


Graphical Abstract
INTRODUCTION
Hepatitis C virus (HCV) infection is a major public health concern, because it frequently leads to liver cirrhosis (LC) and hepatocellular carcinoma (HCC), which impose significant burdens on many countries [1]. HCV treatment has changed from interferon-based therapies to direct-acting antivirals (DAAs), with significant improvements in sustained virological response (SVR) rates [2]. Achieving SVR through anti-HCV therapy greatly reduces the risk of HCC, liver failure [3], and liver-related mortality [4].
The risk of HCC can be reduced but cannot be eliminated completely, even after successful antiviral therapy [5], particularly among patients with persistent advanced fibrosis, insulin resistance, and diabetes mellitus (DM), as well as among the elderly [6-8]. Moreover, patients in whom antiviral therapy fails are still at a high risk of developing HCC, especially those with advanced fibrosis and DM [9].
Chronic hepatitis C (CHC) has been associated with an increased risk of DM [10], and the comorbidity of DM increases the risk of developing HCC in patients with CHC [11]. Metformin use has been associated with a reduced risk of HCC compared with other oral hypoglycemic agents (OHAs) or insulin among patients with DM [12]. We previously showed that metformin use in DM significantly reduces the risk of HCC in patients with CHC after successful antiviral therapy [13].
Statin use has been associated with reduced development of cirrhosis and incidence of HCC, which is mainly observed in patients receiving lipophilic statins [14]. Although the chemopreventive effects of metformin in patients with DM and statins in patients with hyperlipidemia (HLP) reduce the risk of HCC in patients with CHC, which has been proven after achieving SVR [13], the impact on HCC risk reduction remains unclear in patients with CHC who have failed antiviral therapy.
The current study aimed to assess the impact of metformin for DM and/or statins for HLP on the risk of HCC among CHC patients in who failed antiviral therapy. The findings of this study will improve our understanding of the potential benefits of chemoprevention in reducing the risk of HCC in patients with difficult-to-cure CHC.
The study was approved by the institutional review boards of Kaohsiung Medical University Hospital (KMUHIRB-E(I)-20210378) and was conducted in accordance with the Declaration of Helsinki and the ethical guidelines. All participants provided written informed consent.
MATERIALS AND METHODS
Study population
The study included patients aged ≥20 years who were diagnosed with CHC either through liver histology or by testing positive for anti-HCV or HCV RNA for > six months. These patients were drawn from a large-scale, multicenter cohort in Taiwan (Taiwanese Chronic Hepatitis C Cohort, T-COACH) and had undergone antiviral interferon-based therapy for at least four weeks since 2003.
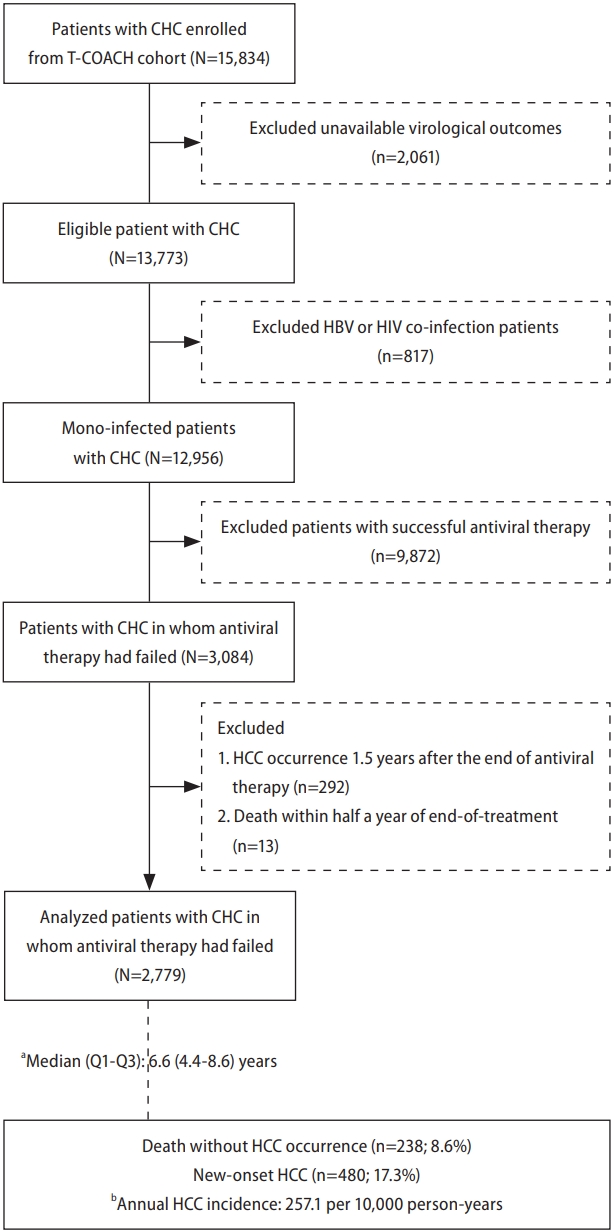
We excluded patients who lacked virological outcome data, achieved SVR, had coinfection with human immunodeficiency virus or hepatitis B virus (HBV), died within six months of end-of-treatment (EOT), and developed HCC within 1.5 years after EOT. Finally, the analysis focused on 2,779 patients with CHC who experienced antiviral therapy failure (Fig. 1).
Independent variables
Data collected on the independent variables included: 1) demographic characteristics: age, sex, and body mass index (BMI); 2) medical history: DM, HLP, and hypertension (HTN); 3) laboratory data: AST, ALT, platelet count, creatinine, liver fibrosis (FIB-4 score; fibrosis index based on four factors), renal function (estimated glomerular filtration rate, eGFR); and 4) clinical features: renal function impairment (eGFR ≤60), advanced fibrosis (FIB-4 ≥3.25), LC, and sustained virological response (SVR; HCV RNA seronegativity 24 weeks after interferon-based therapy). Related assessments of the liver and renal function were performed accordingly. The FIB-4 score was calculated using age, AST, ALT, and platelet count of the patient: [age (years)×AST(IU/L)]/[platelet (x1,000/μL)×ALT (IU/L)^0.5]. The eGFR was calculated using the patient’s creatinine levels, age, and sex: 186×creatinine (mg/dL)-1.154×age (year)-0.203×0.742 (if female). LC was based on any of the following: liver histology,15 transient elastography (FibroScan®; Echosens, Paris, France) >12 kPa,16 acoustic radiation force impulse >1.98 m/s17, FIB-4 >6.5,18 or the presence of clinical, radiological, endoscopic, or laboratory evidence of cirrhosis and portal hypertension.
Study endpoints and linked databases
The data for the study were obtained from the National Health Insurance Research Database, which covers approximately 26 million Taiwanese people since 1995.
Participants were considered to have DM if they met any of the following criteria: a history of DM on treatment with OHAs with or without insulin, fasting glucose ≥126 mg/dL, or 2-hour plasma glucose ≥200 mg/dL. Patients with a DM diagnosis who had taken metformin for ≥84 days were considered metformin users, whereas those who had taken metformin for <84 days were considered metformin nonusers after six months of EOT. Participants were considered to have HLP if they had a history of HLP and used medication. Diagnosed HLP statin users were defined as patients with an HLP diagnosis who had taken statins for ≥84 days, whereas those who had taken statins for <84 days were considered HLP statin non-users after six months of EOT.
All diseases, including HCC and liver transplant (LT), were identified using specific codes from the International Classification of Diseases, 9th or 10th revision (ICD-9-CM and ICD-10). In this study, the occurrence of HCC was determined based on data from the Cancer Registry, whereas the LT cases were identified from the registry of catastrophic illnesses. Information on patient deaths was obtained from the death registry. The relevant medication codes for the diseases were linked to the corresponding entries in the detailed health insurance inpatient/outpatient records (Supplementary Table 1).
New-onset HCC was defined as HCC occurring in patients 1.5 years after antiviral EOT. The follow-up period began 1.5 years after antiviral EOT and continued until the censored events (HCC and death/LT) or December 31, 2019.
Statistical analysis
Continuous variables are presented as mean ± standard deviation, while categorical variables are expressed as numbers (percentages). Chi-square was used to compare subgroups with categorical parameters, and Student’s t-test was used for continuous parameters, as appropriate.
Person-years were calculated as the number of years that each participant contributed to the study from 1.5 years after EOT to the date of the first diagnosis of HCC, death/LT, or December 31, 2019, whichever occurred first. The annual incidence of HCC was calculated as the number of new-onset HCC cases divided by the sum of person-years and the groups were compared by Poisson method.
The study considered death or LT as competing events, meaning that patients who died or underwent LT before developing HCC were no longer at risk of developing HCC. To account for this, the study modified the Kaplan-Meier method using Gray’s cumulative incidence method [19]. Cox proportional hazard regression was used to calculate sub-distribution hazard ratios (SHRs) [20] for HCC development before and after adjusting for various factors such as age, sex, LC, HCV genotype (GT), HCV RNA and aspirin use. In addition, we compared the cumulative incidence of new-onset HCC between subgroups by stratifying the patients according to their LC status.
Sensitivity analyses were conducted to ensure robustness of the findings. First, advanced fibrosis was substituted with LC to validate the robustness of the results in the multivariate analysis. Second, in this study, participants were defined as metformin users when they used metformin six months after EOT. Patients who used metformin either before or during antiviral therapy were classified as metformin non-users. To strengthen our findings, we reclassified previous metformin users to confirm the effect of metformin on the risk of new-onset HCC in patients with DM. A similar approach was employed for HLP statin users. Third, to avoid potential bias related to specific clinical scenarios including treatment by DAA for IFN-failed patients or patients with diabetes and severe renal impairment (eGFR <30) who are typically not candidates for metformin therapy, we conducted further analysis to validate our findings. All statistical analyses were performed using SAS Enterprise Guide, and P-values less than 0.05 were considered statistically significant.
RESULTS
Patient characteristics
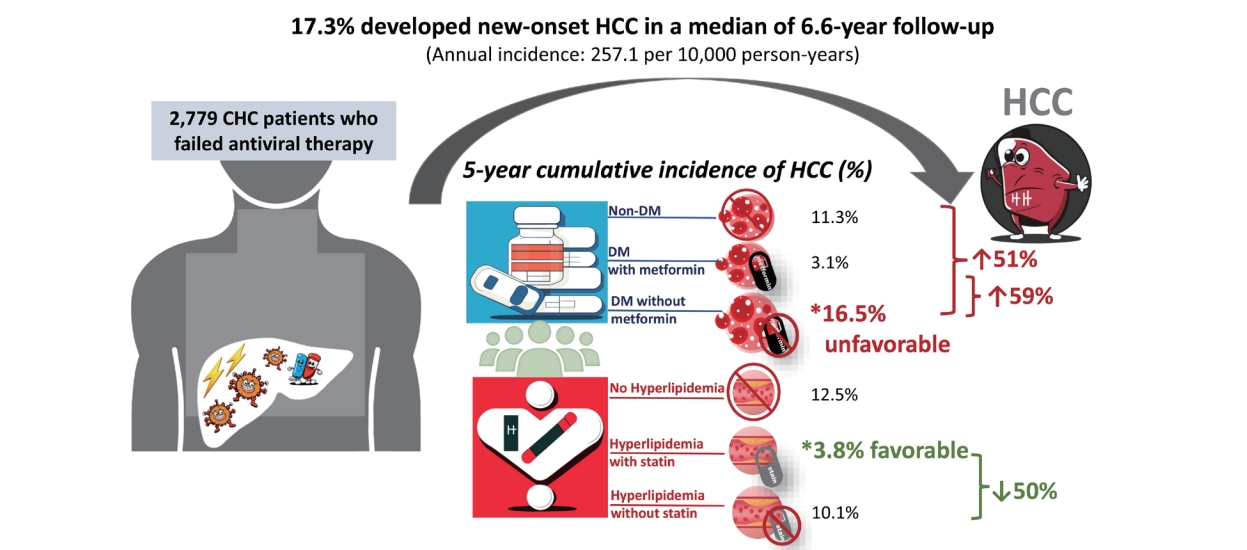
The clinical characteristics of the 2,779 CHC patients who failed antiviral therapy are presented in Table 1. The mean age of the patients was 56.1±10.7 years, mean log-transformed HCV RNA levels were 6.1±0.9, 52.7% were female, 34.7% had advanced fibrosis (FIB-4 ≥3.25), 16.2% had liver cirrhosis, 6.7% had an eGFR <60 mL/min/1.73m2, and 63.1% were infected with HCV GT1. Furthermore, 17.6% of the patients were obese (BMI ≥27), 22.3% had DM, 11.3% had HTN, and 21.8% had HLP. Among the patients with DM, 53.5% were metformin users. Among patients with HLP, 82.5% were statin users. In addition, 10.4% of the patients were aspirin users. Overall, 238 (8.6%) patients died before the development of HCC and 480 (17.3%) developed new-onset HCC during a total of 18,668 person-years of follow-up (median: 6.6 years). The annual incidence of HCC was 257.1 cases per 10,000 person-years (Table 1).
HCC risk between patients with/without DM and on/not on metformin
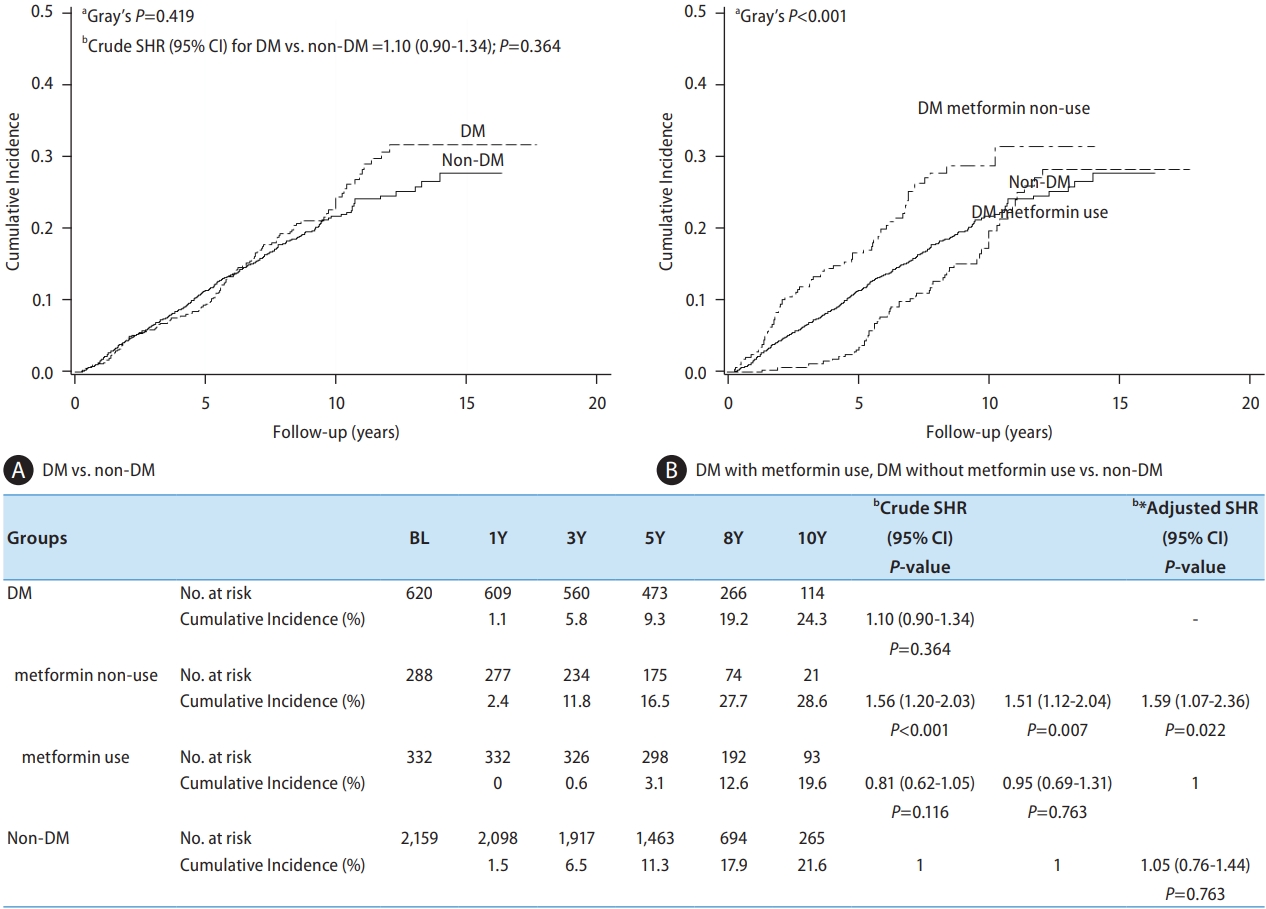
Of the 2,779 CHC patients in whom antiviral therapy failed, 620 (22.3%) had DM. After a median follow-up of 7.27 years, 65 died before HCC developed, and 125 developed HCC (annual incidence: 277.1 per 10,000 person-years). For the other 2,159 (77.7%) patients without DM, 173 died before HCC developed, and 355 developed HCC (annual incidence: 250.8 per 10,000 person-years) after a median follow-up of 6.56 years. The 5-year cumulative incidence rate of HCC was not significantly different between patients with and without DM (9.3% vs. 11.3%, Gray’s P=0.419) (Fig. 2A). Notably, patients with DM who were not on metformin showed a significant increase in the risk of HCC compared to metformin users (annual incidence: 408.9 per 10,000 person-years in metformin non-users vs. 200.1 per 10,000 person-years in metformin users, P<0.001, Table 1). The 5- and 10-year cumulative incidence rates of HCC were 11.3% and 21.6%, respectively, in non-DM patients; 3.1% and 19.6%, respectively, in DM metformin users; and 16.5% and 28.6%, respectively, in DM metformin non-users. HCC risk was significantly higher in metformin non-users than in metformin users (adjusted sub-distribution hazard ratio (aSHR=1.59, 95% CI=1.07–2.36, P=0.022) and in patients without DM (aSHR=1.51, 95% CI=1.12–2.04, P=0.007). However, there was no difference in HCC risk between metformin users and patients without DM (aSHR=1.05, 95% CI=0.76–1.44, P=0.763) (Fig. 2).
HCC risk between patients with/without HLP and on/not on statins
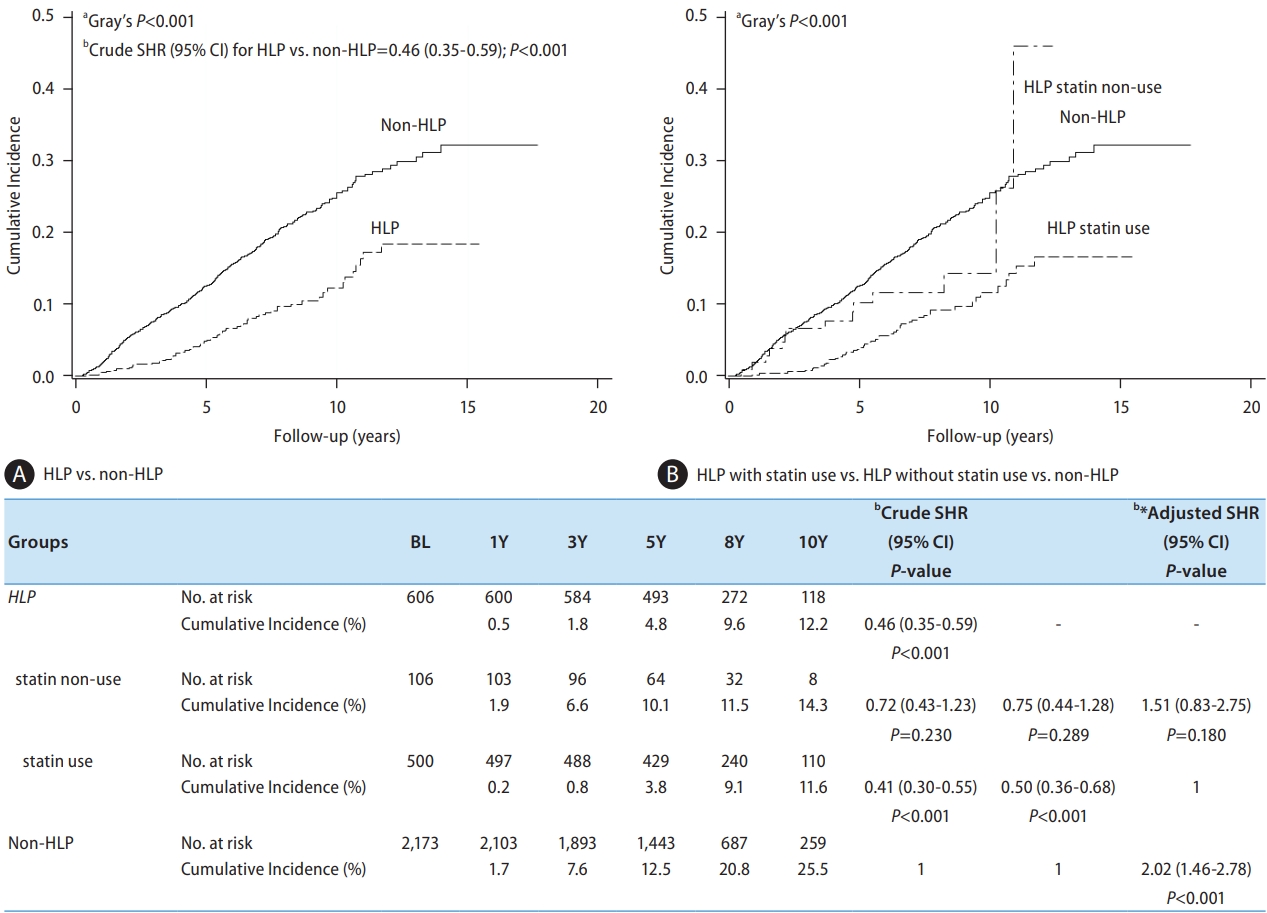
Of 606 patients with HLP, 31 died before HCC developed, and 61 developed HCC after a median follow-up of 7.64 years (annual incidence: 131.8 per 10,000 person-years). Of the 2,173 patients without HLP, 207 died before HCC developed, and 419 developed HCC (annual incidence: 298.4 per 10,000 person-years) after a median follow-up of 6.46 years. The 5-year cumulative incidence rate of HCC was significantly lower in patients with HLP than in those without HLP (4.8% vs. 12.5%, Gray’s P<0.001). After further stratification by statin use in HLP patients, the annual incidences were 220.8 per 10,000 person-years in statin non-users vs. 117.7 per 10,000 person-years in statin users (P=0.036, Table 1). The 5-year cumulative incidence rates of HCC were 12.5%, 3.8%, and 10.1% in patients without HLP, HLP statin users, and HLP statin non-users, respectively. The HCC risk was significantly lower in HLP statin users than in patients without HLP (3.8% vs. 12.5%; aSHR=0.50, 95% CI=0.36–0.68, P<0.001), but there was no difference between patients with HLP who were statin non-users and those who did not (Fig. 3).
Factors associated with HCC risk
After accounting for death as a competing risk, univariate Cox regression analysis showed that being elderly (≥65 years), female, having DM without metformin use, HCV GT1, high AST, high ALT, advanced fibrosis and LC were independently associated with a higher risk of HCC, while aspirin use, HLP statin use and low HCV viral load were associated with a significantly lower risk of HCC. In multivariate analysis, the significant factors associated with increased HCC risk were LC (aSHR=2.27, 95% CI=1.81–2.85), elderly (≥65 years; aSHR=1.89, 95% CI=1.52–2.36), HCV GT1 (aSHR=1.30, 95% CI=1.04–1.63) and DM without metformin use (vs. no DM; aSHR=1.51, 95% CI=1.12–2.04). Conversely, patients with HLP who were on statins had a significantly lower risk of HCC than those without HLP (aSHR=0.50, 95% CI=0.36–0.68) (Table 2). Aspirin use also exhibited a significantly lower HCC risk than non-aspirin use (aSHR=0.71, 95% CI=0.51–1.00, P=0.049) (Supplementary Fig. 1A).
Subgroup analysis
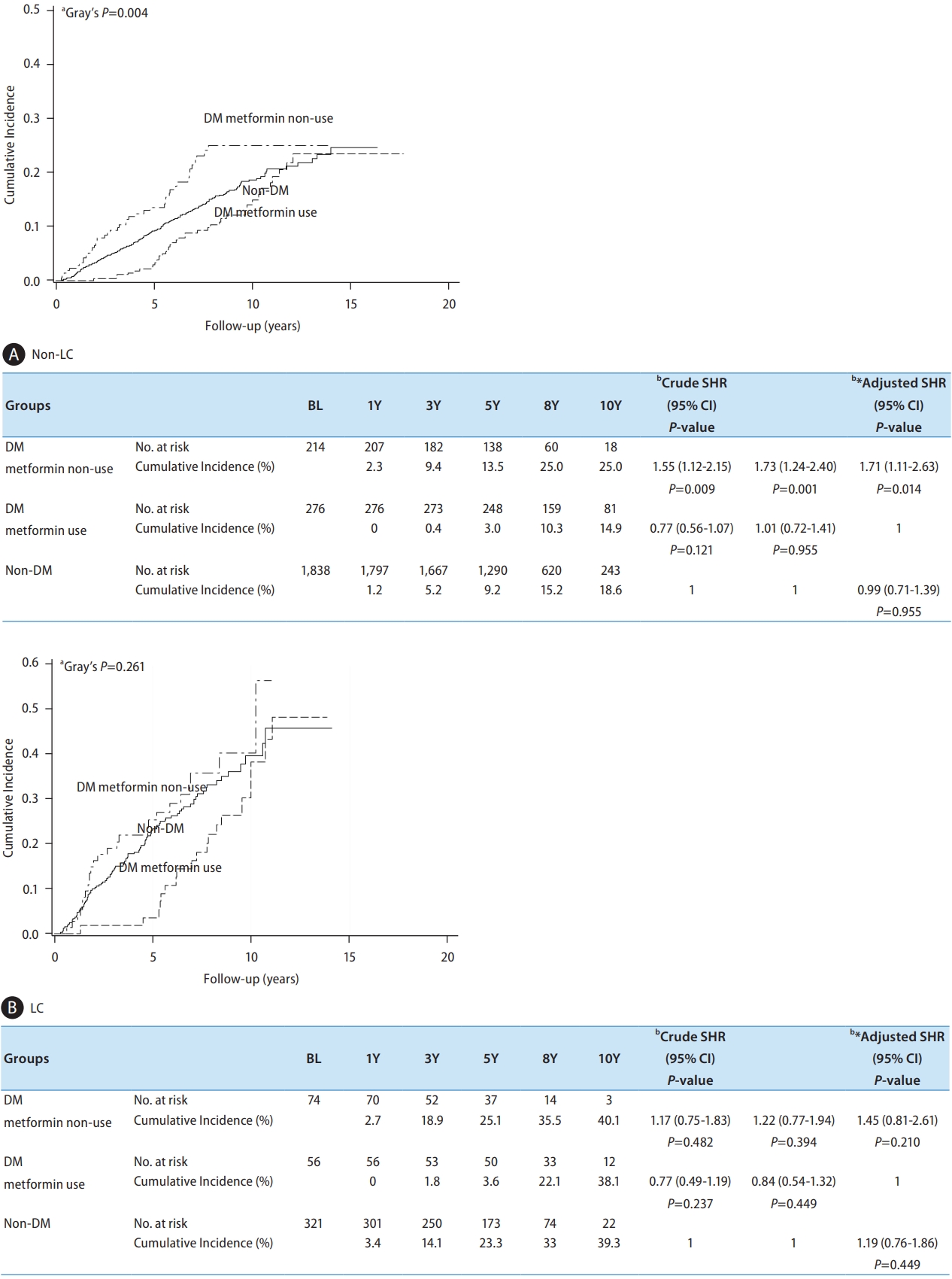
LC is the most significant risk factor for HCC. Therefore, we stratified the patients according to their cirrhosis status to evaluate the impact of metformin or statin use among different subgroups.
Among patients without LC, the 5-year cumulative incidence rates of HCC were 9.2%, 3.0%, and 13.5% among those without DM, metformin users, and metformin nonusers, respectively. The HCC risk was significantly higher in DM metformin non-users than in patients without DM, with an aSHR of 1.73 (95% CI=1.24–2.40, P=0.001) and in patients with DM on metformin, with an aSHR of 1.71 (95% CI=1.11–2.63, P=0.014) (Fig. 4A). No significant differences were observed between metformin users and patients without DM. Among patients with LC, the 5-year cumulative incidence of HCC was 23.3%, 3.6%, and 25.1% in patients without DM, metformin users, and metformin non-users, respectively. However, the difference in HCC risk between metformin non-users and the other two groups was not significant (Fig. 4B).
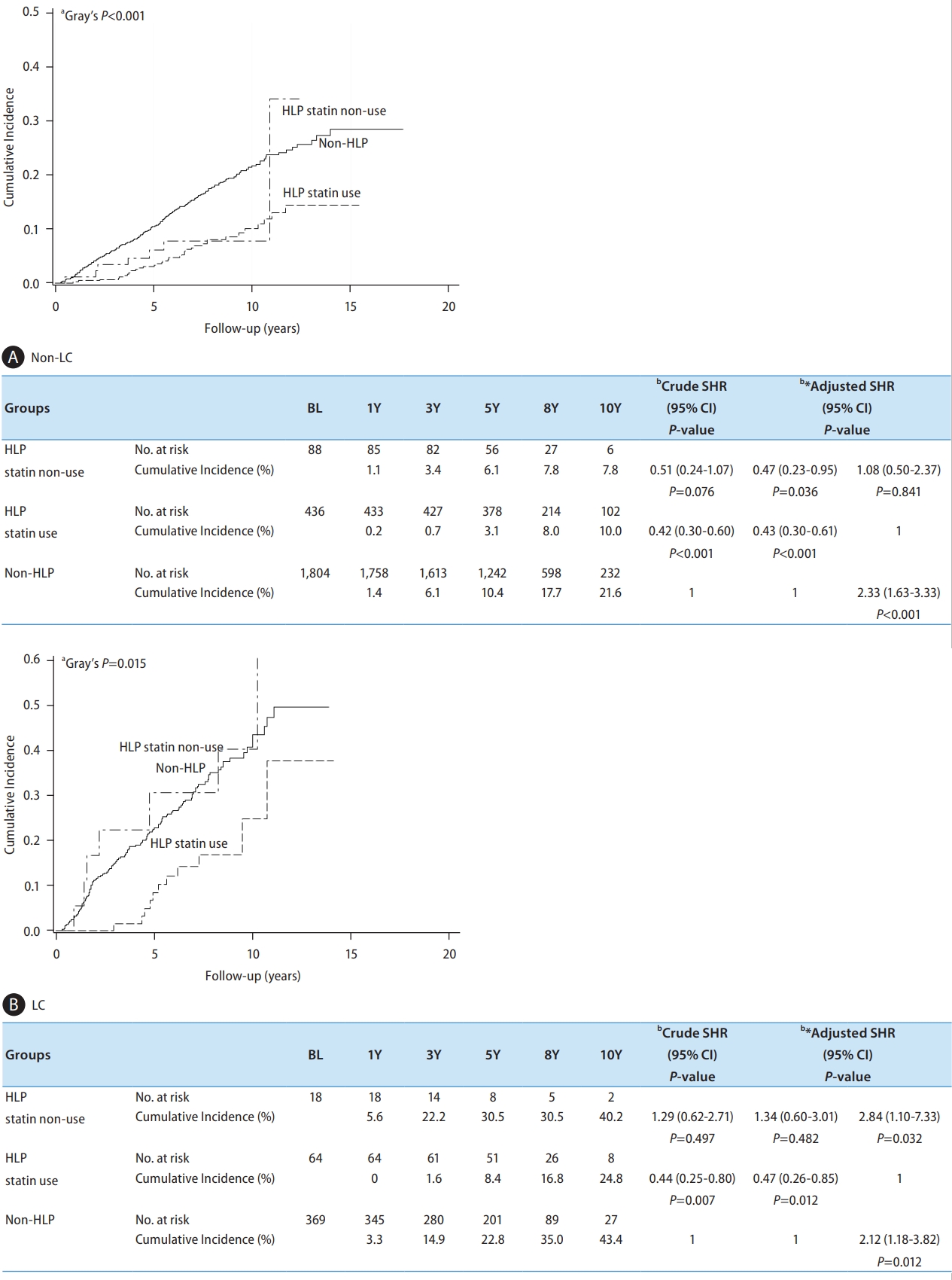
Among patients without LC, the 5-year cumulative incidence rates of HCC were 10.4%, 3.1%, and 6.1% in patients without HLP, in HLP statin users, and in HLP statin non-users, respectively. The HCC risk was significantly lower in HLP statin users than in patients without HLP, with an aSHR of 0.43 (95% CI=0.30–0.61, P<0.001), while there was no difference in HCC risk between HLP statin users and HLP statin non-users (Fig. 5A). Among patients with LC, the 5-year cumulative incidence of HCC was 22.8%, 8.4%, and 30.5% in patients without HLP, HLP statin users, and HLP statin non-users, respectively. HCC incidence was significantly lower in HLP statin users than in patients without HLP (aSHR=0.47, 95% CI=0.26–0.85, P=0.012) and HLP statin non-users (aSHR=0.35, 95% CI=0.14–0.91, P=0.032), whereas there was no difference in HCC risk between patients without HLP and HLP statin non-users (Fig. 5B).
The aspirin use was not associated with a lower risk of HCC in the subgroup of non-LC (aSHR=0.76, 95% CI=0.53–1.08, P=0.122, Supplementary Fig. 1B) and LC (aSHR=0.68, 95% CI=0.39–1.18, P=0.167, Supplementary Fig. 1C).
Sensitivity analysis
Four sensitivity analyses were conducted to validate the robustness of the main findings and enhance the results.
Assessment of outcomes with metformin or statin use before or after the end-of-antiviral therapy
To avoid underestimating the duration of metformin or statin use, we redefined metformin or statin use, either before or after EOT. The 5-year cumulative incidence rate of HCC was higher in patients taking metformin before or after EOT, with rates of 11.1%, 8.1%, and 29.7% in patients without DM, metformin users, and metformin non-users, respectively. HCC risk remained significantly higher in DM metformin non-users than in DM metformin users (aSHR=2.28, 95% CI=1.48–3.46, P<0.001) or patients without DM (aSHR=2.45, 95% CI=1.95–4.24, P<0.001) (Supplementary Fig. 2A). The 5-year cumulative incidence of HCC was higher in patients with HLP on statins before or after EOT, with rates of 12.7%, 5.1%, and 12.7% in patients without HLP, HLP statin users, and HLP statin non-users, respectively. HCC risk remained significantly lower in HLP statin users than in patients without HLP (aSHR=0.43, 95% CI=0.34–0.63, P<0.001) (Supplementary Fig. 2B). The results were consistent between groups using different definitions of metformin or statin use.
Outcomes using advanced fibrosis as the critical variable
We used another level of liver fibrosis, advanced fibrosis (FIB-4 score >3.25), to validate our findings. In multivariate analysis, HCC risk was significantly higher in patients with advanced fibrosis than in those without advanced fibrosis (aSHR=3.01, 95% CI=2.45–3.64, P<0.001, see Supplementary Table 2). The predicted model showed that DM metformin non-users continued to have a significantly higher risk of HCC compared to patients without DM (aSHR=1.54, 95% CI=1.16–2.03, P=0.005) and DM metformin users (aSHR=1.60, 95% CI=1.13–2.85, P=0.013). The HCC risk was significantly lower in patients with HLP on statins than in patients without HLP (aSHR=0.47, 95% CI=0.34–0.67, P<0.001). The results of LC and advanced fibrosis models were consistent.
Minimize potential bias related to specific clinical conditions
To avoid potential bias related to specific clinical scenarios including treatment by DAAs for IFN-failed patients or patients with diabetes and severe renal impairment (eGFR <30) who are typically not candidates for metformin therapy, we conducted further analysis to validate our findings.
After excluding 78 IFN-failed patients who experienced retreatment with DAAs, we found that diabetic patients not treated with metformin had a 1.50-fold increased risk of developing HCC compared to non-diabetic individuals (aSHR=1.50, 95% CI=1.13–1.98, P=0.005) (Supplementary Fig. 3A). Conversely, hyperlipidemia patients who were prescribed statins showed a 55% decrease in HCC risk compared to those without hyperlipidemia (aSHR=0.45, 95% CI=0.33–0.60, P<0.001) (Supplementary Fig. 3B).
Similarly, after removing 49 patients with eGFR<30, the risk of HCC in diabetic patients not treated with metformin was found to be 1.56-fold higher than that in non-diabetics (aSHR=1.56, 95% CI=1.18–2.07, P=0.002, Supplementary Fig. 4A). Hyperlipidemia patients on statin therapy had a 55% decreased risk of HCC compared to those without hyperlipidemia (aSHR=0.45, 95% CI=0.33–0.60, P<0.001, Supplementary Fig. 4B).
Taken together, our findings from the current study were consistent across these sensitivity analyses.
Interaction of statin and metformin
In this study, statin non-users had a 2.42-fold higher risk of HCC compared to statin users among metformin non-users, and a 2.23-fold higher risk among metformin users. Whereas, there was no significant difference in HCC risk between metformin non-users and metformin users, both among statin non-users and statin users. Consequently, our analysis did not reveal a significant interaction between statins and metformin in predicting HCC risk (P=0.82, Supplementary Fig. 5).
DISCUSSION
Of the 2,779 CHC patients, 480 (17.3%) developed new-onset HCC and 238 (8.6%) died after antiviral therapy. Patients with DM but no metformin use had a 1.51-fold higher risk of HCC than patients without DM, whereas HCC risk was comparable between patients without DM and those with DM on metformin. The 5-year cumulative HCC incidence (16.5%) was significantly higher in metformin nonusers than in those without DM (11.3%, P=0.007) and metformin users (3.1%, P=0.022). Conversely, patients with HLP who used statins had a 50% lower risk of HCC than those without HLP (5-year cumulative HCC incidence: 3.8% vs. 12.5%, P<0.001). Notably, the unfavorable effect of metformin non-use on increased HCC risk was mainly observed among patients without LC but not among patients with LC. In contrast, a favorable effect of statins on reducing the risk of HCC was observed in patients with and without LC.
HCV infection has been linked to lower lipid profiles, and when a patient with CHC achieves SVR, their lipid profiles may worsen, potentially leading to cardiocerebral events [21-23]. For patients with CHC, DM or HLP, treatment with the antidiabetic agent metformin and cholesterol-lowering statin is commonly used. Several studies have investigated the association between statin use and HCC risk in patients with CHC. Statins are well-known for their preventive role in many cancers, including liver cancer [24,25]. A meta-analysis of 27 studies found strong evidence of statin-related potential in reducing the risk of HCC [24]. Among patients with CHC, statin use has been associated with improved virological response rates to antiviral therapy [26], decreased liver fibrosis progression, and reduced HCC risk in a dose-dependent manner in both Veteran and Taiwanese insurance cohorts [14,27]. These studies suggested that statin use may have a protective effect against liver cancer in patients with hepatitis C infection. In the present study, we found that statin use reduced the risk of HCC in patients with HLP and CHC after the failure of antiviral therapy.
Several studies have explored the association between metformin use and HCC risk in patients with CHC and DM. A systematic review of 12 studies indicated that metformin might have a protective effect against HCC in patients with DM [12]. A large nationwide Taiwanese study showed that metformin use was linked to a lower HCC risk in a dose-dependent manner in patients with type 2 DM and chronic liver disease [28]. These studies suggested that metformin may exert a protective effect against HCC in patients with CHC and diabetes. Furthermore, our previous study documented that after achieving SVR, LC, and metformin non-use in patients with DM and CHC may result in a higher risk of HCC [13]. Similarly, we also observed a chemopreventive effect of metformin on the risk of HCC development in patients who failed antiviral therapy. Another interesting viewpoint is that among these patients, the HCC risk in the DM metformin use group initially appears lower than in the non-DM group but later aligns with it. This trend implies that the timing and effectiveness of metformin usage may vary. Maybe metformin had a real chemopreventive effect at an earlier period, but it was discontinued later due to progression or uncontrolled diabetes, and the effect faded, resulting in a comparable HCC risk as non-DM. Further validation is needed for these findings.
Our clinical findings revealed that unfavorable DM metformin non-use and favorable HLP statin use were critical in reducing the risk of HCC among patients with CHC after antiviral therapy failed. Several studies have investigated the effects of combination therapy with simvastatin (a statin) and metformin on the growth and migration of different cancer cells, including HBV-related HCC [29] and prostate cancer [30,31]. One study found that simvastatin and metformin inhibited the growth of HBV-related HCC cells by upregulating autophagy [29]. Combining simvastatin with metformin induced G1-phase cell cycle arrest and Ripk1- and Ripk3-dependent necrosis in C4-2B osseous metastatic castration-resistant prostate cancer cells. The synergistic effects of simvastatin and metformin on osseous metastatic castration-resistant prostate cancer cells suggest that this combination may be a promising treatment option for this type of cancer [30,31].
After HCV infection, host factors, such as older age and fibrosis progression leading to LC, appear to be significant in the development of HCC [9,32-34]. Coexisting conditions such as DM, obesity, and co-infection with HBV or HIV may accelerate the development of HCC [35,36]. Conversely, successful antiviral therapy has been associated with a reduced risk of HCC [3,37]. In this study, we observed that older age, advanced fibrosis, and LC were the independent risk factors for HCC. Exploring chemopreventive approaches, such as using favorable HLP statins and unfavorable DM metformin nonuse among patients with CHC in whom antiviral therapy has failed, may present another opportunity to decrease the risk of HCC.
Our study had several limitations that merit attention. Firstly, the specific impact of the duration, dosage, continuity, and timing of metformin and statin use on the incidence of HCC remains to be determined. Secondly, our analysis did not differentiate between the effects of lipophilic and hydrophilic statins, nor did it consider the potential influence of other OHAs such as sulfonylureas, thiazolidinediones, and DPP4 inhibitors on HCC incidence. Thirdly, we had no information on interferon preparations, specifically pegylated interferon α-2a versus α-2b, in this study.
Despite these limitations, which make further analysis challenging, our research offers significant insights in the era of DAAs for a small subset of patients who do not achieve SVR with DAAs [38], are non-compliant with treatment [39], or have contraindications to DAAs [40]. Additionally, this study on the chemopreventive effects of metformin and statins on HCC risk could serve as a benchmark for future research on the long-term risk of HCC among HCV patients and other patients with active liver diseases.
In summary, both metformin for DM and statins for HLP had chemopreventive effects on HCC risk in patients with CHC in whom antiviral therapy failed. These findings underscore the importance of implementing personalized preventive strategies to manage patients with these clinical profiles.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement1
Supplement1 Print
Print





