal [41]. After pooling fifteen studies with 4,525 individual patients in a systematic review and meta-analysis of current literature updated to August 2022, Tseng and colleagues reported that 1.2% (95% CI, 0.70ŌĆō2.1%) of patients would develop severe flares or hepatic decompensation (variably defined in respective studies) after stopping NA. The international RETRACT-B consortium also found that the cumulative incidence of hepatic decompensation (defined as hyperbilirubinemia, coagulopathy, or clinical complications) was 1.8% at five years [33].
On the basis of these aforementioned studies, life-threatening flares were expected to occur in approximately 1ŌĆō2% of HBV-infected patients who discontinued NA according to the stopping rules of earlier practice guidelines (mainly APASL) or local reimbursement policies. Notably, while the criteria of the APASL guidelines are the most stringent for treatment initiation [9-11], they are comparatively more liberal than those of the European Association for the Study of the Liver (EASL) and American Association for the Study of the Liver (AASLD) guidelines for stopping NA therapy (Table 2).
Identification of vulnerable patients at excessive risk
Not all patients carry the same risk of withdrawal flares, and those at excessive risk of serious clinical outcomes should be advised against treatment cessation. It stands to reason that older patients and individuals with far advanced diseases are more vulnerable to devastating flares and this reasoning is now supported by empirical evidence. In a hospital-based study that followed the APASL guidelines to stop NA therapy, Jeng and colleagues [14] found all seven patients who developed hepatic decompensation, and three patients who subsequently died, had liver cirrhosis. In larger studies that were statistically powered to explore risk predictors, liver cirrhosis was consistently identified as a risk factor significantly and strongly associated with serious clinical events following NA withdrawal [35,41]. It has also been shown that an older age was associated with excessive risk of severe withdrawal flares; more specifically, the risk significantly increased with age when the patients were 50 years or older [41]. A higher risk was also observed in patients with a past history of hepatic decompensation or severe acute exacerbation [41,47].
SELECTION OF CANDIDATES FOR FINITE NA THERAPY
High retreatment rates without accurate patient selection
In addition to vulnerable patients at excessive risk of serious flares, individuals who are prone to relapses of clinical hepatitis and unlikely to clear HBsAg following treatment cessation are not suitable to practice finite NA therapy. Stopping NA in these patients bound to resume treatment only brings about unnecessary and potentially harmful interruption in viral inhibition and possible worsening of liver fibrosis. In fact, about half of the patients who stopped NA according to the rules recommended by earlier guidelines developed active hepatitis that fulfilled the usual criteria for antiviral therapy [35,41,48,49]. Such high retreatment rates reflect the insufficiency of current stopping rules to select candidates for finite NA therapy. On one hand, reactivation of viral replication following NA cessation often induces host immune responses that may facilitate seroclearance of HBsAg [50,51]. On the other hand, the elicited immune reaction could also result in severe necroinflammation with serious clinical consequences. It is currently unclear how this double-edged sword can be used to clear HBsAg without causing collateral damage [52]. Notably, patients who developed clinical relapse (usually defined as serum ALT >2├ŚULNs in addition to HBV viremia >2,000 IU/mL) did not have a higher incidence of HBsAg seroclearance than those who remained clinically uneventful [14]. Therefore, the practice of finite NA therapy requires prediction tools that can precisely identify patients at a lowest risk of clinical relapse and also a highest chance of HBsAg loss [53].
Risk predictors-HBsAg
A number of risk predictors, which can be grouped into virus, treatment, and host factors, have been reported to help distinguish patients at different risks of clinical relapse off NA therapy (Fig. 1). Serum level of HBsAg at the end of therapy (EOT) is the most extensively studied and widely validated among them. It is useful to predict both the risk of hepatitis relapse and opportunity of HBsAg loss. In general, the lower the level of EOT HBsAg, the less risk of clinical relapse, and the higher chance of HBsAg seroclearance [54-57]. A cutoff point set at 100 IU/mL was proposed and later validated as the easily applicable threshold to select patients who may consider treatment cessation [57,58]. It should be noted, however, that the risk of clinical flares is lower but not negligible with an EOT HBsAg level <100 IU/mL. The risk can be further decreased by lowering the threshold, but clinical relapse may still occur with a EOT HBsAg level <40 IU/mL, as demonstrated in the study by Tseng and colleagues [59]. Moreover, emerging data indicated that the EOT level of HBsAg did not predict severity of clinical relapse. Fatal flares could still occur in patients with a serum level of EOT HBsAg <10 IU/mL [35].
Risk predictors-HBcrAg
Quantitation of hepatitis B core-related antigen (HBcrAg) in serum can be used to gauge transcriptional activity of the virus and may add to the accuracy of risk prediction based on HBsAg at EOT [60,61]. Hsu and colleagues demonstrated that both EOT levels of HBsAg and HBcrAg were both independent risk factors associated with clinical relapse off NA therapy although these two biomarkers were positively correlated with each other [62]. Nevertheless, how to apply HBcrAg on top of HBsAg in the process of decision making to select candidates for NA cessation remains to be defined. In patients with a low EOT HBsAg (e.g., below 100 or 200 IU/mL), the level of HBcrAg at EOT was found unable to further stratify their relapse risks [59,63,64]. On the other hand, encouraging results were reported in studies that simultaneously combined the two biomarkers together instead of placing one after the other in successive steps [45,62,65,66].
Risk predictors-other viral factors
Other HBV biomarkers that have been reported to predict responses off NA therapy include serum viral load and HBeAg status at treatment initiation [67,68], titer of serum HBV RNA at EOT [64], HBV genotypes [55,59,69], and diversity of viral quasispecies [70]. A lower serum HBV DNA (e.g., <200,000 IU/mL) and negative HBeAg status at the start of antiviral therapy were associated with a lower risk of off-NA relapse [67,68]. In patients with a low EOT HBsAg (e.g., <200 IU/mL), detectable HBV RNA in serum were found to foretell a higher rate of virological relapse [64]. In addition, HBV genotype C versus genotype B was linked to a greater chance of HBsAg loss in Asian patients although the association with off-NA relapse was inconsistent across studies [55,59,69]. A higher pretreatment HBV quasispecies diversity was also found to predict sustained virological response (HBV DNA <2,000 IU/mL) for more than one year off therapy [70].
Risk predictors-host factors
Host factors that are reportedly associated with relapse or remission off NA include age, genetic polymorphisms, ethnicity, circulatory biomarkers of inflammation or immunity, and HBV-specific immune response. As seen in the association with serious life-threatening flares, an older age has been shown to be a significant risk factor for relapses of clinical hepatitis overall [54,55,68]. A pilot study by Su and colleagues [71] found that polymorphisms of CTLA4 and HLA-DPA1, both of which were genes involved in regulation of immune reactions, were predictive of off-NA relapse and clinical response, respectively. There were also preliminary data suggesting that circulatory biomarkers of immunity, such as titers of hepatitis B core antibody (anti-HBc) [72,73] and RNA levels of IFN╬│, IL-8, FASLG, and CCL4 genes from peripheral blood mononuclear cells [74], could help identify patients who would suffer relapses off NA treatment. In fact, a biomarker of hepatic necroinflammation readily available in routine clinical care, i.e., the serum level of ALT, may also add to the risk prediction of off NA relapse [54]. The chance of HBsAg seroclearance was also significantly higher in Caucasian patients than in Asian patients although the incidence of ALT flares did not appear to differ by ethnicity [33,48,75]. This association might reflect differences in the geographic distribution of HBV genotypes, because the genotype was predominantly A or D in Caucasians, but B or C in Asians [75,76]. The mode of transmission, the age/duration of infection, or host genetic polymorphism should also be considered. Further research is warranted.
Risk predictors-HBV-specific immune response
Adaptive immune responses are essential in clearing or controlling HBV infection, and also crucial in mediating liver injury that drives disease progression in patients with CHB [77-79]. The importance of HBV-specific immune response in the prediction of off-NA outcomes has recently been demonstrated. Rivino et al. [80] reported that presence of HBV core and polymerase-specific T cells during NA therapy was associated with absence of flares off treatment. Comparably, increased frequency of functional HBV-specific CD8+ T cells at treatment withdrawal was associated with HBsAg loss or viral control in the study by Garc├Ła-L├│pez et al. [81] Rinker and colleagues also showed that the exhaustion of T cells, which is characteristic of CHB [82], was less severe in patients who cleared HBsAg after stopping NA [51].
Nevertheless, whether NA withdrawal may enhance HBV-specific T-cell immune response is unclear in view of limited and conflicting data [51,81]. Moreover, the probability of functional HBV-specific CD8+ T cell response on NA treatment was found to be significantly correlated with the duration of treatment and EOT HBsAg, both of which were also significant factors associated with off-NA outcomes [83]. Therefore, more research is needed to clarify how HBV-specific immune responses may be factored into the consideration of NA withdrawal.
Risk predictors-treatment-related factors
Treatment-related factors that may impact the risk of off NA relapses include the duration of treatment and the regimen that is discontinued. Earlier studies have shown that a short duration (<6 months) of on-therapy HBV DNA undetectability is predictive of off-therapy relapse [84]. A large body of evidence corroborates an important role for the duration of treatment consolidation, which is defined by the period following HBeAg seroconversion in HBeAg-positive patients, or that after serum HBV DNA becomes undetectable in patients with HBeAg-negative hepatitis B, to determine the risk of off-NA relapse [85-87]. In general, a minimum of one year is required for NA consolidation and extension for two or three years may be preferred [85-87]. Whether further extension beyond three years confers additional benefits to protect against off-therapy relapses has not been confirmed by empirical evidence. Moreover, the types of NA therapy can impact the relapse patterns. Off-treatment relapse occurred significantly more slowly and less frequently with ETV as compared with other regimens including TDF [68,71,86,88,89].
Risk scores
With a few risk predictors uncovered and none sufficiently accurate by themselves, it follows that several independent risk factors may be considered together to improve the precision of risk stratification. The Japan Society of Hepatology (JSH) is the first to endorse application of a scoring formula to select candidates for treatment cessation (Table 2). The JSH score was based on serum levels of HBsAg (<80 IU/mL, 80ŌĆō800 IU/mL, and Ōēź800 IU/mL scored 0, 1, and 2 points, respectively) and HBcrAg (<3 log IU/mL, 3ŌĆō4 log IU/mL, and Ōēź4 log IU/mL scored 0, 1, and 2 points, respectively) at EOT [90]. A total score of 3 or 4 points indicated a high risk of relapse and argued against cessation. Regrettably, external validation of the JSH score has been limited.
The SCAEL-B score is another attempt to integrate information collected at EOT to stratify the risk of clinical relapse [62]. The scoring formula: 35*HBsAg (log IU/mL)+20*HBcrAg (log U/mL)+2*age (year)+ALT (U/L)+40 for tenofovir use (as compared with ETV) consisted of five variables that were conveniently applicable in daily practice. A total score Ōēź320 points indicates a high risk of relapse and low chance of HBsAg seroclearance, while a score <260 points predicts the opposite. The SCALE-B score outperformed the JSH score in the development study and has been independently examined in different patient cohorts with conformed validity in most, albeit not all, of the studies (Table 4) [45,65,66,91]. Nevertheless, it has not been validated in a prospective setting so far, nor has it been calibrated, and appeared insufficient to predict HBsAg seroclearance.
PATIENT MONITORING AFTER TREATMENT CESSATION
Time patterns of off-therapy flares according to NA agents
Close monitoring after treatment is essential to detect HBV reactivation early and effectively manage acute flares, which can insidiously develop but rapidly deteriorate. How close the monitoring should be, however, is unknown [92]. To date, no monitoring program has been prospectively validated to guarantee patient safety. There is only anecdotal and indirect evidence to support current recommendations for posttreatment monitoring.
Generally speaking, NA withdrawal may quickly reactivate HBV replication and usually result in virological relapses within three months after treatment cessation. This timing of off-therapy relapses applies to most NA agents other than ETV [67,68,71,88,89]. For TAF, data is currently limited but it appeared similar to TDF in a pilot study [93]. Therefore, a monthly checkup of serum HBV DNA and ALT is advisable during the first three months. If viremia substantially rebounds and/or ALT flares take place, the management should be individualized with no scheme that can fit all. In principle, subsequent monitoring should be more intense (e.g., every one to two weeks) especially when retreatment was withheld. For patients who do not discontinue ETV and do not encounter virological and/or clinical relapses in the first three months, the follow-up intensity might be decreased to every two to three months through the first year off treatment [92].
ETV is unique for a late timing of off-treatment relapses [67,71], of which the mechanism remains enigmatic. It is common for ETV stoppers to run into virological or clinical relapses after the first three months [8]. Therefore, the monitoring intensity for ETV stoppers may be increased to monthly or bimonthly from the first three months onward until at least one year after treatment cessation.
Although the majority of relapses take place within one year following NA withdrawal, they can still occur years afterwards [34,35]. As a matter of fact, it is possible for patients to suffer HBV reactivation with resultant acute hepatitis flares as long as the viral replication remains active. Disease awareness cannot be overemphasized for NA stoppers, particular those patients with positive indicators for a vigorous viral activity, such as substantial HBV viremia >2,000 IU/mL or high titers of HBsAg >1,000 IU/mL. Patients should be educated to recognize symptoms and signs suggestive of acute flares and instructed to seek medical attention as soon as possible whenever they notice or suspect the manifestations of hepatic insufficiency. Besides the due concern over acute flares and resultant complications, attention should be paid as well to more stealthy progression of the disease, such as worsening of liver fibrosis and development of HCC.
Dynamic risk prediction in the follow-up of NA stoppers
Posttreatment monitoring can be opportunely informed by changes in time-varying factors that foretell an upcoming bout of acute HBV flare-up. Exploration of dynamic risk predictors for posttreatment monitoring, however, has attracted far less research effort as compared to static factors at treatment initiation or EOT. Although empirical data are relatively sparse, it is conceivable that serum levels of viral DNA and HBsAg, the two convenient biomarkers that have been useful in many aspects of clinical care of HBV infection, can also be used in this application. Serum HBV DNA measured at one month after NA cessation was found to disclose early signals of imminent relapses [71]. The investigators found that one log higher in serum HBV DNA was independent of age, biological sex, NA regimen, and EOT HBsAg level to confer a 50% (hazard ratio [HR], 1.5; 95% CI, 1.1ŌĆō2.0) increase in the risk of forthcoming clinical relapse. A similar finding was reported in a recent study, which found a significant association between serum HBV DNA at week 6 off-therapy and ALT flares (ALT >5├Ś ULN) with a HR of 1.2 (95% CI, 1.0ŌĆō1.8). HBV viremia >10,000 IU/mL at week 6 was estimated to confer roughly a 3.5-fold higher risk of withdrawal flares (HR, 3.4; 95% CI, 1.4ŌĆō8.4) [94]. In addition to the viral load measured at fixed time points, that of virological relapse was found to predict subsequent clinical relapse and also severe flares which required retreatment. It was shown that 89.7% (95% CI, 72.4ŌĆō98.2%) of the patients with a viral load >100,000 IU/mL at the virological relapse developed clinical relapse, and 88.0% (95% CI, 68.7ŌĆō97.9%) of them would need to resume treatment in two years [95].
How fast serum HBV DNA rises may also affect the risk of off-therapy flares. A recent retrospective study reported that a much steeper HBV DNA upsurge was associated with the risk of severe flares although the association appeared to interact with the NA regimen [96].
Serum level of HBsAg may markedly change following NA withdrawal in contrast to the typically unfluctuating state during continuous treatment. The time-varying HBsAg level in posttreatment follow-up can be useful to stratify the risk of subsequent relapses. Chien and colleagues [97] confirmed that the dynamic levels of serum HBsAg was associated with forthcoming virological and clinical relapses in a prospective cohort study with serum HBsAg measured every three months after treatment cessation. They reported that the risk of subsequent clinical relapse was very low (only one in nineteen patients) with a HBsAg level below 10 IU/mL.
CONSIDERATIONS OF THE CRITERIA TO RESTART ANTIVIRAL THERAPY
Dilemma over the timing of treatment resumption
It is currently unknown and highly contentious when to resume antiviral treatment in NA stoppers who wish to give finite therapy a try. On one hand, retreatment cannot be withheld until the manifestations of jaundice or coagulopathy, let alone full-blown complications of ACLF. When acute HBV flare manifests with hepatic decompensation, it is not always rescuable by antiviral treatment and may necessitate a timely liver transplant to save lives. Even if the episode is not fatal on the spot, it may leave consequences in the long run as substantial hepatic necrosis is known to accelerate liver fibrosis toward cirrhosis with an increased risk of HCC [98]. Therefore, immediately restarting antiviral therapy for withdrawal flares with the manifestations of liver insufficiency is certainly indicated, but is already too late to ensure patient safety.
On the other hand, recurrent viremia of itself is not an ideal indication for treatment resumption, because it is nearly universal following NA cessation. If patients want to restart treatment due to reappearance of HBV DNA in serum, they should not have interrupted the therapy in the first place. Nevertheless, it is debatable whether retreatment is indicated for recurrence of viremia with serum HBV DNA rising to a certain level with clinical implications. For instance, a viral load >2,000 IU/mL can be considered to be clinically significant and may arguably indicate antiviral therapy [99-101]. Regrettably, virological relapse is still very common in patients who stop treatment as per the criteria of current guidelines although it is not inevitable for carefully selected candidates, such as those with a low HBsAg and/or HBcrAg at EOT [8,54,64]. If virological relapse is fiercer with a higher viral load (e.g., >100,000 IU/mL or higher), patients may consider restarting antiviral therapy, whether or not the episode is accompanied by substantial elevation of serum ALT. Withholding retreatment may not be necessary, because a fierce rebound of viremia often forecasts clinical flares that eventually require antiviral therapy [94-96].
Elevation of serum ALT as the major indication for retreatment
Rise of serum ALT may constitute the indication for retreatment following NA cessation. Various criteria have been proposed in different institutions and studies (Table 5) [34,64,102-108]. Modest elevation of serum ALT (generally 1ŌĆō5├ŚULN) in the absence of hepatic insufficiency was usually managed with close monitoring and retreatment was withheld for a certain period of time (generally one to three months). It has long been observed that serum ALT frequently fluctuated after NA withdrawal, but often could subside without retreatment [19].
Another major reason to withhold retreatment is the belief that restarting antiviral therapy may lower the chance of HBsAg seroclearance. The incidence of HBsAg seroclearance was shown to be significantly higher in patients who experienced clinical relapse and remained untreated than in those clinical relapsers who were retreated [67]. While this observation may encourage NA stoppers who are eager to clear HBsAg not to restart therapy as soon as facing mild fluctuations in serum ALT, it warrants noticing that the timing of retreatment was not randomly assigned in any study conducted to date. Whether the association is causal or confounded remains unclear, particularly when the status of exposure (i.e., clinical relapse or not, retreatment or not) is determined by events that occur after the inception of observation. Moreover, it is not clear how late is too late to avert deterioration to hepatic decompensation. Therefore, patients should not be discouraged from resuming treatment for clinical relapse, which actually meets the usual indication for treatment initiation [9-11]. For sufficiently informed patients who wish to watch and wait, intensive follow-up (every one to two weeks) is strongly advised.
In our opinion, a significant increase in serum ALT (e.g., >10 times ULN) requires immediate retreatment to reduce the risk of further progression, as acute HBV flares cannot always be predictable and the harm of delaying treatment has been well documented [109,110]. On the assumption that treating ŌĆ£goodŌĆØ flares would hinder HBsAg seroclearance, some experts have suggested withholding treatment for withdrawal flares and using the kinetics of serum HBsAg and ALT levels to guide retreatment [111,112]. However, data on the HBV-specific T cell immune response to support the practice of withholding treatment for ŌĆ£goodŌĆØ withdrawal flares is not available. In fact, existing data indicating an increase in HBV-specific adaptive immune response was not associated with withdrawal flares [80,81]. The speculation that retreatment would hinder immune reactions was based on anecdotal evidence from observational research [14,112]. Moreover, how reliably HBsAg and ALT kinetics can distinguish ŌĆ£goodŌĆØ from ŌĆ£badŌĆØ flares has not been prospectively attested. For the benefit of patient safety, we maintain that any proposed rule for withholding treatment in the event of acute HBV flares should be thoroughly scrutinized and validated in prospective studies before being adopted in clinical practice. After all, the consequence of an inaccurate prediction can be irreversible.
LIMITATIONS IN CURRENT KNOWLEDGE AND PERSPECTIVES FOR FUTURE RESEARCH
Interpretation of current literature to evaluate safety of NA cessation requires great caution. First of all, safety outcomes were not adequately reported and could be severely underestimated in existing studies [42]. Serious adverse events were often not specified as a study endpoint and might not have been mentioned at all. In those studies that included severe hepatitis flares or hepatic decompensation, one third (14 out of 46 reports) did not clearly define the safety events [43]. In fact, most of the previous studies focused on virological or clinical relapse and the observation could have been censored before occurrence of a more serious event [32,42]. Accordingly, we believe it is mandatory to include safety events as one of the study endpoints in every research that reports patient outcomes following NA cessation. Such events should be prespecified with a clear definition to allow for validation of the research, comparison among studies, and pooled analysis of relevant data. In addition, much of the available data originates from select specialist centers and ethnic groups and may not be representative of the entire population with CHB, especially those patients who receive care at primary care settings.
Moreover, existing studies were mostly retrospective and highly heterogeneous in various aspects, including compositions of patient populations, eligibility criteria for NA cessation, posttreatment monitoring, indications for retreatment, and measurements of outcomes [32,43,87]. For instance, the proportion of patients with cirrhosis and the criteria for retreatment varied greatly among studies. Without great caution, knowledge synthesis from the literature could be inaccurate and study findings would be erroneously extrapolated to patients who were not represented in the study [42,113]. In particular, there was a substantial heterogeneity in definitions. What defined a ŌĆ£severeŌĆØ flare differed across studies. It could be a marked elevation of serum ALT alone, ALT elevation accompanied with jaundice, ALT elevation with both jaundice and coagulopathy, or overt complications of ACLF. Different definitions certainly lead to different estimates of a ŌĆ£nominally sameŌĆØ event [114]. In order to avoid confusion and thus facilitate advancement of the knowledge, we advocate for an international consensus among leading groups or experts in the field to unify the definitions that are crucial in the studies of NA cessation.
Existing evidence so far has not confirmed the superiority of finite NA therapy over continuous treatment in improving patient outcomes. There should be tangible benefits with measurable effects to justify the risk of potential consequences following HBV reactivation in patients who electively stop the medication. Ideally, the safety, efficacy, and effect size (if effective) of a treatment strategy as compared to the standard of care needs to be evaluated by data from randomized controlled trials that are statistically powered with a representative patient population. Regrettably, evaluation of finite NA therapy is currently based predominantly on observational studies, in which the decision to stop or continue NA treatment was easily confounded. Only three randomized trials were reported to date and one of them has not been fully published. Notably, the results were inconsistent for the effect on HBsAg seroclearance (Table 6) [102-104]. Further evidence from robust randomized controlled trials is required for this treatment strategy to be considered standard care [115,116]. After all, what was approved by regulatory agencies to treat HBV was administration of NA instead of withdrawal from it [117]. Certainly, such a trial must be carefully planned and meticulously executed with patient safety considered as first priority.
Despite recent progress, current knowledge is insufficient for an accurate prediction of clinical outcomes in most NA stoppers. Many of the reported risk predictors have not been externally validated by data from independent study populations and thus, their generalizability is uncertain. How to accurately predict the consequences of ALT flares is particularly crucial but largely unknown. In view of the potential rapidity from ALT elevation to hepatic insufficiency [117], the risk of ACLF cannot be negligible unless ŌĆ£goodŌĆØ and ŌĆ£badŌĆØ flares can be reliably predicted before the flares. Elevation of serum ALT is already a sign of liver injury. The development of biomarkers to forecast outcomes of HBV reactivation requires deeper understanding of immune responses and resultant tissue injuries that underlie different clinical phenotypes [79]. Regrettably, data about HBV-specific immune responses to NA withdrawal are very limited to date. Inclusion of immunological factors into the prediction models, which currently are based on viral antigens [27,62,75], could further improve the predictive accuracy. To this end, we believe dynamic monitoring of both viral factors (activities of replication and/or transcription) and host factors (especially adaptive immune responses) during posttreatment follow-up could be helpful and worthy of study.
CONCLUSIONS
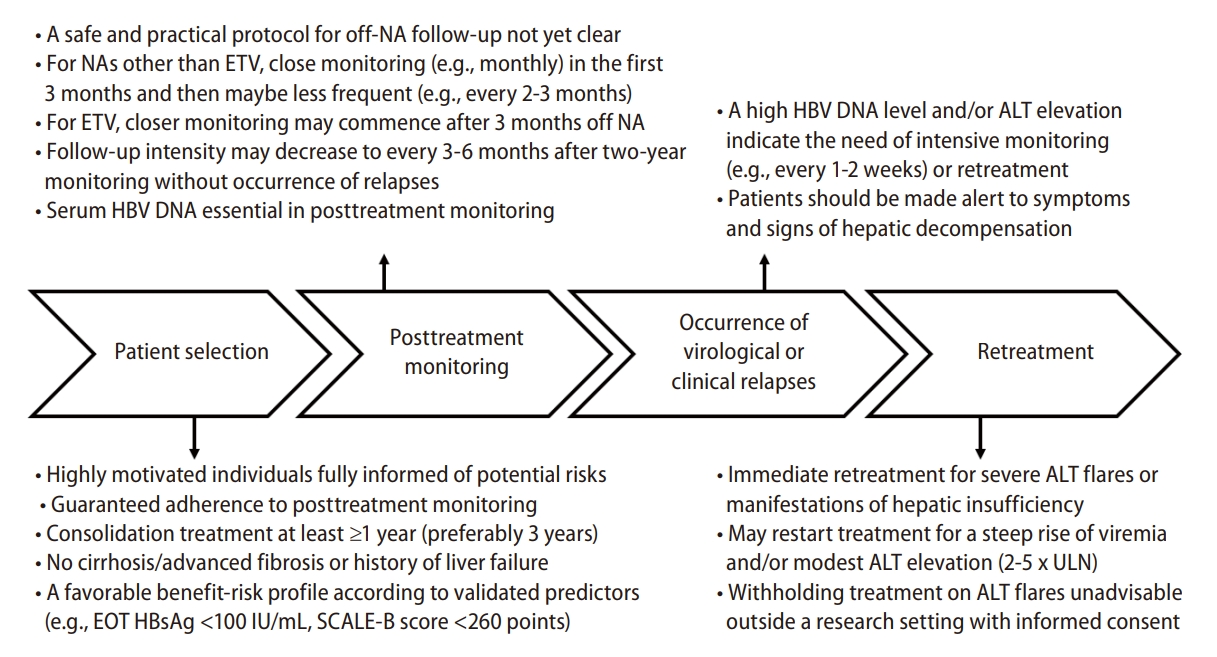
Discontinuation of NA therapy leads to HBV reactivation in most of the patients who discontinued NA per the criteria recommended in guidelines. Virological and clinical relapses were common, but seroclearance of HBsAg only occurred in a minority of patients. Moreover, approximately 1% of the NA stoppers suffered severe withdrawal flares with hepatic decompensation. Accurate risk prediction is essential to identify the candidate who can safely stop NA. A useful tool is likely to include viral, host, and therapeutic factors. Close follow-up after NA cessation is mandatory, but how close the monitoring should be is not yet clear. A posttreatment surge in serum HBV DNA with a high-level viremia forecasts clinical events and may be considered an indication to restart antiviral therapy. Withholding retreatment on ALT flares cannot be recommended as a routine practice, because rapid deterioration is not always predictable and potentially devastating. In the interest of patient safety, elective discontinuation of NA therapy can only be considered in carefully selected, highly motivated, and fully informed individuals who consent to the uncertainties during posttreatment monitoring (Fig. 2).

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





