


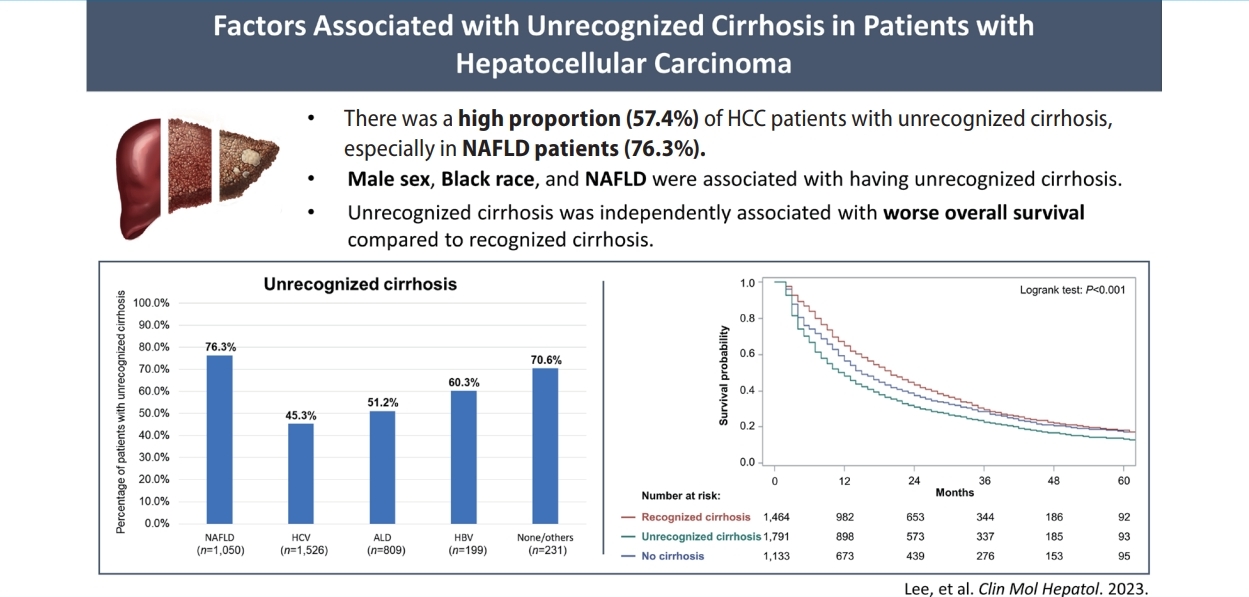
Graphical Abstract
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary liver cancer worldwide [1,2]. Cirrhosis caused by any etiology is the most important risk factor of HCC, and over 90% of patients with HCC in the Western world have underlying cirrhosis [1,3]. Professional society guidelines recommend patients with cirrhosis undergo semiannual surveillance for HCC [4-6]. A systematic review of cohort studies highlighted a consistent association between HCC surveillance and improved clinical outcomes, including early tumor detection and HCC mortality [7].
However, HCC surveillance is underused in clinical practice related to patient- and provider-level barriers [8]. Although there are failures at multiple steps in the cancer screening continuum [9-11], one common failure is under-recognition of cirrhosis [12-15]. Early compensated cirrhosis is often asymptomatic and can be undiagnosed for years, particularly given a lack of systematic screening for cirrhosis [16]. Patients with unrecognized cirrhosis are not enrolled in HCC surveillance programs so can experience late-stage HCC detection and worse survival [17].
Identifying factors associated with under-recognition of cirrhosis can help target intervention strategies, such as increased use of non-invasive markers of fibrosis. A prior retrospective cohort study from the Veterans Administration (VA) reported nonalcoholic fatty liver disease (NAFLD) is associated with a 4.8-fold increased risk of unrecognized cirrhosis [17]. However, it is unclear if these data are generalizable to non-VA populations given differences in patient populations as well as practice patterns.
Herein, we aimed to characterize the frequency and associated factors of unrecognized cirrhosis and its impact on overall survival in a national sample of patients with HCC from the United States.
MATERIALS AND METHODS
Study population
HCC patient data were extracted from the SEER-Medicare Linked Database, which linked data on incident cancer cases from SEER program’s 18 cancer registries to data from Medicare, the primary health insurer for individuals aged 65 years and older [18]. The inclusion criteria for HCC cases were (1) International Classification of Diseases (ICD)-Oncology-3 codes, site: C22.0 AND histology: 8170–8175, AND (2) adults ≥68 years of age, AND (3) HCC was diagnosed between 2011 and 2015. The reason for limiting the study cohort to adults ≥68 years of age is to ensure a 3-year follow-up period after Medicare enrollment for identifying potential risk factors and etiologies for HCC. The exclusion criteria (Supplementary Fig. 1) were (1) HCC cases diagnosed only based on death certificate without microscopic confirmation (n=437), OR (2) HCC cases from Medicare Part A and B enrollment with fewer than 3-year follow-up after Medicare enrollment, or HCC cases with fewer than 6-month follow-up after HCC diagnosis (n=1,886), OR (3) HCC cases from Medicare health maintenance organizations (HMOs) enrollment (n=3,487). We excluded HCC cases from Medicare HMOs because Medicare HMOs plans were not required to submit individual claims information to the Centers for Medicare and Medicaid Services, which might introduce bias to subsequent analyses.
Cirrhosis was defined based on ICD-9 or 10 codes from Medicare claims [19], or presence of cirrhosis complications including ascites, hepatic encephalopathy, esophageal varices, etc (Supplementary Table 1) [20]. If cirrhosis was diagnosed within 6 months immediately preceding HCC diagnosis, or after HCC diagnosis, cases were categorized as “unrecognized cirrhosis.” Etiology of HCC was defined based on ICD-9 or 10 codes [20].
For overall survival (OS) analyses, we excluded HCC cases without follow-up after diagnosis OR HCC cases who died at the same calendar month of HCC diagnosis (i.e., 0-month follow-up, Supplementary Fig. 1) (n=710).
Study variables
Demographic and clinical variables including sex, age, race/ethnicity (categorized as non-Hispanic White, non-Hispanic Black, non-Hispanic Asian/Pacific Islander [API]/Others, and Hispanic), regions stratified by poverty level (as determined by United States Census data), rural-urban regions (level of metropolitan and nonmetropolitan based on the United States Department of Agriculture Economic Research Service definition), National Cancer Institute (NCI) Comorbidity Index, liver disease etiology, and the presence of diabetes, ascites, and hepatic encephalopathy were included in this study.
To calculate the NCI Comorbidity Index for representing the noncancer comorbidity, we applied the ICD diagnosis and procedure codes one year before HCC diagnosis [21]. To avoid collinearity in the subsequent multivariable analyses, the NCI Comorbidity Index for HCC patients was calculated after excluding liver disease and diabetes [20]. To determine the etiology of HCC, Medicare claims ICD-9 or 10 codes for hepatitis C virus (HCV), hepatitis B virus (HBV), alcoholic liver disease (ALD), NAFLD, and others were used. We classified patients with ICD-9 or 10 code for obesity, diabetes, history of bariatric surgery or both dyslipidemia and hypertension in the absence of HBV, HCV, alcohol abuse, and other known liver disease as NAFLD since NAFLD is often under-coded [20]. For patients with ≥ two etiologies, the etiology was assigned by the following hierarchy: HCV>HBV>ALD>others>NAFLD. The ICD-9 or 10 codes for defining chronic liver diseases, diabetes, and complications related to cirrhosis were provided in Supplementary Table 2 and Supplementary Table 3, respectively.
The variables of tumor stage and treatment type were included in the OS analyses. We defined early-stage HCC as a single tumor, less than or equal to 5 cm in diameter without vascular invasion or extrahepatic metastasis since SEER-Medicare Linked Database only categorizes tumor number as unifocal or multifocal [20]. Treatments were stratified as potentially curative treatments (liver resection, liver transplantation, and tumor ablation) and non-curative treatments (chemoembolization, radioembolization, other radiation, systemic treatment, and others/best supportive care) [20].
Statistical analysis
Demographic and clinical variables among patients with unrecognized cirrhosis, recognized cirrhosis, and no cirrhosis were compared using chi-square test for categorical variables and one-way analysis of variance test for continuous variable (i.e., age). Factors associated with unrecognized cirrhosis were identified using univariate and multivariable logistic regression analyses. OS probabilities of HCC patients stratified by cirrhosis status were estimated using the Kaplan-Meier method and compared using the log-rank test. Factors associated with OS were evaluated using univariate and multivariable Cox regression analyses.
All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA) and Stata 16.1 (StataCorp, College Station, TX, USA) software with two-sided tests and a significance level of 0.05.
RESULTS
Clinical characteristics
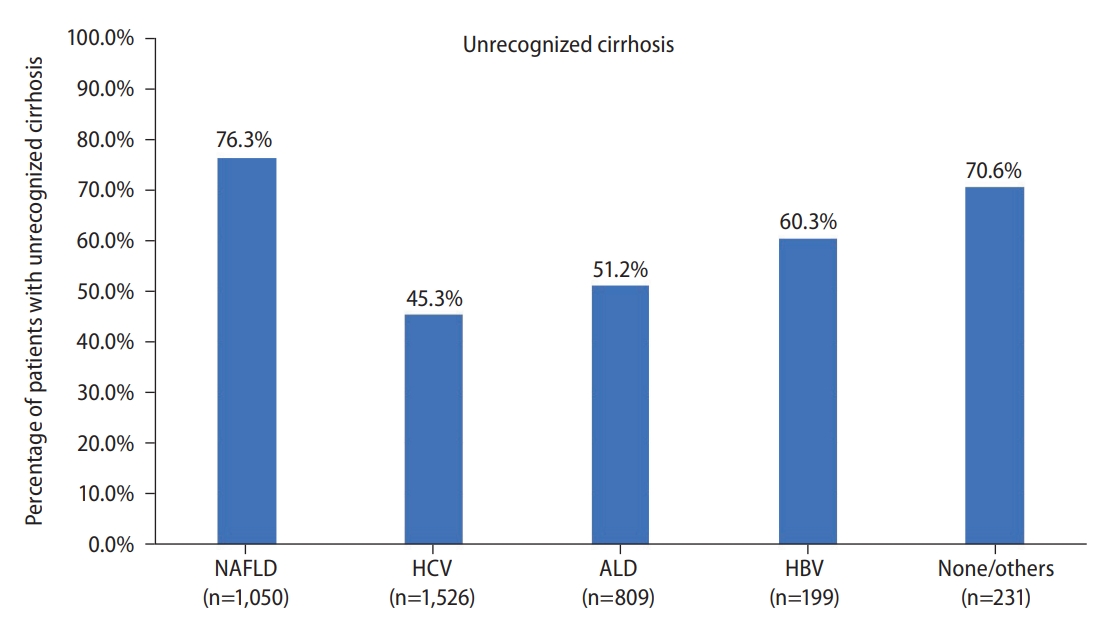
We identified 5,098 eligible patients with HCC, of whom NAFLD (35.6%) was the leading underlying etiology, followed by HCV (33.6%), ALD (17.6%), other/no etiologies (8.4%), and HBV (4.8%). A total of 3,815 patients with HCC (74.8%) were diagnosed with underlying cirrhosis, although there was a wide variation between etiologies (89.0% HCV, 80.9% HBV, 90.4% ALD, 57.9% NAFLD, and 53.8% other/no etiologies).
Among patients with cirrhosis, 2,190 patients (57.4%) had unrecognized cirrhosis. The clinical characteristics of HCC patients with recognized cirrhosis, unrecognized cirrhosis, and no cirrhosis were summarized in Table 1. Compared to those with recognized cirrhosis, a higher proportion of patients with unrecognized cirrhosis were older, male, non-Hispanic Black, and had underlying NAFLD. In fact, 76.3% of patients NAFLD and 70.6% of those with other etiologies had unrecognized cirrhosis at HCC diagnosis (Fig. 1).
Factors associated with unrecognized cirrhosis
Among HCC patients with cirrhosis, univariate logistic regression analysis revealed older age, male sex, living in nonmetro/rural counties, and NAFLD etiology as being associated with greater odds of having unrecognized cirrhosis, while Hispanic ethnicity and higher NCI comorbidity index were associated with lower odds of unrecognized cirrhosis (Table 2). In multivariable logistic regression analysis, older age (adjusted odds ratio [aOR]: 1.04, 95% confidence interval [CI]: 1.03–1.05), male sex (aOR: 2.12, 95% CI: 1.83–2.46), non-Hispanic Black race (reference: non-Hispanic White; aOR: 1.93, 95% CI: 1.45–2.57), and NAFLD etiology (reference: HCV; aOR: 4.46, 95% CI: 3.68–5.41) were associated with unrecognized cirrhosis (Table 2). Conversely, Hispanic ethnicity (aOR: 0.79, 95% CI: 0.65–0.96), higher NCI comorbidity index (aOR: 0.72, 95% CI: 0.57–0.90), and diabetes (aOR: 0.73, 95% CI: 0.63–0.85) were inversely associated with having unrecognized cirrhosis in multivariable analysis (Table 2).
Subgroup analysis was performed to further identify factors associated with unrecognized cirrhosis among cirrhotic patients with NAFLD-related HCC. Male sex (aOR: 2.32, 95% CI: 1.71–3.14) and older age (aOR: 1.03, 95% CI: 1.00–1.05) was associated with unrecognized cirrhosis, while higher NCI comorbidity index (aOR: 0.58, 95% CI: 0.39–0.86) was inversely associated (Table 3).
Association between unrecognized cirrhosis and overall survival
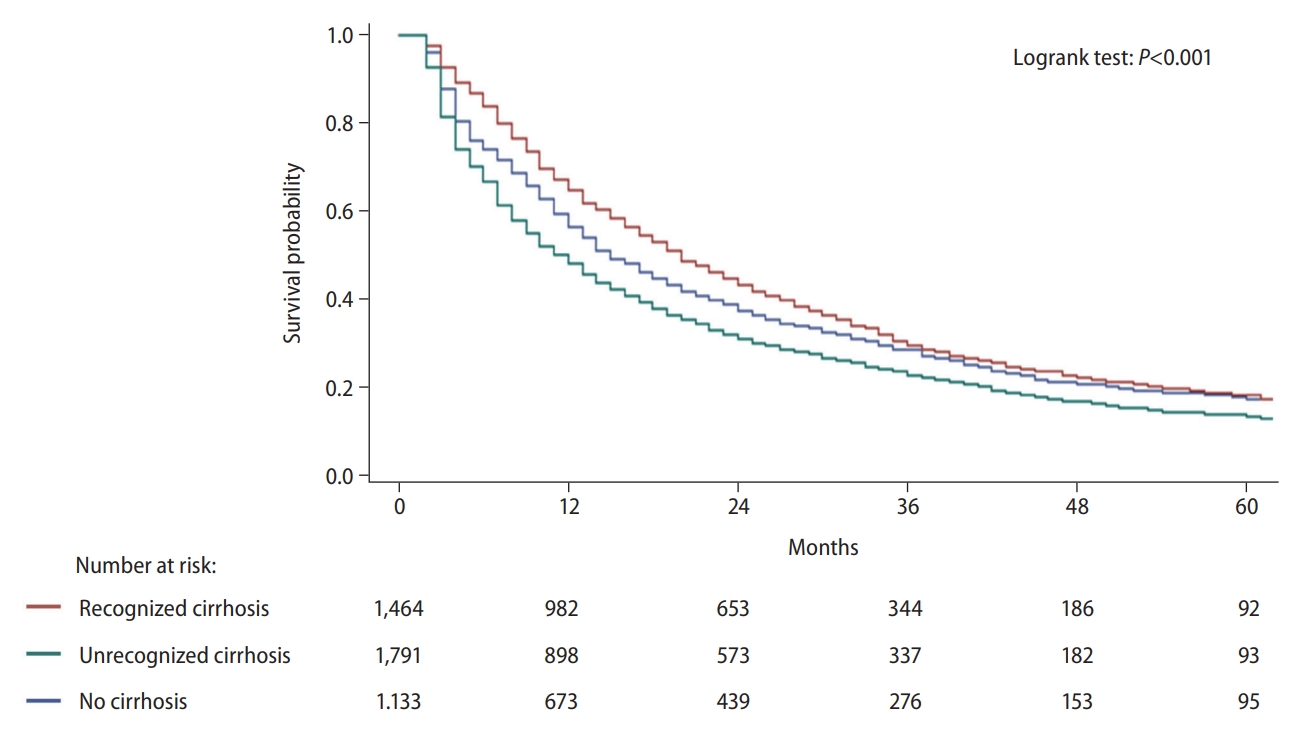
Compared to patients with recognized cirrhosis, significant lower proportion of patients with unrecognized cirrhosis were presented with early-stage HCC (13.7% vs. 29.9%) and underwent potentially curative treatments (19.9% vs. 29.2%) (Table 1). Median OS were 20 months (interquartile range [IQR]: 9–43 months), 12 months (IQR: 4–33 months), and 15 months (IQR: 6–41 months) for patients with recognized cirrhosis, unrecognized cirrhosis, and no cirrhosis, respectively (P<0.001; Fig. 2). In multivariable Cox regression analysis adjusting for the demographic and clinical variables, tumor stage, and treatment type (Table 4), unrecognized cirrhosis was independently associated with worse OS (adjusted HR [aHR]: 1.17, 95% CI: 1.08–1.27) compared to recognized cirrhosis, while patients with no cirrhosis had favorable OS (aHR: 0.84, 95% CI: 0.76–0.93).
DISCUSSION
We investigated the frequency and associated factors for unrecognized cirrhosis among patients with cirrhosis and HCC using a large United States Medicare-based database. We found over 50% of HCC patients had unrecognized cirrhosis prior to HCC diagnosis, including three-fourths of those with NAFLD-related HCC. Older age, male sex, Non-Hispanic Black race, and NAFLD etiology were independently associated with greater odds of unrecognized cirrhosis, while Hispanic ethnicity, higher comorbidity, and diabetes were associated with lower odds of having unrecognized cirrhosis. Lastly, our study confirmed that HCC patients with unrecognized cirrhosis were associated with worse survival than those with recognized cirrhosis.
In line with the findings in the previous VA study [17], we showed that NAFLD was associated with a more than fourfold increased likelihood of having unrecognized cirrhosis compared to HCV. A recent study showed that only 4.4% of patients with NAFLD in the United States were aware of their liver disease, much lower than the percentages of patients with HCV (42.4%) and HBV (17.2%) [22]. The low awareness of liver diseases among patients with NAFLD could be attributed to the insufficient understanding of NAFLD for both the general population and non‐hepatologist physicians [23]. Considering the increasing burden of NAFLD in the world [24,25], American Association of Clinical Endocrinology and American Association for the Study of Liver Diseases recently provided a clinical practice guideline for diagnosis and management of NAFLD to prevent the development of liver cirrhosis and related comorbidities [26,27]. The guideline suggests using liver fibrosis prediction calculations (e.g., Fibrosis-4) to initially assess the risk of advanced liver fibrosis in NAFLD patients, and triage the high-risk patients for fibrosis/cirrhosis screening by transient elastography. With increased availability of non-invasive biomarkers of fibrosis and transient elastography, the guideline will potentially increase recognition of NAFLD-related cirrhosis, especially for primary care physicians and endocrinologists who often look after NAFLD patients.
In overall and NAFLD subgroup analyses, we observed sex differences with the male having more than a two-fold increased likelihood of having unrecognized cirrhosis, which could arise from the variance of adherence to regular follow-up with physician and screening test [15,28]. For example, a United States cohort study demonstrated females were more compliant with HCC surveillance than males [28]. More recently, a study exploring potential reasons for HCC screening underuse showed similar results, indicating that men were less likely to stick to regular outpatient care than women [15]. Even patients having regular outpatient care, failure of receiving ultrasound or noninvasive biomarkers for fibrosis might cause unrecognition of cirrhosis [15,29]. Further investigation is warranted to understand underlying causes of this sex difference.
We noted Non-Hispanic Black race was associated with increased likelihood of having unrecognized cirrhosis. Higher likelihood of having unrecognized cirrhosis in non-Hispanic Black patients may partly explain underlying racial ethnic disparity in HCC surveillance, curative treatment, and overall survival as reported in previous studies [20,30-33]. Consistent with other studies, our previous study using SEER-Medicare Linked Database showed that non-Hispanic Black race is inversely associated with HCC surveillance receipt, early stage HCC detection, and curative treatment receipt [20]. A comprehensive approach to monitoring and eliminating racial-ethnic disparities in early recognition of cirrhosis and surveillance implementation is urgently needed to reduce disparities in early HCC detection and prognosis. Other than demographic factors, we found that higher comorbidites and diabetes were associated with lower odds of having unrecognized cirrhosis. This could be explained by higher healthcare utilization in patients with comorbid conditions.
While under-recognition of cirrhosis is thought to be related to poor survival due to the lack of HCC surveillance, no study directly interrogates their association. The previous VA study showed HCC patients with unrecognized cirrhosis were 6.5 times more likely to be diagnosed with advanced stage HCC compared to with recognized cirrhosis [17], implying their unfavorable prognosis. Importantly, our study first confirmed the inferior survival of HCC patients with unrecognized cirrhosis, even after adjusting for tumor stage and treatment type. Therefore, earlier recognition of cirrhosis, particularly in the growing population of NAFLD patients will likely lead to improved overall survival after HCC diagnosis.
We acknowledge the inherent limitations of this retrospective study. First, compared to previous study by Walker et al. [17], where a systematic electric chart review was performed, use of ICD-9 and ICD-10 codes in our current study to define cirrhosis and the underlying etiology of HCC could have led to misclassification. For example, some cirrhosis cases may have been recognized but could have been undercoded; codes for cirrhosis were not assigned within 6 months preceding HCC diagnosis may not guarantee the unrecognition of cirrhosis. However, consistency of the findings between ours and Walker et al. [17] confirmed the validity of the results. Secondly, Medicare population represents older individuals, and the study results might not be generalizable to younger patients with HCC. In addition, the stringent inclusion and exclusion criteria of this study might introduce selection bias. For instance, since most of the patients with HBV- or HCV-related HCC were diagnosed and deceased before 70 years old [34,35], patients with NAFLD-related HCC might have been overrepresented and burdern of unrecognized cirrhosis could have been overestimated in the current study. Lastly, missing data on Child-Pugh score prevent us from performing granular subgroup analyses.
Despite these limitations, our study has the strength of including nationwide population compared to the previous study [17]. We first confirmed the findings (i.e., NAFLD, Black race, and age are associated unrecognized cirrhosis) from the previous study [17] in a larger cohort outside VA system. In addition, the majority of patients in the previous study had HCV-associated HCC [17], while few HCC patients with NAFLD were included [17]. Our study included more balanced etiologies and 1,813 HCC patients had NAFLD, which could represent the trends of global rise of HCC patients attributed to NAFLD. Lastly, we enrolled the HCC patients diagnosed between 2011–2015, which follows the period (2005–2011) of the previous study [17], highlighting the issue of unrecognized cirrhosis remains unsolved and requires immediate intervention.
In summary, our results highlight that unrecognition of cirrhosis remains a common barrier to effective HCC surveillance implementation in the United States, particularly among patients with NAFLD-related HCC. We also validated the independent association between unrecognized cirrhosis and poor prognosis. Future studies and efforts are required to evaluate intervention strategies to better recognize cirrhosis at early stages to promote increased uptake of HCC surveillance programs and improve patients’ outcomes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement1
Supplement1 Print
Print





